pd apparatus solutions transfer set connectologies acess for pd ,catheter and exit site care in detail
show info here
🫁 Peritoneal Dialysis (PD) - Complete Clinical Reference
1. PD APPARATUS - OVERVIEW
Key Components of the PD System:
| Component | Description |
|---|---|
| PD catheter | Silicone or polyurethane tube; Tenckhoff type most common |
| Transfer set / tubing | Connects catheter to dialysate bags |
| Dialysate bags | Contain osmotic agent, electrolytes, buffer |
| Cycler (APD) | Automated machine for overnight exchanges |
| Drainage bag | Collects spent dialysate (effluent) |
| Clamps, caps, connectors | Maintain sterility during exchanges |
2. PD SOLUTIONS (DIALYSATE)
Composition of PD Fluid:
- Electrolytes - sodium, calcium, magnesium, chloride
- Buffer - lactate (standard) or bicarbonate (biocompatible)
- Osmotic agent - to drive ultrafiltration
- Water as carrier
Osmotic Agents Compared:
| Feature | Dextrose (Glucose) | Icodextrin | Amino Acid |
|---|---|---|---|
| Mechanism | Crystalloid osmosis | Colloid osmosis | Osmotic + nutritional |
| Concentration | 1.5%, 2.5%, 4.25% | 7.5% | 1.1% |
| Duration | Short dwells (4-6 hrs) | Long dwells (8-12 hrs) | Long dwells |
| UF achieved | Dwell-time dependent | Sustained (no glucose dissipation) | Modest |
| Concern | Glucose absorption, peritoneal fibrosis | Maltose accumulation | Amino acid load |
| Best use | Standard CAPD exchanges | Overnight APD/long dwell | Malnourished patients |
Key Physiology:
- At dwell time 0: glucose concentration is highest → maximum osmotic pressure → highest ultrafiltration rate
- Over time, ~2/3 of glucose is absorbed within 4 hours → osmotic gradient falls → UF diminishes
- Icodextrin (a glucose polymer) is NOT absorbed via aquaporins → maintains colloid osmotic pressure for long dwells
- 50% of transcapillary UF occurs through aquaporin-1 (AQP-1) ultra-small pores
Solution Types by pH/Buffer:
| Type | Buffer | pH | Features |
|---|---|---|---|
| Conventional | Lactate | Low (5.2-5.5) | Standard; peritoneal membrane toxic long-term |
| Bicarbonate | Bicarbonate | Physiologic (7.0-7.4) | Biocompatible; less painful on infusion |
| Bicarbonate/Lactate | Mixed | ~7.0 | Balanced; better membrane preservation |
Long-term exposure to lactate-acid solution and high glucose damages the peritoneal membrane, leading to loss of mesothelial microvilli, reduced anionic charges, and eventually encapsulating peritoneal sclerosis (EPS).
3. PD MODALITIES
| Modality | Full Name | Description |
|---|---|---|
| CAPD | Continuous Ambulatory PD | Manual; 3-5 exchanges/day; no machine |
| APD | Automated PD | Machine (cycler); exchanges overnight |
| NIPD | Nightly Intermittent PD | APD at night; no daytime dwell; used when residual renal function is good |
| CCPD | Continuous Cycling PD | APD overnight + one daytime exchange |
| TPD | Tidal PD | Never fully drains; a reserve volume left; faster cycles |
4. TRANSFER SET & CONNECTOLOGY
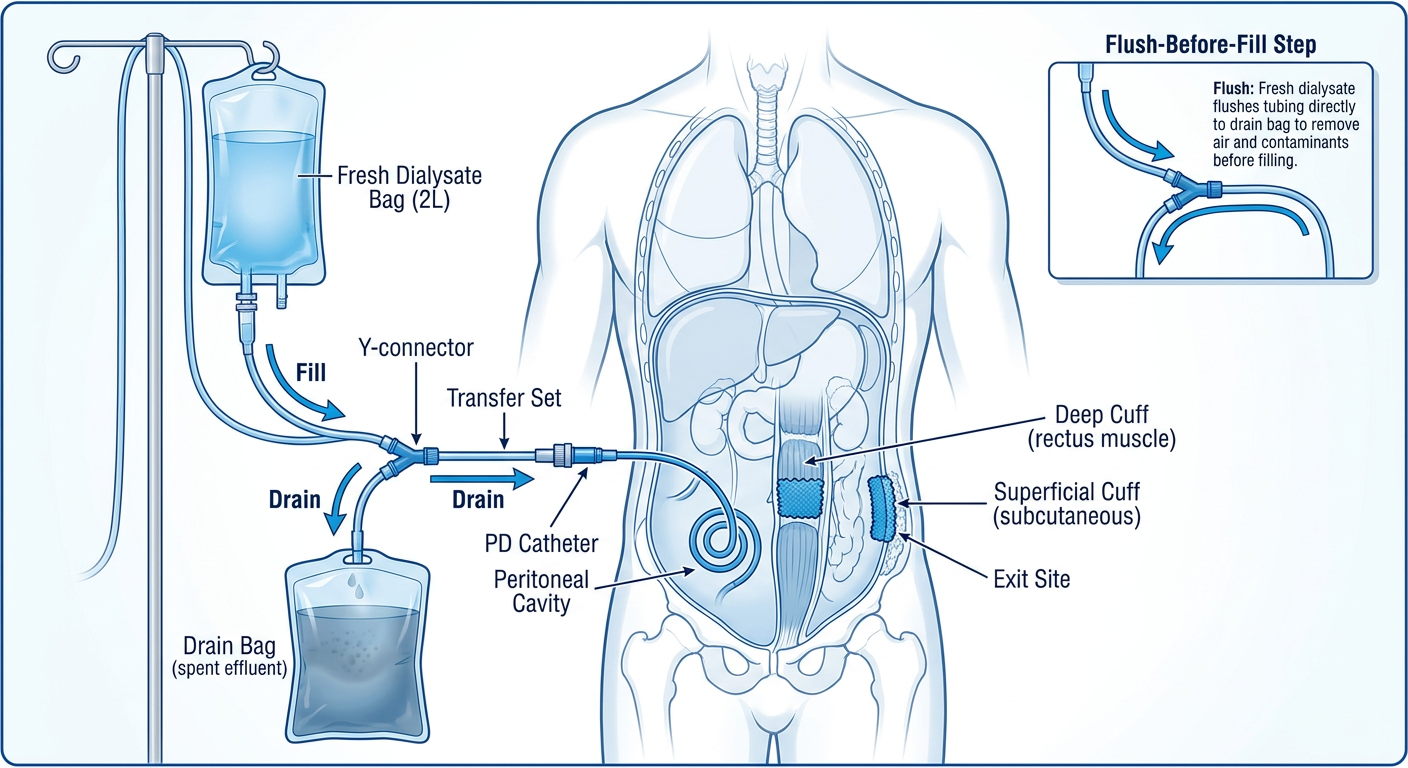
The Y-Set System ("Flush-Before-Fill" Technique):
Fresh dialysate bag
|
Y-connector
/ \
Drain bag PD Catheter (patient)
- Connect Y-set to PD catheter
- Drain spent dialysate from peritoneum into drain bag first
- Flush - briefly run fresh dialysate through the Y-set into the drain bag (flushes any touch contaminants out)
- Fill - infuse fresh dialysate into peritoneum
- Disconnect; cap catheter
The "flush-before-fill" design dramatically reduced coagulase-negative Staphylococcus (CoNS) peritonitis by flushing away organisms that may have entered during connection.
Connectology Principles:
- Spike connector or Luer-lock system used depending on manufacturer (Baxter, Fresenius)
- Sterile technique at all connection/disconnection steps is mandatory
- Titanium adapter or transfer set adapter connects catheter to exchange tubing
- Transfer sets are changed every 6 months (or per manufacturer protocol)
- All connections must use aseptic technique: mask worn by patient and assistant
- Clamps must be closed before disconnecting any part of the circuit
- Inspect bags for cloudiness, leaks, or particulate matter before each use
CAPD vs APD Connectology:
| CAPD | APD | |
|---|---|---|
| Connection | Manual Y-set or spike | Cycler tubing cassette |
| Frequency | 3-5×/day | 1× (overnight setup) |
| Sterile breaks | Multiple per day | Single nightly connection |
| Peritonitis risk | Slightly higher | Slightly lower |
5. PERITONEAL DIALYSIS ACCESS - THE CATHETER
Types of PD Catheters:
| Feature | Options |
|---|---|
| Material | Silicone rubber (most common) or polyurethane |
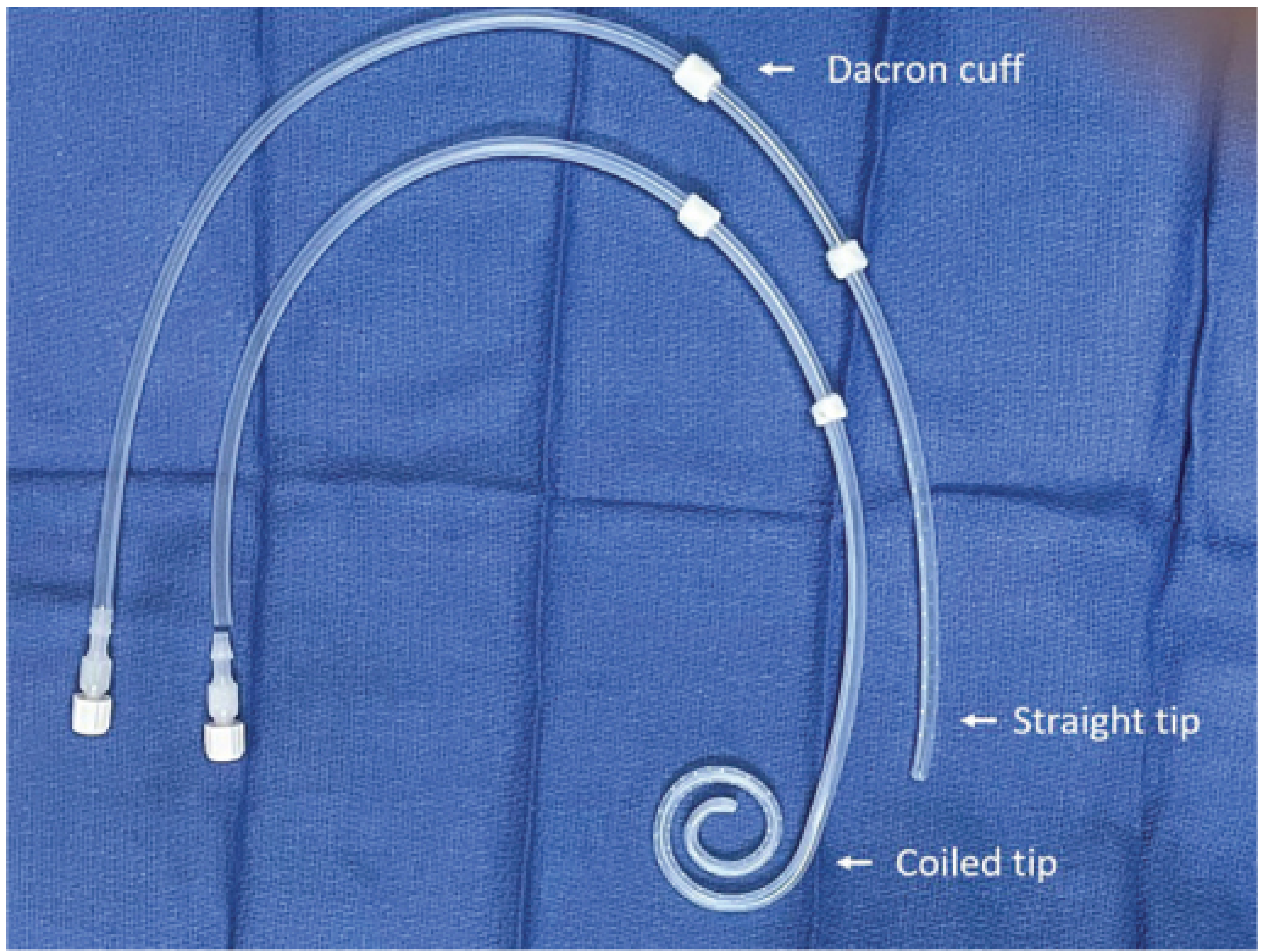
| Intraperitoneal portion | Straight, coiled (preferred), Ash/T-Fluted, silicone disc |
| Extraperitoneal portion | Straight or swan-neck design |
| Cuffs | Single or double (double preferred) |
Most Widely Used: Double-cuff, Swan-neck, Coiled Tenckhoff Catheter
- Coiled tip → less pain on infusion, less catheter migration, fewer outflow problems
- Swan-neck → downward-pointing exit site → prevents cuff extrusion, reduces infection
- Double cuffs → inner cuff in rectus muscle (prevents leaks); outer cuff in subcutaneous tissue (blocks external bacterial migration)
Catheter Placement Techniques:
| Technique | Notes |
|---|---|
| Blind (Seldinger) | Bedside; fast; higher risk |
| Surgical (open) | Best visualization; gold standard |
| Peritoneoscopic | Better survival rates; direct visualization |
| Laparoscopic | Best for complex cases; allows omentopexy |
| Fluoroscopic | With or without real-time ultrasound |
| Moncrief-Popovich | Catheter buried subcutaneously; externalized later |
Peritoneoscopic placement has been shown to have longer catheter survival compared to blind technique.
Cuff Placement:
- Inner (deep) cuff → placed within the rectus abdominis muscle (prevents leaks and peritoneal fluid tracking)
- Outer (superficial) cuff → placed in subcutaneous tissue, 2-4 cm from skin exit site → dead space between cuffs blocks bacteria tracking inward
- Ingrowth of fibrous tissue into both cuffs provides secure fixation and allows water immersion (bathing/swimming)
Exit Site Positioning:
- Exit site should face downward and laterally
- Determined with patient in upright position before insertion
- Avoid: beltline, prior surgical scars, abdominal midline
- Special situations: presternal exit site - used in obese patients, patients with ostomies, or incontinent children - shown to decrease peritonitis and exit-site infection, with catheter survival up to 95% at 2 years
6. CATHETER CARE - POST-INSERTION
Immediate Post-Operative Care:
- Cover with non-occlusive dressing
- Catheter should NOT be used for 10-14 days post-placement
- Flush catheter with saline or dialysate 2-3 times/week until PD starts
- PD typically started 2-4 weeks after placement (allows wound healing + cuff ingrowth)
- Urgent-start PD (within 24 hours) may be attempted with low-volume exchanges if no other access is available
Ongoing Catheter Care:
- Immobilize the catheter with tape or catheter securement device to prevent traction on exit site
- Never pull or tug on the catheter
- Inspect for signs of infection at every encounter
- Prophylactic antibiotics at time of catheter insertion (first-generation cephalosporin or glycopeptide based on local microbiology)
7. EXIT SITE CARE
Definition of Exit Site:
Routine Exit Site Care Protocol:
- Wash hands thoroughly before touching the catheter
- Clean exit site daily with antiseptic solution (chlorhexidine or normal saline per center protocol)
- Apply topical antibiotic daily:
- Mupirocin (Bactroban) cream/ointment - reduces Staphylococcus aureus exit-site infections
- Gentamicin cream - alternative; also covers gram-negative organisms (especially Pseudomonas)
- Apply sterile dressing and secure catheter
- Avoid submersion in non-chlorinated water (lakes, ponds, baths) - showers preferred
Exit Site Infection (ESI) - Recognition:
| Feature | Healthy Exit Site | Infected Exit Site |
|---|---|---|
| Appearance | Pink, well-healed | Redness, swelling, crusting |
| Discharge | None or serous | Purulent / cloudy |
| Pain | None | Tenderness |
| Granulation | Minimal | Excessive (sign of chronic irritation) |
Exit Site Infection - Common Organisms:
- Staphylococcus aureus - most common
- Pseudomonas aeruginosa - associated with higher risk of catheter loss
- Coagulase-negative Staphylococci
- Gram-negative rods
Tunnel Infection:
- Infection tracking along the subcutaneous catheter tunnel
- Presents as pain/tenderness/redness along the tunnel tract
- Diagnosed by ultrasound (shows fluid/edema around catheter)
- If tunnel infection reaches inner cuff → catheter removal often required
- Tunnel + exit site infection → treat aggressively with systemic antibiotics; catheter removal if no improvement in 2-3 weeks
Prevention of Exit Site Infection:
| Measure | Details |
|---|---|
| Daily topical antibiotic | Mupirocin or gentamicin at exit site |
| Proper catheter immobilization | Prevents trauma and micro-motion |
| Downward-facing exit site | Gravity prevents fluid pooling |
| Patient training | Technique reviewed at every visit; retrained after any infection |
| Prophylactic antifungal | When antibiotics given for any reason (prevents fungal peritonitis) |
| Avoid contamination | No touching catheter with dirty hands; mask worn during exchanges |
8. PERITONITIS - OVERVIEW (Linked to Access/Exit Site Care)
Routes of Entry:
- Intraluminal - touch contamination during exchange (most common)
- Periluminal - bacteria tracking along outside of catheter from exit site
- Transmural - bowel flora translocating across intestinal wall
- Hematogenous - transient bacteremia seeds peritoneum
- Transvaginal - organisms via female reproductive tract
- Fungal - in immunocompromised or post-antibiotic patients
Diagnosis (2 of 3 criteria required):
- Organisms on Gram stain/culture of effluent
- Cloudy fluid (WBC >100/mm³, >50% neutrophils)
- Clinical signs of peritoneal inflammation + cloudy fluid + abdominal pain
Impact of Y-Set on Peritonitis:
The introduction of the Y-set and flush-before-fill technique led to a dramatic decrease in CoNS peritonitis rates globally - one of the most significant improvements in PD management.
9. COMPLICATIONS OF CATHETER/ACCESS
| Complication | Description | Management |
|---|---|---|
| Catheter migration | Tip moves out of pelvis | Laxatives; laparoscopic repositioning |
| Omental entrapment | Omentum wraps catheter | Omentopexy at time of insertion; laparoscopic release |
| Outflow failure | Drainage stops | Fibrinous sheath disruption by guidewire |
| Leaks | Fluid leaking at insertion site | Early low-volume PD; surgical repair |
| Cuff extrusion | Outer cuff pushes through skin | Shaving/trimming or catheter replacement |
| Fibrinous sheath | Catheter encased in fibrin | Guidewire disruption or exchange |
| Encapsulating peritoneal sclerosis (EPS) | Late complication; membrane fibrosis | Cessation of PD; surgery if severe |
10. SUMMARY TABLE - PD SYSTEM AT A GLANCE
| Element | Key Point |
|---|---|
| Best catheter | Double-cuff, swan-neck, coiled Tenckhoff |
| Cuff positions | Inner = rectus muscle; Outer = subcutaneous (2-4 cm from exit) |
| Exit site direction | Downward and lateral |
| Best connection system | Y-set with flush-before-fill |
| Standard dialysate | Dextrose-based, lactate-buffered |
| Long dwell agent | Icodextrin (colloid osmosis via AQP-1 bypass) |
| Daily exit site antibiotic | Mupirocin or gentamicin cream |
| When to start PD | 2-4 weeks post-insertion |
| Transfer set change | Every 6 months |
| Peritonitis diagnosis | 2 of 3 ISPD criteria |
pd therapies intermittent and continuous in detail
Peritoneal Dialysis Therapies - Intermittent & Continuous: Complete Reference
1. THE THREE FUNDAMENTAL STEPS OF EVERY PD EXCHANGE
FILL → DWELL → DRAIN
| Step | Description | Clinical Significance |
|---|---|---|
| Fill (Infusion) | Sterile dialysate instilled into peritoneal cavity | Volume typically 1.5-3 L; coiled catheter reduces infusion pain |
| Dwell | Fluid remains in peritoneum | Diffusion + ultrafiltration occur across peritoneal membrane |
| Drain (Effluent) | Spent dialysate drained out | First 1.6-1.8 L drains rapidly; slows as residual volume falls below 300 mL |
The entire exchange (instillation + drainage) should not exceed 30 minutes in a functioning catheter.
2. CLASSIFICATION OF PD MODALITIES
PD THERAPIES
│
├── CONTINUOUS (peritoneum always filled with dialysate)
│ ├── CAPD – Continuous Ambulatory PD (manual)
│ ├── CCPD – Continuous Cycling PD (APD + daytime dwell)
│ └── CFPD – Continuous Flow PD (experimental)
│
└── INTERMITTENT (peritoneum has dry/empty periods)
├── IPD – Intermittent PD (classic/acute)
├── NIPD – Nightly Intermittent PD (APD, dry day)
└── TPD – Tidal PD (partial drain variant)
3. CONTINUOUS THERAPIES
A. CAPD - Continuous Ambulatory Peritoneal Dialysis
| Feature | Detail |
|---|---|
| Type | Manual; no machine |
| Exchanges/day | Typically 3-5 per day (most common: 4 exchanges) |
| Dwell volume | 2.0-2.5 L per exchange (range 1.5-3 L) |
| Daytime dwells | 3-4 exchanges, each 4-6 hours dwell time |
| Overnight dwell | 1 long dwell of 10-12 hours (icodextrin or high glucose used) |
| Total dialysis | 24 hours/day, 7 days/week - peritoneum always contains fluid |
| Equipment | Y-set / double-bag system only; no cycler needed |
| Cost | Lower ($$) |
Morning (6 AM) → Drain overnight dwell + Fill fresh bag [Exchange 1]
Midday (12 PM) → Drain + Fill [Exchange 2]
Afternoon (5 PM) → Drain + Fill [Exchange 3]
Bedtime (10 PM) → Drain + Fill with icodextrin/high glucose [Overnight dwell]
Next morning → Drain overnight + repeat cycle
- No machine - portable, travel-friendly
- Lower cost - important in low/middle-income countries
- Better for patients uncomfortable sleeping connected to a machine
- Easier for "fussy" catheters (can control drain speed)
- Preferred in cirrhosis/ascites (can control drain volume precisely)
- More confident with twin-bag technique training
- Better suited for low transporters (long dwell time maximizes diffusion)
- Multiple sterile connections per day = higher peritonitis risk vs APD
- Disruptive to daytime activities
- Higher risk of hernias, leaks, and back pain (constant intra-abdominal pressure day and night)
- Challenging beyond 4 exchanges/day - those patients better switched to APD
- Less flexible for working patients
B. CCPD - Continuous Cycling Peritoneal Dialysis
| Feature | Detail |
|---|---|
| Type | Automated (APD cycler) overnight + daytime dwell |
| Overnight exchanges | 3-5 cycles by cycler while patient sleeps (8-9 hrs) |
| Overnight dwell volume | 2.0-2.5 L per cycle |
| Daytime dwell ("last fill") | 1 long dwell remains in peritoneum during the day |
| Daytime dwell agent | Icodextrin (sustains osmosis for 8-16 hrs) or high glucose |
| Total dialysis | 24 hours/day, 7 days/week - peritoneum always filled |
| Connection frequency | Single nightly connection to cycler |
10 PM → Connect to cycler; cycler runs 3-5 automated exchanges overnight
6 AM → Cycler delivers final "last fill" (2 L icodextrin)
6 AM → Disconnect from machine; patient is FREE during day
10 PM → Drain last fill + reconnect cycler → repeat
- Single daily connection = fewer sterile breaks = lower peritonitis risk
- Daytime freedom (ideal for working patients, children in school)
- Lower risk of hernias and leaks if daytime is "dry" (no abdominal pressure during day)
- Lower risk of back pain
- Better for urgent-start PD (supine, low-volume cycling)
- Easier for assisted PD in elderly (carer connects once at night)
- Remote monitoring via cycler data transmission
- Cycler warms fluid before infusion (reduces shivering/discomfort)
- Better suited for high transporters (rapid short dwells maximize UF before glucose is absorbed)
- Higher cost ($$$$) - cycler, cartridges, specialized tubing
- Requires electricity and space
- Cycler alarms can disturb sleep
- Drain pain and low-drain alarms more common
- Less confident with twin-bag manual backup technique
- Challenging in cirrhosis/ascites management
4. INTERMITTENT THERAPIES
A. IPD - Intermittent Peritoneal Dialysis
| Feature | Detail |
|---|---|
| Type | Manual or automated; scheduled sessions |
| Frequency | 3× per week (like hemodialysis schedule) OR daily short sessions |
| Session duration | 8-12 hours per session |
| Dwell time | Short: 30-60 minutes per exchange |
| Exchanges per session | 10-24 rapid exchanges per sitting |
| Between sessions | Peritoneum is dry (empty) |
| Setting | Hospital/clinic-based; used in AKI |
- Peritoneum rests between sessions → reduced membrane exposure to glucose
- Lower intraperitoneal pressure most of the time → fewer hernias and leaks
- Feasible in acute kidney injury without formal catheter maturation
- Nurse-managed in hospital; no patient self-care required
- Least efficient of all PD modalities for solute clearance
- Requires frequent hospital attendance
- Short dwells may not achieve adequate equilibration with large solutes
- Not suitable as a long-term ESKD modality
- Cardiovascular instability can still occur with rapid fluid shifts
B. NIPD - Nightly Intermittent Peritoneal Dialysis
| Feature | Detail |
|---|---|
| Type | Automated (cycler) - nights only |
| Overnight exchanges | 3-5 cycles on cycler (8-10 hours) |
| Daytime | Abdomen dry - no fluid in peritoneum |
| Weekly Kt/V | Lower than CCPD; adequate only when RKF is preserved |
| Best patient | Those with significant residual kidney function (RKF) |
- Maximum daytime freedom with empty abdomen
- Lowest intraperitoneal pressure of any PD modality
- Lowest risk of hernias, leaks, and back pain
- Less glucose absorption (fewer hours of contact)
- Less peritoneal membrane exposure to glucose/lactate
- Reduced risk of hernia formation
- Insufficient for anuric patients - relies on RKF for additional clearance
- Lowest solute and fluid removal of all continuous/APD options
- As RKF declines, must transition to CCPD or add daytime dwell
- Short dwell times limit large-solute and middle-molecule removal
C. TPD - Tidal Peritoneal Dialysis
| Feature | Detail |
|---|---|
| Type | Automated (cycler); modified drain pattern |
| Mechanism | A reserve (tidal) volume is left in peritoneum after each drain |
| Tidal volume | Typically 70% TPD = drain 70% of fill volume; retain 30% |
| Example | For 2L fill: drain 1.4L, retain 0.6L; next fill is 1.4L |
| Final drain | Complete drain at end of session |
Fill: 2.0 L
Dwell: short
Drain: only 1.4 L drained (70%)
Retained: 0.6 L stays in peritoneum
Next fill: 1.4 L added (total 2.0 L again)
→ Repeat cycles → Full drain at end
- Originally designed to enhance diffusive clearance (results were disappointing - not used for this)
- Current main use: Management of low-drain alarms on the cycler
- Also used for patients with pain during inflow or drain phases
- Maintains continuous membrane contact → no "dead time" during refilling
- Does NOT significantly improve solute clearance over standard APD
- More complex prescription
- Higher dialysate volume usage = higher cost
5. INCREMENTAL PD - A MODERN APPROACH
Typical Incremental PD Prescriptions:
| Modality | Incremental Options |
|---|---|
| CAPD | 3 × 2L daily; 2 × 2L daily; 1 × 2L icodextrin only; 4-6 days/week |
| APD | No day dwell; 5 nights/week; 3 nights/week; 1.5L dwell volumes; 6 hours/night only |
- Reduces early workload - builds patient confidence gradually
- Lower cost (less dialysate)
- Less glucose exposure - protects peritoneal membrane
- Fewer mechanical complications early on
- May slow decline of RKF
- Personalized to patient lifestyle
From the CANUSA cohort: every 5 L/week/1.73m² of residual creatinine clearance = 12% lower relative risk of death. RKF provides middle-molecule removal, volume control, and metabolic benefits that peritoneal clearance alone cannot fully replace.
6. URGENT-START PD
| Feature | Protocol |
|---|---|
| Position | Supine dialysis (reduces leak risk) |
| Volume | Low-volume exchanges (1-1.5 L initially) |
| Modality | APD preferred (lower leak risk vs CAPD) |
| Dry periods | Dry abdomen when upright |
| Volume escalation | Gradually increase to full volume over 2-4 weeks |
| Also used for | AKI requiring urgent renal replacement |
7. PERITONEAL MEMBRANE TRANSPORT - MATCHING MODALITY TO PATIENT
The Peritoneal Equilibration Test (PET)
| Transport Type | D/P Creatinine at 4h | Glucose Absorption | Best Modality |
|---|---|---|---|
| High | >0.81 | Rapid | APD (short dwells; UF before glucose absorbed) |
| High-average | 0.65-0.81 | Moderate-fast | APD or CAPD |
| Low-average | 0.50-0.65 | Moderate-slow | CAPD |
| Low | <0.50 | Slow | CAPD (long dwells maximize diffusion) |
Important caveat (modern practice): While transport type theoretically guides modality choice, current guidelines recommend prescriptions be individualized to patient lifestyle and priorities, not solely dictated by transport kinetics. For example, a high transporter who works nights may still prefer CAPD.
8. PRESCRIPTION VARIABLES - WHAT TO SPECIFY FOR EVERY PD ORDER
| Variable | Options |
|---|---|
| 1. Dwell volume | 1.25-1.5 L/m² BSA; typically 2-3 L; start lower if recent surgery/hernia risk |
| 2. Dwell time | Short (APD: 1-2 hrs) to long (overnight: 10-12 hrs) |
| 3. Number of exchanges | CAPD: 3-5/day; APD: 3-5 cycles overnight |
| 4. Dextrose concentration | 1.5% (yellow), 2.5% (green), 4.25% (red) - colour-coded bags |
- 1.5% - minimal UF; euvolaemic patients
- 2.5% - moderate UF; mild volume overload
- 4.25% - maximum UF; significant volume overload; highest glucose load
9. DIALYSIS ADEQUACY - TARGET MEASURES
| Measure | Target | Notes |
|---|---|---|
| Weekly total Kt/V urea | ≥ 1.7 | Includes peritoneal + residual kidney Kt/V |
| Peritoneal creatinine clearance | ≥ 50 L/week/1.73m² | Some centers prefer this over Kt/V |
| Ultrafiltration | > 750 mL/24h (in anuric) | Goal-directed by volume status |
| D/P creatinine | Used in PET | 4-hour ratio to classify membrane |
Modern ISPD approach: "Adequacy" is now framed as goal-directed dialysis - shared decision making between patient and care team focusing on quality of life, symptom control, and individualized targets, not just Kt/V numbers alone.
10. COMPARISON TABLE: ALL PD MODALITIES AT A GLANCE
| Feature | CAPD | CCPD | NIPD | IPD | TPD |
|---|---|---|---|---|---|
| Machine | No | Yes | Yes | Optional | Yes |
| Peritoneum filled 24h | Yes | Yes | No (dry day) | No | Partial |
| Exchanges/day | 3-5 manual | 3-5 auto + 1 day dwell | 3-5 auto, no day | 10-24/session | Modified cycles |
| Dwell time | 4-12 hrs | 1-3 hrs (night) + 8-16 hrs (day) | 1-3 hrs | 30-60 min | Short (partial drain) |
| Ideal transporter | Low/Low-avg | High/High-avg | High (with RKF) | Acute/any | Any (drain alarms) |
| Hernia/leak risk | Higher | Lower (dry day) | Lowest | Low | Moderate |
| Peritonitis risk | Higher | Lower | Lower | Lower | Lower |
| Cost | $$ | $$$$ | $$$$ | $ | $$$$ |
| Best for | Low-resource; low transporters | Working patients; high transporters | Patients with good RKF | AKI; hospital-based | Low drain alarms; infusion pain |
11. KEY CLINICAL DECISION POINTS
Patient starting PD
│
├── Has significant RKF?
│ YES → Consider NIPD or incremental PD
│ NO → CCPD or full-dose CAPD
│
├── Works during the day?
│ YES → CCPD (daytime freedom)
│ NO → CAPD or CCPD both acceptable
│
├── High peritoneal transporter?
│ YES → APD/CCPD (short dwells before glucose absorbed)
│ NO → CAPD (long dwells for maximal diffusion)
│
├── Recent catheter placement (<2 weeks) or hernia risk?
│ YES → Urgent-start APD supine; low volumes; dry day
│
├── Low drain alarms / infusion pain on APD?
│ YES → Tidal PD (TPD) - retain 30% reserve volume
│
└── AKI / hospital setting?
→ IPD or low-volume APD
capd apparatus procedure pros cons diagram
Detailed medical diagram of CAPD (Continuous Ambulatory Peritoneal Dialysis) system showing: a human torso outline with the peritoneal catheter inserted through the abdominal wall into the peritoneal cavity, the Tenckhoff catheter with deep cuff in rectus muscle and superficial cuff in subcutaneous tissue, the external catheter connecting via a transfer set/titanium adapter to a Y-set, one limb of Y connecting to a fresh dialysate bag (hanging on IV pole) and the other limb connecting to a drain bag below. Label all components clearly: Fresh Dialysate Bag (2L), Y-connector, Transfer Set, PD Catheter, Peritoneal Cavity, Drain Bag (spent effluent), Deep Cuff (rectus muscle), Superficial Cuff (subcutaneous), Exit Site. Include arrows showing direction of flow: Fill arrow going into peritoneum, Drain arrow going out into drain bag. Show the flush-before-fill step with a small inset. Clean clinical illustration style with blue and white color scheme, well-labeled anatomy.
CAPD - Apparatus, Procedure, Pros & Cons
1. CAPD APPARATUS - COMPLETE EQUIPMENT LIST
The Peritoneal Membrane (the "natural dialyzer")
The PD Catheter
Full CAPD System Components:
| Component | Specification | Purpose |
|---|---|---|
| PD Catheter | Double-cuff, swan-neck, coiled Tenckhoff; silicone | Access into peritoneal cavity |
| Titanium adapter | Metal luer-lock connector | Joins catheter to transfer set |
| Transfer set | Short silicone/polyurethane tubing with clamp | Extension from catheter to Y-set |
| Y-set (Double-bag system) | Pre-attached fresh bag + drain bag on Y-limbs | Main exchange system |
| Fresh dialysate bags | 1.5L or 2L PVC bags (1.5%, 2.5%, or 4.25% glucose) | Provides osmotic agent + electrolytes |
| Drain bag | Sterile empty PVC bag, capacity 3L+ | Collects spent effluent |
| IV pole / stand | Adjustable height | Hang fresh bag for gravity infusion |
| Clamps | Roller or slide clamps | Control flow direction |
| Sterile caps / spike covers | Disposable | Maintain sterility between exchanges |
| Warming device | Dry warming pad (NOT microwave) | Warm dialysate to body temperature before infusion |
| Face mask | Surgical mask for patient and helper | Prevent droplet contamination during connection |
| Antiseptic supplies | Chlorhexidine, gauze, gloves | Exit site care |
2. CAPD SYSTEM DIAGRAM
3. CAPD PROCEDURE - STEP BY STEP
Pre-Exchange Preparation
- Wash hands thoroughly with soap and water for at least 2 minutes
- Dry with clean towel; apply alcohol-based hand rub
- Put on surgical face mask (patient and any helper)
- Gather all equipment: new dialysate bag, drain bag, Y-set, antiseptic supplies
- Inspect the dialysate bag:
- Check expiry date
- Check for cloudiness or particulates (discard if present)
- Check bag for leaks or damage
- Warm to body temperature (37°C) using warming pad
- Set up the Y-set: connect fresh bag and drain bag to the two limbs of the Y-connector (if not pre-attached)
The Exchange Procedure (Flush-Before-Fill - Double Bag System)
STEP 1 - CONNECT
Patient connects Y-set to transfer set adapter
(mask on; strict aseptic technique; all clamps closed)
STEP 2 - FLUSH (5 seconds)
Open fresh dialysate bag → flush briefly into drain bag
(purges any touch contaminants from connection point
into drain bag - this is the "flush before fill" safety step)
STEP 3 - DRAIN (20 minutes)
Open clamp to drain bag → spent dialysate drains from
peritoneum by gravity into drain bag
(first 1.6-1.8L drains fast; slows as residual volume
falls below 300 mL)
Clamp drain limb when drainage complete
STEP 4 - FILL (10 minutes)
Open clamp to fresh dialysate bag →
2L of warm fresh dialysate flows by gravity into
peritoneal cavity
Clamp when bag is empty
STEP 5 - DISCONNECT
Disconnect Y-set; apply sterile cap to transfer set
Secure catheter against body with tape/binder
STEP 6 - DWELL (4-8 hours)
Patient is FREE to move, walk, work
Diffusion + ultrafiltration occur continuously
CAPD Daily Schedule (Typical 4-Exchange Regimen):
| Time | Action | Dwell Duration |
|---|---|---|
| 6:00 AM | Drain overnight bag + Fill fresh 1.5% glucose | 6 hours |
| 12:00 PM | Drain + Fill fresh 1.5% or 2.5% glucose | 5 hours |
| 5:00 PM | Drain + Fill fresh 2.5% glucose | 5 hours |
| 10:00 PM | Drain + Fill icodextrin or 4.25% glucose | 8-12 hours (overnight) |
| Next 6 AM | Drain overnight + repeat cycle | - |
Most common CAPD prescription (PDOPPS registry): 4 exchanges/day × 2.0-2.5 L/exchange
The Double-Bag System in Detail:
[FRESH DIALYSATE BAG]
|
--------Y--------
| |
[Drain bag] [Transfer set → Catheter → Peritoneum]
Step 1: Short flush → fresh dialysate runs briefly → drain bag
(clears intraluminal contaminants)
Step 2: Drain spent dialysate → drain bag (20 min gravity)
Step 3: Break "frangible pin" in tubing → fill peritoneum (10 min gravity)
Step 4: Clamp, disconnect, cap → dwell begins
The frangible (breakable) pin is a built-in safety feature in the tubing. Breaking it opens the fill channel after drainage is complete, ensuring the correct sequence is always followed.
4. PROS AND CONS OF CAPD
✅ ADVANTAGES (PROS)
Clinical Advantages:
| Advantage | Explanation |
|---|---|
| Hemodynamic stability | Slow, continuous fluid removal - no rapid fluid shifts; better tolerated in heart failure and elderly |
| Preserves residual kidney function (RKF) | Better than HD - no acute intravascular volume depletion; ACEi/ARB use supported |
| No blood-membrane contact | Avoids HD-associated accelerated RKF decline; no heparin required |
| Continuous dialysis | 24h/7d solute clearance - more physiological than intermittent HD |
| Better middle-molecule clearance | Long dwell times allow equilibration of larger solutes |
| Lower infection rate vs standard system | Y-set flush-before-fill dramatically reduced CoNS peritonitis |
| Good for high potassium | Continuous K⁺ removal avoids inter-dialytic hyperkalaemia surges |
| Useful in AKI | Can treat hyperkalemia and acidosis; used in low-resource settings and during COVID-19 |
| Post-transplant advantage | PD patients have better 5-year survival and lower delayed graft function vs prior HD |
Practical / Lifestyle Advantages:
| Advantage | Explanation |
|---|---|
| Home-based | No need to travel to dialysis center 3x/week |
| No machine required | Portable; only bags and Y-set needed |
| Travel-friendly | Dialysate bags can be shipped to destination |
| Dietary flexibility | Continuous dialysis = less strict dietary restrictions |
| Better quality of life | Higher self-reported QoL vs other dialysis modalities |
| Lower cost | Significantly cheaper than APD and often competitive with HD |
| Preferred in low/middle income countries | No electricity or expensive equipment needed |
| Incremental dialysis possible | Can start with 2-3 exchanges/day and increase as RKF declines |
| Suitable for elderly with assistance | Carer can perform exchanges |
| No vascular access | Avoids AVF/graft/catheter complications |
| Useful when vascular access fails | Absolute indication when HD access is impossible |
❌ DISADVANTAGES (CONS)
Clinical Disadvantages:
| Disadvantage | Explanation |
|---|---|
| Peritonitis risk | Most serious complication; 6% mortality per episode; requires vigilant technique |
| Glucose absorption | Up to 2/3 of glucose absorbed per exchange → hyperglycaemia, obesity, dyslipidaemia |
| Increased hernia risk | Continuous intraabdominal pressure (day + night) → higher hernia and leak rate vs APD |
| Back pain | Continuous fluid load increases lumbar pressure |
| Protein loss | ~5-15g/day protein lost in effluent → nutritional risk |
| Less efficient than HD | Lower per-hour clearance rate; requires continuous 24h operation to compensate |
| Volume overload risk | Especially with UF failure or non-compliance |
| Peritoneal membrane deterioration | Long-term glucose/lactate exposure → loss of membrane function; eventual encapsulating peritoneal sclerosis (EPS) |
| Insufficient for catabolic states | High urea generation may exceed CAPD clearance capacity |
Practical Disadvantages:
| Disadvantage | Explanation |
|---|---|
| Multiple daily exchanges | 3-5 connections/day is burdensome and time-consuming |
| Requires patient training | 1-2 week education program required before starting |
| Demands manual dexterity | Poor eyesight, arthritis, or cognitive impairment may preclude CAPD |
| Home storage | Large volume of supplies (dialysate bags) needed at home |
| Daytime disruption | Each exchange takes 20-30 min; must plan day around exchange times |
| Body image | Permanent external catheter; some patients find this distressing |
| Beyond 4 exchanges is cumbersome | Patients needing >4/day often better switched to APD |
5. INDICATIONS FOR CAPD
Renal Indications:
- Inability to perform hemodialysis
- Vascular access failure
- HD intolerance
- Children age 0-5 years
- Severe peripheral vascular disease
- Severe cardiac function impairment
- Patient preference
- Bleeding diathesis (no heparin needed in CAPD)
- Multiple myeloma
- Needle anxiety
- Labile diabetes mellitus
- Lifestyle preference
Non-Renal Indications:
- Drug poisoning
- Refractory congestive heart failure
- Hepatic failure
- Hypo/hyperthermia
- Dialysis-associated ascites
- Pancreatitis
6. CONTRAINDICATIONS
| Type | Conditions |
|---|---|
| Absolute | Intra-abdominal infection; documented Type II UF failure; loss of peritoneal surface (adhesions); severe inflammatory bowel disease; severe psychiatric/active psychotic disorders; third trimester pregnancy |
| Relative | Abdominal wall hernias; severe obesity; stomas or feeding tubes; intra-abdominal adhesions; visual impairment; proteinuria >10 g/day; poor socioeconomic conditions |
7. CAPD vs APD - QUICK REFERENCE
| Feature | CAPD | APD |
|---|---|---|
| Machine | ❌ None needed | ✅ Cycler required |
| Cost | $$ Low | $$$$ High |
| Hernia/leak risk | Higher | Lower (dry day) |
| Peritonitis risk | Slightly higher | Slightly lower |
| Daily connections | 3-5 sterile breaks | 1 nightly connection |
| Daytime freedom | Less (exchanges interrupt day) | More (free during day) |
| For low transporters | ✅ Ideal (long dwells) | Less optimal |
| For high transporters | Less optimal | ✅ Ideal (short rapid cycles) |
| Travel | ✅ Easy | Harder (cycler required) |
| Elderly/assisted | More challenging | Easier (1-2 visits/day) |
| Cirrhosis/ascites | ✅ Better (control drain volume) | More challenging |
apd apparatus procedures and ipd apparays
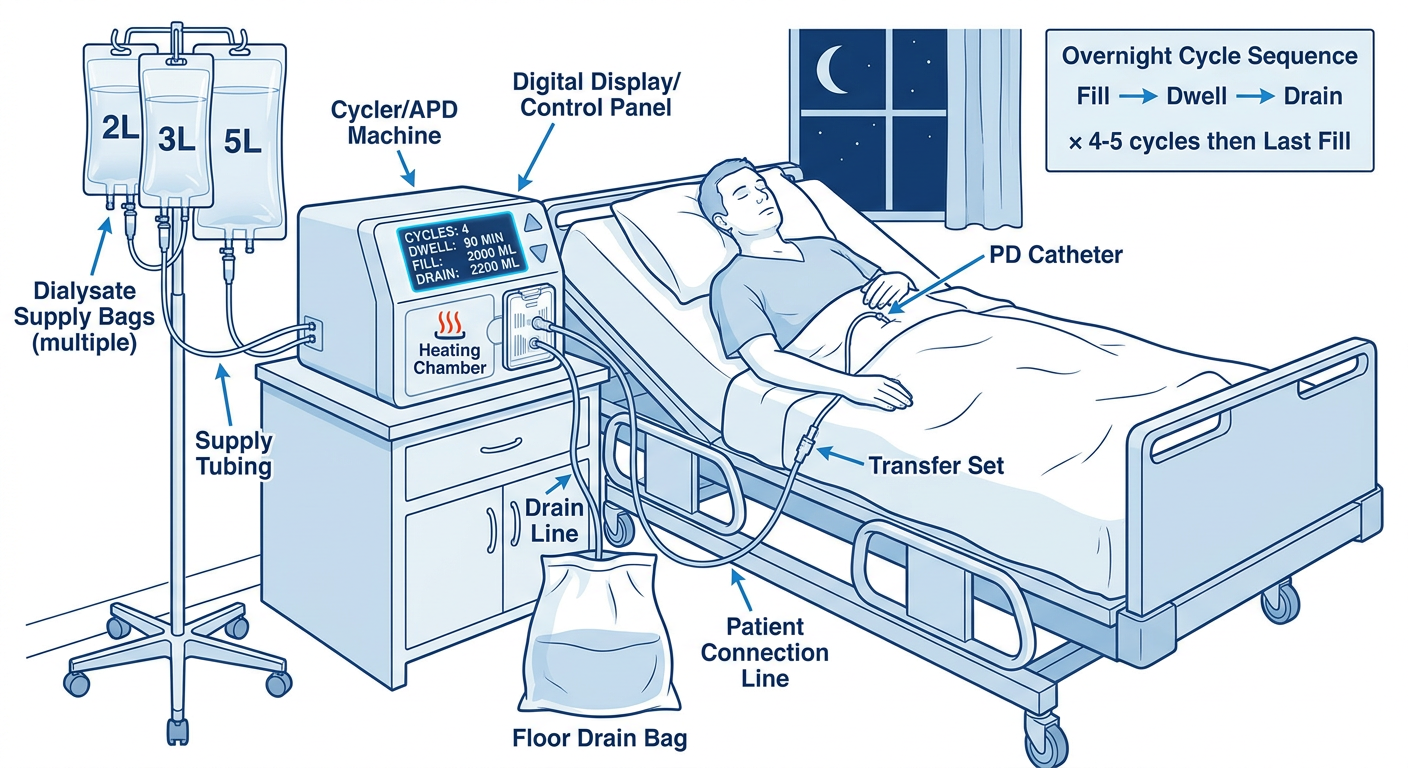
Detailed medical diagram of APD (Automated Peritoneal Dialysis) system showing: a bedside cycler machine with digital display screen showing programmed settings (number of cycles, dwell time, fill volume, drain volume), multiple large dialysate bags (2-6L each) connected to the cycler via supply tubing, a heating element/warmer inside the cycler, a disposable cassette/tubing set attached to the cycler, a drain line going to a large floor drain bag or drain point, and patient connection line going to the patient's PD catheter via transfer set. Label all parts clearly: Cycler/APD Machine, Digital Display/Control Panel, Dialysate Supply Bags (multiple), Heating Chamber, Disposable Cassette, Drain Line, Patient Connection Line, Transfer Set, PD Catheter. Show patient lying in bed connected to cycler at night. Include a small inset showing the overnight cycle sequence: Fill → Dwell → Drain × 4-5 cycles then Last Fill. Clean clinical blue and white medical illustration style with clear labels.
Medical diagram of IPD (Intermittent Peritoneal Dialysis) setup for acute/hospital use showing: a hospital bed with a patient, a simple gravity-based peritoneal dialysis system with a dialysate bag hanging on IV pole, manual roller clamp on tubing, a Y-connector, PD catheter going into patient's abdomen, and a drain bag below. Show multiple bags staged and ready. Label: Dialysate Bag (1-2L), IV Pole, Roller Clamp, Y-connector, PD Catheter, Peritoneal Cavity (abdominal outline), Drain Bag, Timer/clock indicating 30-60 minute dwell intervals. Include a cycle schedule timeline showing rapid exchanges: Fill (10 min) - Dwell (30-60 min) - Drain (20 min) repeated 10-24 times over an 8-12 hour session, with dry periods between sessions. Clinical style, clear labels, blue and white color scheme.
APD & IPD - Apparatus, Procedure & System Details
PART A: APD - AUTOMATED PERITONEAL DIALYSIS
1. APD APPARATUS - COMPLETE EQUIPMENT
The Cycler Machine - Core Component
| Cycler Feature | Description |
|---|---|
| Digital control panel | Touchscreen or button interface; programs number of cycles, fill volume, dwell time, drain time, total therapy time |
| Peristaltic/pressure pump | Drives fluid in controlled volumes; measures pressure to detect blockages |
| Integrated fluid warmer/heater | Warms dialysate to 37°C before infusion (prevents shivering and discomfort) |
| Volume measurement system | Gravimetric or volumetric; records fill volume, drain volume, and net UF per cycle |
| Alarm system | Audible + visual alarms for: low drain, kink in line, air in line, machine error, end of therapy |
| Remote monitoring capability | Modern cyclers transmit session data (inflow time, dwell time, drain time, volumes) to clinic via internet |
| Data logging | Records every cycle's performance; downloadable for clinical review |
| Battery backup | Some models support short power outages |
Commercial Cycler Examples:
| Brand | Model |
|---|---|
| Baxter | HomeChoice / HomeChoice Pro / Amia |
| Fresenius | Sleep Safe / Sleep Safe Harmony |
| Nipro | PD-NIGHT |
Full APD Equipment List:
| Component | Specification | Purpose |
|---|---|---|
| APD Cycler machine | Bedside; ~5-10 kg | Automated control of all exchange phases |
| Disposable cassette/tubing set | Single-use; pre-sterilized | Fluid pathway inside cycler; changed per session |
| Large dialysate supply bags | 1.5L to 6L bags (vs 2L for CAPD) | Fluid reservoir for multiple overnight cycles |
| Drain line / drain bag | Tubing to household drain or large bag (5-10L) | Continuous drainage of spent effluent |
| Patient line / connection tubing | Sterile; connects cycler to patient | From cycler outlet to patient transfer set |
| Transfer set | Short tubing + clamp on patient | Junction between patient catheter and cycler line |
| PD Catheter | Same double-cuff Tenckhoff as CAPD | Peritoneal access |
| Sterile caps | Disposable | Cap transfer set when disconnecting from cycler |
| Surgical mask | For patient/helper at connection | Prevent contamination during nightly hook-up |
| Alcohol wipes / antiseptic | For connection site | Sterility maintenance |
APD vs CAPD - Equipment Differences:
| Feature | CAPD | APD |
|---|---|---|
| Machine | None | Cycler (bedside) |
| Bag size | 2L individual bags | 2-6L large supply bags |
| Tubing | Simple Y-set, gravity | Disposable cassette, pump-driven |
| Exchange control | Manual by patient | Fully automated |
| Storage space | Multiple 2L bags | Fewer, larger bags + cycler |
| Electricity | Not required | Required |
| Cost | $$ | $$$$ |
2. APD PROCEDURE - STEP BY STEP
Pre-Session Setup (Evening - ~30 mins before sleep)
- Cycler machine (already at bedside)
- New disposable cassette/tubing set (changed every session or per manufacturer)
- Required number of dialysate supply bags for the night
- Patient mask, alcohol wipes, sterile cap
- Insert new disposable cassette into cycler housing
- Connect supply bags to the appropriate supply ports on the cassette
- Connect drain tubing to drain point (household drain, toilet, or large drain bag)
- Prime the tubing (cycler auto-primes on most modern machines)
- Total therapy time (e.g., 8-9 hours)
- Fill volume per cycle (e.g., 2.0-2.5 L)
- Number of cycles (e.g., 4-5 overnight cycles)
- Dwell time per cycle (calculated automatically)
- Last fill volume and solution type (e.g., 2L icodextrin for daytime dwell)
- Cycler heats dialysate automatically to 37°C before each fill
The Nightly APD Session (CCPD Mode):
10:00 PM Patient connects to cycler
↓
INITIAL DRAIN
Drains any residual fluid from last daytime dwell
↓ CYCLE 1
FILL (10-15 min) → Cycler pumps 2L warm fresh dialysate
DWELL (1-2 hrs) → Diffusion + UF occur
DRAIN (20-30 min)→ Cycler drains spent dialysate to drain
↓ CYCLE 2 → same sequence
↓ CYCLE 3 → same sequence
↓ CYCLE 4 → same sequence
↓ CYCLE 5 (if programmed)
↓ LAST FILL (6 AM)
Cycler delivers final 2L icodextrin or glucose bag
→ This stays in peritoneum all day (daytime dwell)
6:00 AM DISCONNECT from cycler
Apply sterile cap to transfer set
Patient FREE all day
10:00 PM Reconnect → drain last fill → new session begins
Tidal APD Mode (for drain alarms or infusion pain):
Standard: Fill 2L → Drain ALL → next fill 2L
↓
70% Tidal: Fill 2L → Drain only 1.4L (70%)
→ 0.6L stays as "tidal reserve"
→ Next fill: only 1.4L added (total back to 2L)
→ Repeat until final complete drain
Tidal mode prevents the cycler from alarming when the peritoneum empties and also reduces end-drain pain from catheter tip touching pelvic structures.
Disconnecting in the Morning:
- Allow cycler to complete last fill delivery
- Stop cycler; clamp patient line
- Put on mask
- Disconnect patient line from transfer set using aseptic technique
- Apply sterile cap to transfer set
- Secure catheter against body
- Log therapy data or review cycler screen for overnight summary (total UF, total drained, any alarms)
3. APD - KEY CLINICAL FEATURES
| Parameter | Typical Values |
|---|---|
| Session duration | 8-10 hours (overnight) |
| Cycles per session | 3-5 |
| Fill volume per cycle | 2.0-2.5 L |
| Supply bag size | 1.5-6 L |
| Total fluid used per night | 8-15 L |
| Dwell time per cycle | 60-180 min |
| Last fill (daytime dwell) | 1.5-2 L icodextrin |
| Glucose concentration | 1.5%, 2.5%, or 4.25% |
| Temperature of infused fluid | 37°C (warmed by cycler) |
4. APD PROS & CONS
✅ APD Advantages:
| Advantage | Detail |
|---|---|
| Daytime freedom | Single nightly connection; patient free during day |
| Fewer sterile breaks | 1 connection/night vs 3-5/day in CAPD |
| Lower peritonitis risk | Fewer connections = fewer contamination opportunities |
| Lower hernia/leak risk | Dry abdomen during day reduces intraperitoneal pressure |
| Lower back pain | Upright abdomen is empty |
| Ideal for high transporters | Short, rapid cycles maximize UF before glucose absorbed |
| Remote monitoring | Clinic can review overnight data without patient attending |
| Fluid warming | Built-in heater prevents cold infusion discomfort |
| Ideal for working patients | No daytime exchange disruption |
| Better for assisted PD | Carer connects once at night; 1-2 visits vs 4-5 for CAPD |
| Urgent-start PD | Supine low-volume cycling = safest way to start early PD |
| Tidal mode | Solves low-drain alarms and infusion/drain pain |
❌ APD Disadvantages:
| Disadvantage | Detail |
|---|---|
| High cost | Cycler + cassettes + large bags = significantly more expensive than CAPD |
| Electricity dependent | Power outages disrupt therapy; some machines have battery backup |
| Sleep disruption | Alarms (low drain, kink, air) may wake patient at night |
| Drain pain | Catheter tip touching peritoneal structures when nearly empty |
| Sodium sieving | Short rapid dwells cause more sodium sieving → increased thirst |
| Complex training | Machine setup, cassette loading, alarm troubleshooting |
| Equipment burden | Cycler + large bags; less portable than CAPD |
| Less suitable for cirrhosis | Cannot finely control individual drain volumes |
| Less confident with backup CAPD | APD patients less practiced with manual Y-set exchanges |
| Daytime UF depends on last fill | If last fill UF is inadequate, may not maintain fluid balance |
PART B: IPD - INTERMITTENT PERITONEAL DIALYSIS
5. IPD APPARATUS
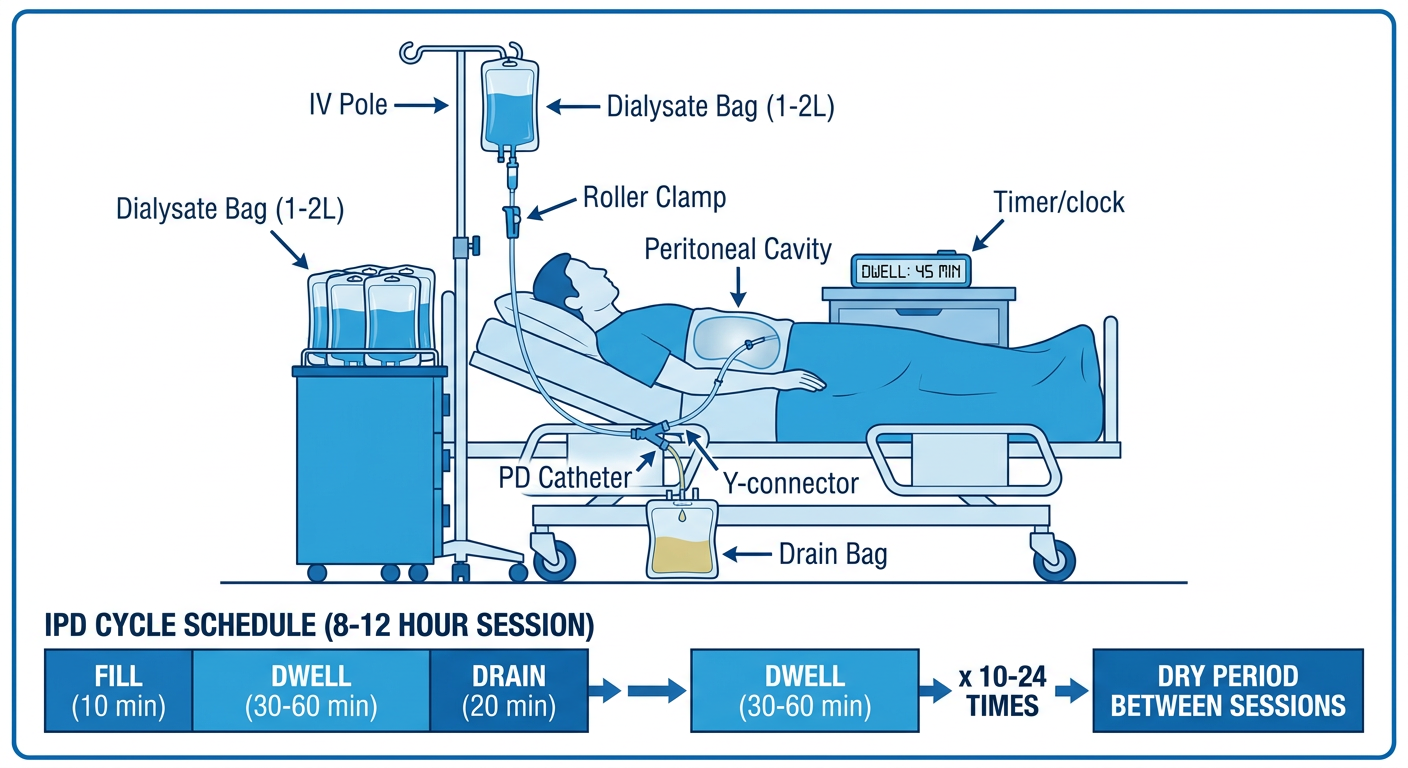
IPD is the simplest PD setup - primarily a gravity-based system:
| Component | Specification | Purpose |
|---|---|---|
| PD catheter | Tenckhoff (same design) or temporary acute catheter | Peritoneal access |
| Dialysate bags | 1-2L bags; multiple bags staged | Fluid for rapid exchanges |
| IV pole/stand | Height-adjustable | Gravity-driven infusion |
| Standard IV/PD tubing | With roller clamp | Connects bag to catheter |
| Y-connector | Optional; or straight set | Connect fill and drain |
| Drain bag | Large sterile bag or direct gravity drain | Collect spent effluent |
| Roller clamps (×2) | On fill line and drain line | Control flow direction manually |
| Timer | Bedside clock or nursing timer | Track dwell times (30-60 min) |
| Warming facility | Warming cabinet or basin | Warm bags to 37°C |
| Nursing documentation | Exchange chart | Record fill/drain volumes, times, fluid balance |
IPD may also use an APD cycler in hospital settings when available - the cycler is simply programmed for short, rapid cycles without a daytime last fill.
6. IPD PROCEDURE - STEP BY STEP
Session Setup:
- Warm dialysate bags to 37°C
- Prepare enough bags for entire session (10-24 exchanges × 1-2L = 20-40L total)
- Prime tubing; connect to PD catheter using aseptic technique
- Position patient: supine (hospital bed)
Each Exchange (repeated 10-24 times per session):
FILL (5-10 min)
Open fill clamp → gravity infills 1-2L warm dialysate
Close fill clamp when bag empty
DWELL (30-60 min)
Both clamps closed
Diffusion + UF occur across peritoneal membrane
Nurse documents time started
DRAIN (15-20 min)
Open drain clamp → spent dialysate drains by gravity into drain bag
Close drain clamp when drainage stops (or slows to a trickle)
Record drain volume and appearance (clear vs cloudy)
REPEAT → hang new dialysate bag → next exchange
Full IPD Session:
| Feature | Typical Values |
|---|---|
| Session duration | 8-12 hours per session |
| Exchanges per session | 10-24 rapid exchanges |
| Dwell time per exchange | 30-60 minutes (very short) |
| Volume per exchange | 1.0-2.0 L |
| Total fluid per session | 20-40 L |
| Frequency | 3-4 sessions/week (like HD schedule) |
| Between sessions | Peritoneum is DRY |
| Setting | Hospital, dialysis unit, or clinic |
7. IPD - SPECIAL CONSIDERATIONS
Acute IPD (for AKI):
- Used when urgent renal replacement is needed but HD is unavailable
- Effective for hyperkalaemia and acidosis correction
- Short dwells + high glucose concentration (2.5%-4.25%) for maximum UF
- Used in low-resource settings and during equipment shortages (e.g., COVID-19)
- Catheter may be temporary (acute) or permanent Tenckhoff placed urgently
IPD with APD Cycler (hospital):
- Cycler programmed for: 1-2L fill × 10-20 rapid cycles × 30-60 min dwell
- No last fill at end
- Drain to bedside bag or hospital drain
- More precise volume control and less nursing burden than gravity IPD
8. IPD PROS & CONS
✅ IPD Advantages:
| Advantage | Detail |
|---|---|
| Peritoneum rests between sessions | Lower intraperitoneal pressure most of the time |
| Fewer hernias and leaks | Pressure only during 8-12h sessions; dry the rest |
| Hospital-based / nurse-managed | Patient doesn't need to self-care |
| No patient training required | Suitable for acutely ill patients |
| Effective for AKI | Treats hyperkalaemia, acidosis, fluid overload |
| Low resource requirement | Basic IV bags, tubing, gravity setup; no electricity needed |
| Lower glucose exposure | Shorter total membrane contact time |
| Flexibility | Can be performed anywhere with basic supplies |
❌ IPD Disadvantages:
| Disadvantage | Detail |
|---|---|
| Least efficient PD modality | Short dwells = incomplete equilibration, especially for larger solutes |
| Requires frequent hospital attendance | 3-4 sessions/week = clinic-dependent |
| Not suitable for long-term ESKD | Insufficient clearance for anuric chronic patients |
| Labour intensive | Nurse must manage multiple rapid exchanges per session |
| Fluid balance challenges | Rapid fluid shifts can destabilize haemodynamics |
| Protein loss | Each exchange removes protein from dialysate |
| Risk of contamination | Multiple bag changes per session = more sterile break points |
| Cold dialysate risk | Bags must be consistently warmed between exchanges |
9. SIDE-BY-SIDE COMPARISON: CAPD vs APD vs IPD
| Feature | CAPD | APD (CCPD) | IPD |
|---|---|---|---|
| Machine | None | Cycler | None (or cycler) |
| Manual/Auto | Manual | Automated | Manual (or auto) |
| Exchanges/session | 3-5/day | 3-5/night + last fill | 10-24/session |
| Dwell time | 4-12 hours | 1-3 hrs (night), 8-16 hrs (day) | 30-60 minutes |
| Peritoneum filled 24h | Yes | Yes (CCPD) | No (dry between sessions) |
| Sessions per week | 7 days | 7 nights | 3-4 sessions |
| Hernia/leak risk | High | Low (if dry day) | Low |
| Peritonitis risk | Moderate | Lower | Lower |
| Ideal setting | Home (outpatient) | Home (outpatient) | Hospital/clinic |
| Requires training | Yes (patient) | Yes (patient) | No (nurse-managed) |
| Cost | $$ | $$$$ | $ |
| Best for | ESKD home patient | Working adults; high transporters | AKI; hospital; acute |
| RKF needed? | No | No (CCPD); Yes (NIPD) | No |
10. ALARM MANAGEMENT ON APD CYCLER
| Alarm Type | Cause | Action |
|---|---|---|
| Low drain | Catheter partially blocked; constipation; low residual volume | Reposition patient; treat constipation; switch to tidal mode |
| Line kink | Tubing bent | Straighten tubing |
| No flow / occluded | Catheter tip migration or omentum trapping | Guidewire manipulation or laparoscopic repositioning |
| Air in line | Disconnected tubing or empty bag | Check connections; replace bag |
| Overfill | Programmed volume exceeds tolerance | Reduce fill volume |
| End of therapy | Session completed | Morning disconnect routine |
assessment of peritoneal membrane permeability
Assessment of Peritoneal Membrane Permeability
1. WHY ASSESS THE PERITONEAL MEMBRANE?
- Classify transport status to guide PD prescription
- Detect ultrafiltration failure (UFF) early
- Monitor membrane deterioration from repeated peritonitis or long-term glucose exposure
- Evaluate free water transport via aquaporin-1 channels
- Adjust modality (CAPD vs APD) and dwell time to suit individual membrane biology
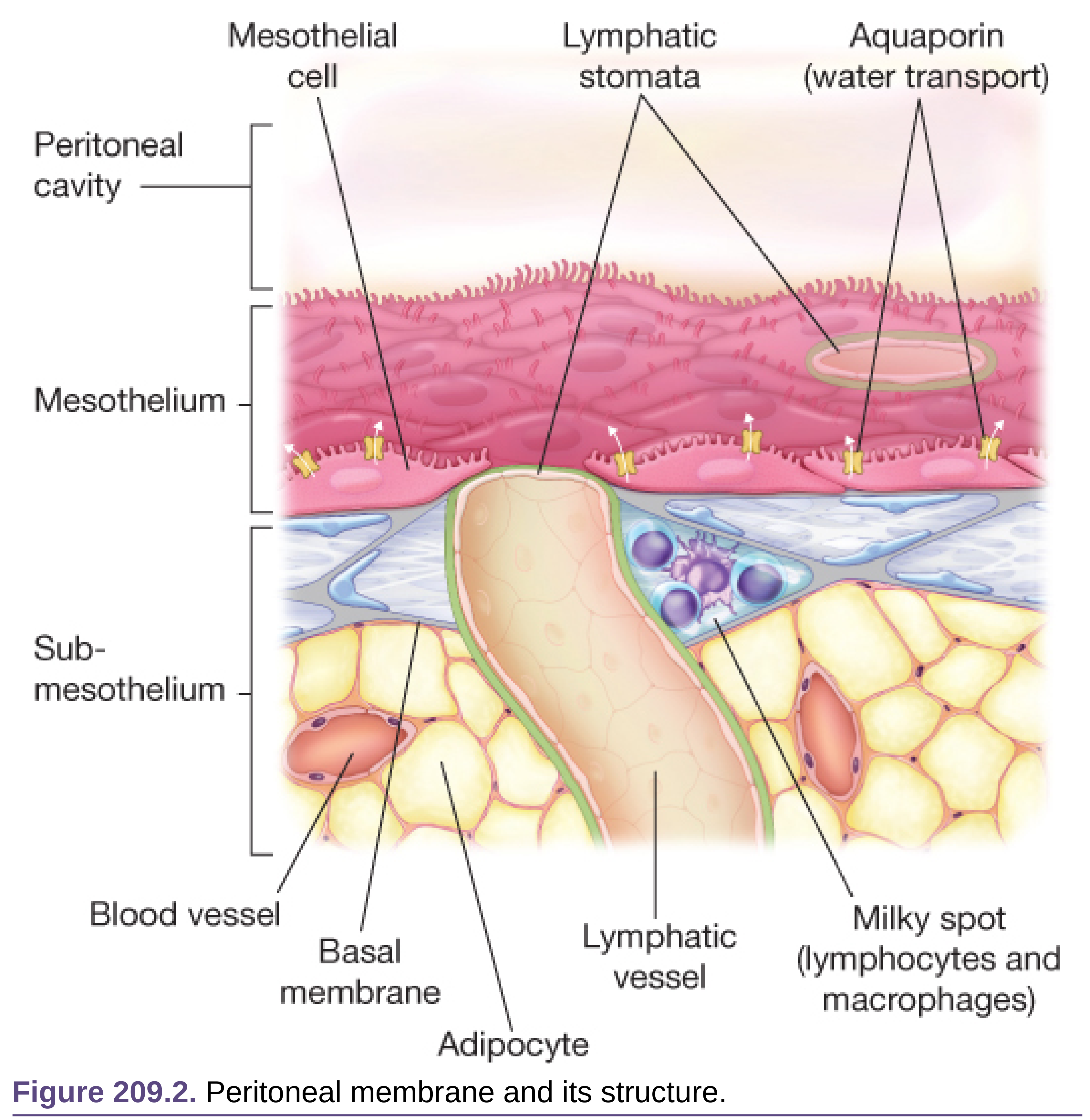
2. STRUCTURE OF THE PERITONEAL MEMBRANE - TRANSPORT BASIS
| Pore Type | Size | What Crosses | % of UF |
|---|---|---|---|
| Ultra-small pores (Aquaporin-1, AQP-1) | 3-5 Å | Water ONLY (no solutes) | ~50% of transcapillary UF |
| Small pores | 40-50 Å | Water + small solutes (urea, creatinine, glucose, electrolytes) | ~45% |
| Large pores | up to 150 Å | Water + larger molecules (proteins, albumin) | ~5% |
Key concept: Glucose has a very low osmotic reflection coefficient through small pores (near 0 = passes freely) but a very HIGH reflection coefficient through aquaporin-1 channels (= 1, completely impermeable). This is why glucose drives UF mainly through AQP-1 - water crosses but glucose cannot → creates an oncotic gradient.
- Peritoneal capillary wall = main barrier
- Interstitium = significant additional barrier to water and solute movement
- Mesothelial cell layer = tertiary barrier
3. WHAT IS "TRANSPORT STATUS"?
- Effective peritoneal surface area
- Capillary density and vascularity
- Membrane permeability
| Transport Status | What it Means |
|---|---|
| High transporter | Rapid solute equilibration; rapid glucose absorption → early loss of osmotic gradient; good solute removal but poor UF with long dwells |
| High-average transporter | Moderate-fast equilibration |
| Low-average transporter | Moderate-slow equilibration |
| Low transporter | Slow equilibration; glucose absorbed slowly → sustained osmotic gradient; good UF but slower solute removal; long dwells needed |
4. THE PERITONEAL EQUILIBRATION TEST (PET)
The Gold Standard Test for Membrane Permeability
PET Procedure - Step by Step:
| Step | Action |
|---|---|
| Preparation | Empty peritoneal cavity completely (drain previous overnight dwell for 20 min with patient sitting upright) |
| Step 1 - Fill | Instill 2 L of 2.27% (or 2.5%) glucose dialysate warmed to 37°C; infuse over 10 minutes with patient supine; patient rolls side-to-side every 2 minutes during infusion to distribute fluid throughout peritoneal cavity including paracolic gutters |
| Step 2 - Time 0 sample | At exactly 10 min after start of infusion: drain 200mL into bag; discard first 5mL; collect next 5mL for creatinine and glucose (dialysate D0 sample); return remainder to peritoneum |
| Step 3 - 2-hour sample | At 2 hours post-fill: collect dialysate sample as above for creatinine and glucose |
| Step 4 - Blood sample | At 2 hours: draw simultaneous plasma sample for creatinine and glucose |
| Step 5 - 4-hour drain | At exactly 4 hours: drain dialysate completely over 20 minutes; weigh total drain bag; subtract empty bag weight to calculate total drain volume (= net UF) |
| Step 6 - 4-hour sample | After mixing the 4-hour drain bag: collect sample for creatinine and glucose |
PET Calculations:
| Ratio | Formula | Meaning |
|---|---|---|
| D/P creatinine | Dialysate creatinine at 4h ÷ Plasma creatinine at 2h | Solute transport rate (↑ = high transporter) |
| D/D₀ glucose | Dialysate glucose at 4h ÷ Dialysate glucose at time 0 | Glucose absorption rate (↓ = high transporter; glucose absorbed faster) |
| Net UF | Total drain volume - 2000 mL fill volume | Ultrafiltration capacity |
PET Interpretation Graph:
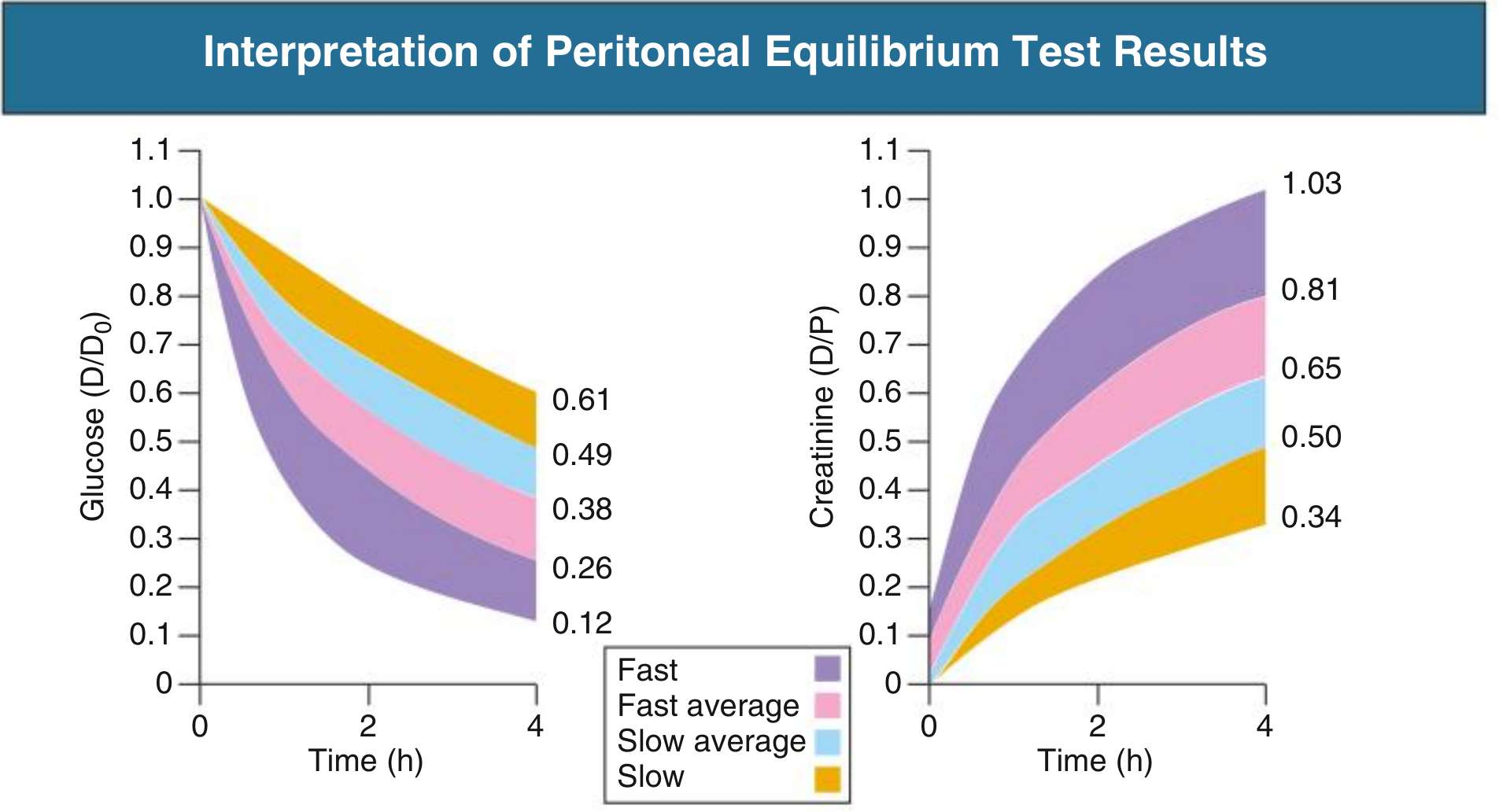
PET Classification Cutoffs (at 4 hours):
| Transport Category | D/P Creatinine at 4h | D/D₀ Glucose at 4h | Clinical Implication |
|---|---|---|---|
| High (Fast) | > 0.81 | < 0.26 | Rapid equilibration; glucose absorbed fast; poor UF with long dwells; high solute clearance |
| High-Average (Fast-Avg) | 0.65-0.81 | 0.26-0.38 | Moderate-fast; flexible PD options |
| Low-Average (Slow-Avg) | 0.50-0.65 | 0.38-0.49 | Moderate-slow; good UF with standard dwells |
| Low (Slow) | < 0.50 | > 0.49 | Slow equilibration; sustained osmotic gradient; good UF; needs long dwells for adequate solute clearance |
~70% of patients have stable transport status at 1 year post-PET; ~50% remain stable at 2 years. Transport can increase (worsen) with repeated peritonitis, long-term PD, or membrane damage.
PET Results - Prescription Guidance:
| Transport Status | Best Modality | Why |
|---|---|---|
| High | APD (short rapid cycles) | Short dwells maximize UF before glucose absorbed; avoid long dwells |
| High-Average | APD or CAPD | Flexible |
| Low-Average | CAPD | Moderate dwells adequate |
| Low | CAPD (long dwells) | Long dwells needed for adequate solute equilibration; excellent UF |
Modern practice caveat: While transport status guides prescription theoretically, current ISPD guidelines recommend prescriptions be individualized to patient lifestyle and preference rather than solely dictated by PET results. Patient preference now takes priority.
5. UF CAPACITY ASSESSMENT FROM PET
| UF at 4h (with 2.27% glucose) | Interpretation |
|---|---|
| > 400 mL | Normal UF capacity |
| < 400 mL | Possible UF failure - investigate further |
- Perform a 4-hour dwell with 3.86%/4.25% glucose
- UF < 400 mL with high-concentration solution = confirmed Ultrafiltration Failure (UFF)
6. ULTRAFILTRATION FAILURE (UFF) - CLASSIFICATION
| Type | Mechanism | PET Finding | Treatment |
|---|---|---|---|
| Type I (High transport) | Increased peritoneal surface area/vascularity; rapid glucose absorption | High D/P Cr; low UF with standard solutions | Short dwells (APD); icodextrin for long dwells |
| Type II (Aquaporin failure) | Loss of AQP-1 channels; free water transport reduced | Low sodium sieving on mini-PET | Absolute contraindication to PD; must transfer to HD |
| Type III (Lymphatic absorption) | Increased lymphatic reabsorption of dialysate | Normal D/P; low net UF | Reduce dwell time |
| Type IV (Catheter/mechanical) | Mechanical problem - leak, migration, loculation | Normal membrane parameters | Fix catheter problem |
7. ALTERNATIVE PET TESTS
A. Mini-PET (Fast PET)
| Feature | Detail |
|---|---|
| Solution | 3.86% or 4.25% glucose (high concentration) |
| Dwell time | 1 hour only (vs 4 hours in standard PET) |
| What it measures | Small-solute transport AND free water transport |
| Key measurement | Sodium concentration in 1-hour drained dialysate |
| Principle | High-concentration glucose drives water via AQP-1 → sodium sieving occurs (dialysate Na falls below plasma) - if sodium does NOT fall, AQP-1 failure is suspected |
| Advantage | Faster; identifies free water transport defect |
B. Double Mini-PET
| Feature | Detail |
|---|---|
| Method | Two consecutive mini-PETs: first with 1.36%/1.5% glucose, then with 3.86%/4.25% glucose |
| What it measures | Osmotic conductance of glucose (OCG) - the ability of glucose to drive water transport |
| Key calculation | Difference in drain volume between low and high concentration solutions = free water transport capacity |
| Use | Detect early UFF; research tool; identifies AQP-1 transport defect before clinical UFF develops |
| Limitation | More complex; still being validated for routine clinical use |
C. 24-Hour Dialysate Collection
| Feature | Detail |
|---|---|
| Method | Collect all dialysate from all exchanges over 24 hours |
| Measurements | Urea, creatinine clearance; total UF; total protein loss |
| Use | Calculate weekly Kt/V urea; peritoneal creatinine clearance; protein losses |
| Not for | Transport classification (PET is needed for that) |
D. MTAC (Mass Transfer Area Coefficient)
- The theoretical instantaneous maximal solute clearance at time 0, without ultrafiltration
- Requires computer modelling of multiple dialysate samples
- Represents true membrane permeability independent of dwell time and UF
- Clinically approximated by: 4-hour D/P ratio or 24-hour clearance
- Used mainly in research; not routine clinical practice
8. FACTORS THAT ALTER TRANSPORT STATUS OVER TIME
| Factor | Effect on Transport |
|---|---|
| Peritonitis episode | Acutely ↑ transport (inflammation ↑ vascularity) |
| Long-term glucose exposure | Progressive ↑ transport; membrane fibrosis |
| Biocompatible PD solutions | Slower deterioration of membrane function |
| Encapsulating peritoneal sclerosis (EPS) | Severe ↓ transport in late stage |
| Time on PD | Gradual shift toward higher transport over years |
| Recently placed catheter (<1 month) | Falsely elevated transport (post-surgical inflammation) |
9. WHEN TO PERFORM THE PET - CLINICAL INDICATIONS
| Indication | Timing |
|---|---|
| Baseline assessment | 4-6 weeks after starting PD (after full healing) |
| Inadequate dialysis | When Kt/V or UF is suboptimal despite prescription changes |
| UF failure investigation | When net UF consistently < 400mL/day |
| Changing modality | CAPD → APD or vice versa |
| After peritonitis | 4-6 weeks after resolution |
| Routine surveillance | Annually or per center protocol |
Current perspective: PET is NOT required routinely for every PD patient at every center. Modern PD prescription is primarily driven by patient preference and clinical response, not solely by PET transport category. Several expert centers no longer perform routine PET unless clinically indicated.
10. SUMMARY TABLE - PET AT A GLANCE
| Feature | Value |
|---|---|
| Solution used | 2.27% or 2.5% glucose, 2L |
| Temperature | 37°C (warmed) |
| Patient position during fill | Supine; rolls side to side |
| Sample times | Time 0, 2 hours, 4 hours (dialysate); 2 hours (blood) |
| Key ratios | D/P creatinine at 4h; D/D₀ glucose at 4h |
| High transporter | D/P Cr > 0.81; D/D₀ glucose < 0.26 |
| Low transporter | D/P Cr < 0.50; D/D₀ glucose > 0.49 |
| Normal UF | > 400 mL at 4h |
| UFF confirmed | < 400 mL with 4.25% solution |
| Do NOT perform PET | Within 1 month of catheter insertion; during/after peritonitis |
| Mini-PET | 1 hour; 4.25% glucose; measures free water transport |
| Double mini-PET | Two consecutive 1h dwells; measures osmotic conductance |
acute peritoneal dialysis definition apparatus procedure pro and cons
acute peritoneal dialysis procedure apparatus pros and cons
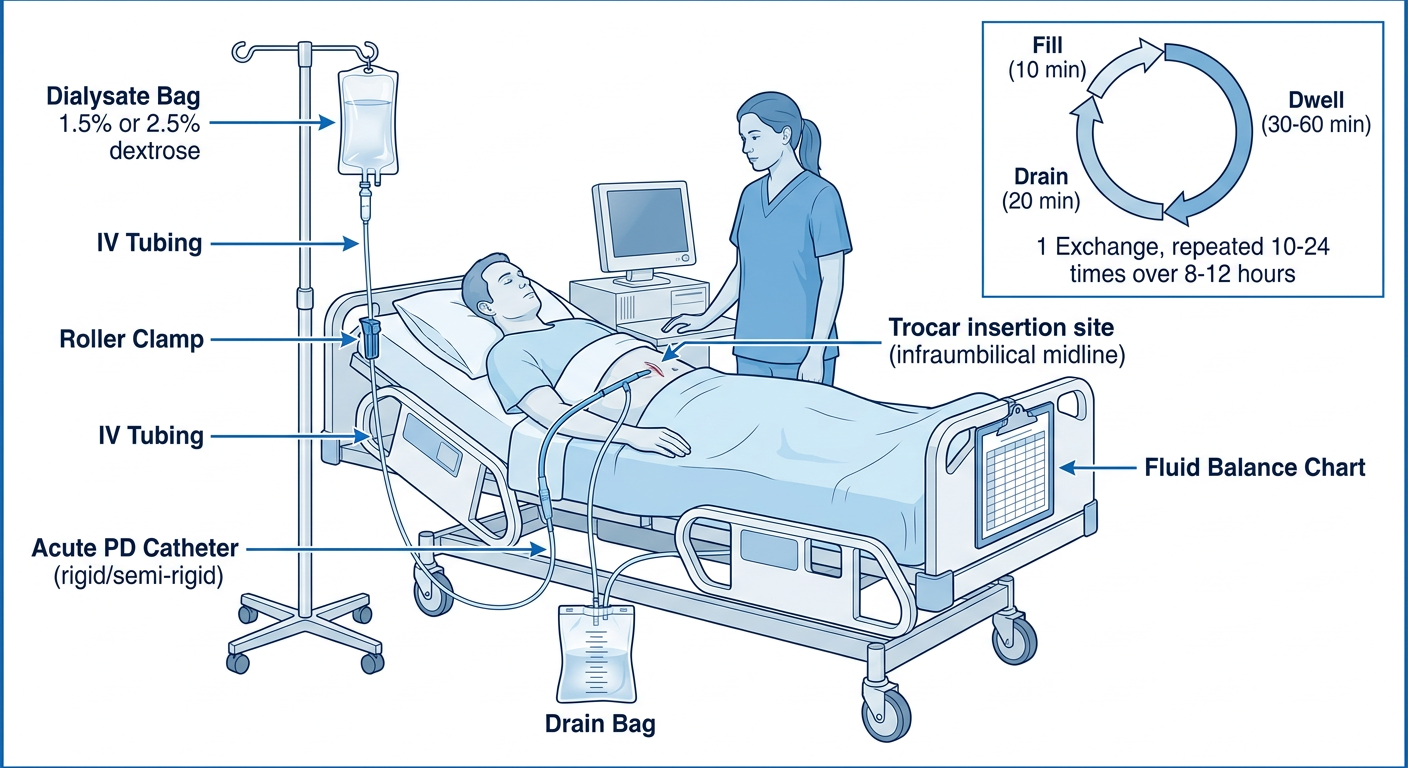
Detailed medical diagram of Acute Peritoneal Dialysis (IPD) setup in a hospital setting showing: a hospital bed with an acutely ill patient in supine position, a rigid or semi-rigid acute PD catheter inserted through the lower abdomen using a trocar/Seldinger technique, connected via standard IV tubing with a roller clamp to a dialysate bag (1-2L) hanging on an IV pole, with a drain tube going to a measuring drain bag below the bed level. Label all components: Acute PD Catheter (rigid/semi-rigid), Trocar insertion site (infraumbilical midline), Dialysate Bag 1.5% or 2.5% dextrose, Roller Clamp, IV Tubing, Drain Bag, Fluid Balance Chart on clipboard. Include a separate inset diagram showing the rapid exchange cycle timeline: Fill (10 min) → Dwell (30-60 min) → Drain (20 min) = 1 Exchange, repeated 10-24 times over 8-12 hours. Show a nurse beside the patient. Clean clinical style, blue and white color scheme, clear labels.
Medical diagram of Acute Peritoneal Dialysis setup for hospital/ICU showing: a hospital bed with critically ill patient (AKI), a rigid or semi-rigid acute PD catheter inserted through a trocar into the lower abdomen at the midline, IV pole with warm dialysate bag (1-2L) hanging high, roller clamp on fill tubing, Y-connector joining fill and drain lines, drain tubing going down by gravity to a large measuring drain bag on the floor. Label clearly: Acute PD Catheter (trocar-inserted), Fill Line with roller clamp, Dialysate Bag (1.5% glucose, 1-2L warmed to 37C), Y-connector, Drain Line, Graduated Drain Bag, Peritoneal Cavity. Show a bedside timer. Include a small table/box showing the exchange cycle: Fill 10min - Dwell 30-60min - Drain 20min, and total session of 8-12 hours. Also show a nurse documenting fluid balance. Clinical ICU setting, clean blue-white medical illustration style, all parts clearly labeled.
Acute Peritoneal Dialysis - Definition, Apparatus, Procedure, Pros & Cons
1. DEFINITION
Acute PD = a form of Intermittent Peritoneal Dialysis (IPD) performed in a hospital or clinic, using rapid, repeated short-dwell exchanges over sessions of 8-24 hours, repeated several times per week as clinically needed, with dry periods between sessions.
Key Distinctions from Chronic PD:
| Feature | Acute PD | Chronic PD (CAPD/APD) |
|---|---|---|
| Setting | Hospital / ICU / ward | Home-based |
| Goal | Temporary RRT during AKI; bridge to recovery | Permanent ESKD treatment |
| Catheter type | Acute (rigid/semi-rigid) or emergency Tenckhoff | Permanent double-cuff Tenckhoff |
| Catheter placement | Bedside / urgent; no cuff maturation needed | Surgical/peritoneoscopic; 2-4 weeks healing |
| Dwell times | Short (30-60 min) | Long (4-12 hours) |
| Sessions | 3-4 sessions/week; 8-24 hours each | Continuous, 7 days/week |
| Patient training | None; nurse-managed | Extensive (1-2 week training program) |
| Expected duration | Days to weeks | Months to years (or indefinite) |
2. INDICATIONS FOR ACUTE PD
Primary Renal Indication: Acute Kidney Injury (AKI)
| Metabolic Emergency | Target |
|---|---|
| Hyperkalaemia | Remove potassium via diffusion; life-threatening K⁺ > 6.5 mEq/L |
| Severe metabolic acidosis | Correct with lactate/bicarbonate-buffered dialysate |
| Fluid overload / pulmonary oedema | Ultrafiltration with hypertonic glucose (2.5% or 4.25%) |
| Uraemia (rising BUN/creatinine) | Diffusive clearance of urea and creatinine |
| Hyponatraemia/hypernatraemia | Electrolyte correction |
| Drug/toxin poisoning | Removal of dialyzable drugs (e.g., lithium, salicylates, methanol) |
Non-Renal Indications:
- Refractory congestive heart failure - fluid removal without hemodynamic instability
- Hepatic failure - adjunct to liver support
- Pancreatitis - historically used (controversial; peritoneal lavage principle)
- Hypo/hyperthermia - temperature correction using warm or cool dialysate
- Dialysis-associated ascites
Special Clinical Situations where Acute PD is Preferred:
- Low-resource settings where HD machines are unavailable
- COVID-19 pandemic - used when HD machines were in short supply in developed countries
- Paediatric AKI - well-tolerated in neonates and infants
- Cardiovascular instability - PD causes slower, gentler fluid/solute shifts than HD
- Severe peripheral vascular disease - no vascular access required
- Bleeding diathesis - no heparin required
- Remote/rural hospitals - simple gravity setup requires minimal equipment
3. ACUTE PD APPARATUS
Equipment List - Acute PD Setup:
| Component | Specification | Notes |
|---|---|---|
| Acute PD catheter | Rigid (stylet-guided) or semi-rigid; 28-32 Fr | Placed bedside urgently; no cuffs (or single soft cuff); temporary use |
| Permanent Tenckhoff (preferred) | Double-cuff silicone; placed surgically/percutaneously | Preferred even for acute use if time allows; better function, lower infection |
| Trocar/Stylet or Seldinger needle | For bedside blind insertion | Infraumbilical midline placement |
| Dialysate bags | 1-2 L; 1.5%, 2.5%, or 4.25% glucose | Staged bedside; multiple bags per session |
| IV pole / drip stand | Adjustable; height above bed level | Gravity fills peritoneum from above |
| Standard IV/PD infusion tubing | Sterile; clear PVC | Fill line from bag to catheter |
| Roller clamps (×2) | One on fill line; one on drain line | Manual flow control |
| Y-connector (optional) | Joins fill and drain lines at catheter | Reduces manipulation at catheter |
| Sterile drain bag | 2-3 L capacity; marked at 500 mL intervals | Hangs below bed level; gravity drainage |
| Fluid balance chart | Bedside nursing record | Records fill volume, drain volume, net UF per exchange |
| Warming facility | Warming cabinet, dry warmer, or basin of warm water | Warm bags to 37°C before use - mandatory |
| Mask, sterile gloves | For nurse performing connection/exchange | Strict aseptic technique required |
| Antiseptic supplies | Chlorhexidine, povidone-iodine, sterile gauze | Catheter insertion site and connections |
| Heparin (optional) | 500 units/L of dialysate | Added if fibrin/clots in effluent |
| Potassium supplement (if needed) | Add to dialysate | Prevent hypokalaemia with rapid exchanges |
Acute PD Catheter Types:
| Type | Description | Use |
|---|---|---|
| Rigid acute catheter | Straight trocar catheter; firm stylet; multiple side holes | Rapid emergency access; bedside insertion; prone to migration and bowel injury |
| Semi-rigid (Cook/Argyle) | Softer material; single-cuff; stylet-guided or Seldinger | Better than rigid; reduced trauma risk |
| Tenckhoff (permanent) | Double-cuff, coiled; placed surgically/peritoneoscopically | Preferred even for urgent start - better function and lower infection |
| Temporary surgical | Placed in OT under direct vision | Safest; needed if adhesions or prior abdominal surgery |
Best practice: Even in the acute setting, placing a permanent double-cuff Tenckhoff catheter (surgically or percutaneously under ultrasound/fluoroscopy) is preferred over a rigid acute catheter. Rigid catheters are associated with higher complication rates (bowel perforation, leaks, infection).
Acute Catheter Insertion - Methods:
| Method | Technique | Notes |
|---|---|---|
| Blind (Seldinger/Trocar) | Midline below umbilicus; needle → guidewire → dilator → catheter | Fastest; highest complication risk; requires full bladder emptied, empty bowel |
| Ultrasound-guided bedside | Real-time US guides needle insertion | Safer than blind; avoids vessels and bowel |
| Surgical open | Mini-laparotomy; direct vision catheter placement | Safest; needed with adhesions or prior surgery |
| Laparoscopic | Full laparoscopy; used for complex cases | Best visualization; allows omentopexy |
4. ACUTE PD PROCEDURE - STEP BY STEP
Phase 1: Pre-Procedure Preparation
- Obtain consent and explain procedure to patient/family
- Empty the bladder - catheterise if necessary (prevents bladder injury during trocar insertion)
- Check bowel - ensure not distended; NG tube if needed
- Blood tests: FBC, coagulation screen, electrolytes, BUN, creatinine
- Correct coagulopathy if severe (INR > 2.0 or platelet < 50,000 is relative concern)
- Mark insertion site: infraumbilical midline (2-3 cm below umbilicus); avoid prior surgical scars
- Prophylactic antibiotic: single dose 1st or 2nd generation cephalosporin IV before insertion
- Warm dialysate bags to 37°C
Phase 2: Catheter Insertion (Bedside Seldinger/Trocar)
1. Position patient: supine, flat
2. Prep abdomen with antiseptic; sterile drape
3. Local anaesthetic: 1% lidocaine to skin, subcutaneous tissue, fascia
4. Small stab incision at infraumbilical midline
5. Insert trocar needle → confirm peritoneal entry
(loss of resistance; aspirate for pre-existing fluid/blood/bowel gas)
6. Insert guidewire through needle
7. Remove needle; dilate tract
8. Thread catheter over guidewire/stylet toward pelvis (pouch of Douglas)
9. Remove stylet/guidewire; secure catheter at skin with suture
10. Apply sterile dressing
11. Test function: infuse 500mL warm saline → drain → confirm free flow
Phase 3: The Acute PD Exchange Procedure
STEP 1 - FILL (5-10 minutes)
│ Open fill clamp
│ 1-2L warm (37°C) dialysate flows by gravity from bag on IV pole
│ into peritoneal cavity
│ Close fill clamp when bag empties
STEP 2 - DWELL (30-60 minutes)
│ All clamps closed
│ Diffusion: urea, creatinine, K⁺, phosphate move blood → dialysate
│ Ultrafiltration: water drawn across by osmotic gradient (glucose)
│ Nurse records start time
STEP 3 - DRAIN (15-20 minutes)
│ Open drain clamp
│ Spent dialysate drains by gravity into drain bag below bed
│ Nurse records drain volume + appearance (clear vs cloudy)
│ Close drain clamp
│ Record net UF = drain volume - fill volume
│ Hang fresh bag → repeat cycle
Acute PD Session Parameters:
| Parameter | Typical Acute PD Value |
|---|---|
| Volume per exchange | 1.0-2.0 L (start with 1L; increase to 2L as tolerated) |
| Dwell time | 30-60 minutes (short; maximizes clearance per hour) |
| Drain time | 15-20 minutes |
| Exchanges per session | 10-24 |
| Session duration | 8-24 hours |
| Sessions per week | 3-4 (like HD schedule) |
| Between sessions | Peritoneum DRY |
| Glucose concentration | 1.5% (euvolaemic) / 2.5% (mild overload) / 4.25% (severe overload) |
| Heparin addition | 500 units/L if fibrin seen in effluent |
| Potassium in dialysate | Standard = zero K⁺; add KCl if hypokalaemia develops |
| Temperature | 37°C mandatory; cold dialysate causes pain and hypothermia |
Fluid Balance Monitoring Per Exchange:
Exchange # | Fill Vol | Drain Vol | Net UF | Appearance | Time
------------|----------|-----------|----------|-------------|-------
1 | 1000 mL | 950 mL | -50 mL | Clear | 06:30
2 | 1000 mL | 1150 mL | +150 mL | Clear | 07:30
3 | 2000 mL | 2300 mL | +300 mL | Clear | 08:30
...
RUNNING TOTAL UF = sum of all net UF values
Positive net UF = fluid removed from patient (desired). Negative = fluid absorbed.
Heparin Protocol for Cloudy/Fibrinous Effluent:
- Add 500-1000 units heparin per litre of dialysate
- Prevents catheter blocking from fibrin clots
- Does NOT cause systemic anticoagulation (not absorbed from peritoneum)
5. ACUTE PD - PROS AND CONS
✅ ADVANTAGES (PROS)
Clinical Advantages:
| Advantage | Explanation |
|---|---|
| Haemodynamic stability | Slow continuous fluid removal - far gentler than HD; no sudden large fluid shifts; ideal for cardiovascular instability, septic shock, cardiorenal syndrome |
| Effective for AKI | Equivalent to HD for treating hyperkalaemia and acidosis in AKI - evidence-based |
| No vascular access required | No arteriovenous fistula, graft, or central venous catheter needed; eliminates vascular access complications |
| No anticoagulation needed | Unlike HD (which requires heparin); safe in bleeding disorders, post-surgery, post-trauma |
| No blood-membrane contact | Avoids HD-related complement activation, platelet consumption |
| Continuous RRT | 24-hour sessions provide sustained gradual correction vs intermittent bolus HD |
| Paediatric advantage | Very well tolerated in neonates and infants; preferred modality for paediatric AKI |
| Temperature control | Warm dialysate (fever) or cool dialysate (hyperthermia) can be used therapeutically |
| Preserves residual kidney function | Less risk of acute haemodynamic insults than HD |
| Drug removal | Effective for small dialyzable molecules in poisoning (lithium, salicylates, methanol) |
Logistical/Resource Advantages:
| Advantage | Explanation |
|---|---|
| Minimal equipment | IV bags, tubing, clamp, pole, drain bag; gravity-driven; no electricity required |
| Low cost | Significantly cheaper than HD or CRRT |
| Low-resource settings | Widely used in low- and middle-income countries where HD unavailable |
| No dialysis machine | Frees up HD machines for other patients |
| Crisis use | Used effectively during COVID-19 when HD machines were in short supply in developed countries |
| Bedside setup | Can be established in any hospital ward, rural health centre, or field hospital |
| No specialist machine operator | Trained nurse can manage exchanges; no HD technician required |
❌ DISADVANTAGES (CONS)
Clinical Disadvantages:
| Disadvantage | Explanation |
|---|---|
| Less efficient per hour | Lower clearance rate per hour than HD or CRRT; may be insufficient for highly catabolic patients (e.g., rhabdomyolysis, severe sepsis with high urea generation) |
| Inadequate in extreme hyperkalaemia | Rapid K⁺ correction is slower than HD; not suitable when K⁺ > 7.0 mEq/L needs immediate correction |
| Glucose absorption | Each exchange delivers a glucose load → hyperglycaemia (especially with 4.25% solutions) |
| Peritonitis risk | Multiple bag changes in acute setting increases contamination risk |
| Protein loss | 5-15g albumin/day lost in effluent → worsens malnutrition in already catabolic AKI patients |
| Respiratory compromise | Fluid in abdomen raises diaphragm → reduces FRC → may worsen respiratory failure in ventilated patients |
| Contraindicated in abdominal pathology | Cannot use if recent abdominal surgery, bowel perforation, peritonitis, ileus, large bowel obstruction |
| Catheter complications | Rigid acute catheter: bowel perforation, bleeding, catheter occlusion, leaks, omental wrapping |
| Hypothermia risk | If dialysate not warmed adequately |
| Monitoring burden | Nurse must document every exchange; labour-intensive over 24-hour sessions |
| Cannot achieve exact volume targets | Less precise UF control than HD; volumes depend on membrane characteristics and gravity |
6. ACUTE PD vs OTHER RRT MODALITIES
| Feature | Acute PD | Intermittent HD | CRRT (CVVH/CVVHD) |
|---|---|---|---|
| Haemodynamic stability | Excellent | Poor | Excellent |
| Clearance efficiency | Moderate | High | Moderate-High |
| Vascular access | Not needed | Required | Required |
| Anticoagulation | Not needed | Required | Required |
| Cost | $ Lowest | $$$ | $$$$ Highest |
| Equipment | Minimal | Complex machine | Complex machine |
| Electricity | Not required | Required | Required |
| Trained operator | Nurse | HD technician + nurse | Intensivist + nurse |
| Best for | Haemodynamically unstable; low-resource; paediatric | Rapid metabolic correction; stable patient | ICU; haemodynamically unstable; precise control |
| Contraindications | Abdominal pathology; respiratory failure | Vascular access failure; bleeding | Access failure; clotting |
7. MONITORING DURING ACUTE PD
| Parameter | Frequency | Target |
|---|---|---|
| Fluid balance (net UF) | Every exchange | Documented; adjust glucose concentration |
| Blood pressure & pulse | Every 1-2 hours | Haemodynamic stability |
| Blood glucose | 4-6 hourly | Control hyperglycaemia; insulin if needed |
| Serum electrolytes (K⁺, Na⁺, HCO₃⁻) | 4-6 hourly initially | K⁺ < 5.0; correct acidosis |
| BUN / Creatinine | Daily | Monitor clearance adequacy |
| Dialysate effluent appearance | Every exchange | Clear = normal; cloudy = suspect peritonitis |
| Temperature | 4-6 hourly | Prevent hypothermia; warm all dialysate |
| Abdominal assessment | Each nursing check | Tenderness, distension, leak at exit site |
8. COMPLICATIONS OF ACUTE PD
| Complication | Cause | Management |
|---|---|---|
| Peritonitis | Touch contamination; catheter exit site | Intraperitoneal antibiotics; strict sterile technique |
| Bowel perforation | Blind trocar insertion | Immediate surgical referral |
| Haemoperitoneum | Vessel injury at insertion | Often self-limiting; if ongoing → surgical |
| Catheter blockage/outflow failure | Fibrin, omentum, migration | Heparin in dialysate; reposition; laxatives |
| Dialysate leak | Around catheter exit | Reduce volume; surgical repair if persistent |
| Hyperglycaemia | Glucose absorption | Insulin; use lower glucose concentration |
| Hypokalaemia | K⁺ removal without replacement | Add KCl to dialysate; monitor every 4-6h |
| Respiratory distress | Raised diaphragm from dialysate volume | Reduce fill volume; consider semi-recumbent position |
| Hypothermia | Cold dialysate infusion | Warm ALL bags to 37°C before infusion |
| Protein loss/malnutrition | Protein in dialysate effluent | Increase dietary protein; amino acid supplements |
9. SUMMARY - ACUTE PD AT A GLANCE
ACUTE PD
│
├── DEFINITION: Temporary RRT using peritoneum during AKI
│
├── CATHETER: Rigid acute / semi-rigid (bedside) OR Tenckhoff (preferred)
│
├── PROCEDURE: Rapid IPD exchanges
│ Fill (1-2L, 10 min) → Dwell (30-60 min) → Drain (20 min)
│ Repeated 10-24×/session over 8-24 hours
│ 3-4 sessions/week; DRY between sessions
│
├── BEST FOR:
│ ✓ Haemodynamically unstable AKI
│ ✓ No vascular access
│ ✓ Bleeding risk (no heparin)
│ ✓ Low-resource settings
│ ✓ Paediatric AKI
│ ✓ COVID-19 / resource crisis
│
├── NOT SUITABLE FOR:
│ ✗ Recent abdominal surgery / peritonitis
│ ✗ Severely catabolic patients needing high clearance
│ ✗ Extreme hyperkalaemia needing immediate correction
│ ✗ Respiratory failure worsened by abdominal fill
│
└── KEY ADVANTAGE: No machine, no vascular access, no anticoagulation,
haemodynamically gentle, works with basic nursing skills
Acute Peritoneal Dialysis (Acute PD) - Definition, Apparatus, Procedure, Pros & Cons
1. DEFINITION
"PD can be used in patients with AKI to treat hyperkalemia and acidosis in a manner equivalent to that of HD and has been used successfully in low-income countries with limited resources. During the COVID-19 pandemic, many developed countries also used PD when dialysis machines to treat AKI were in short supply." - Fischer's Mastery of Surgery, 8th Edition
2. INDICATIONS FOR ACUTE PD
Renal Indications (AKI):
| Condition | Detail |
|---|---|
| Acute Kidney Injury (AKI) | Oliguric or anuric AKI requiring renal replacement |
| Severe hyperkalemia | K⁺ not controlled by medical therapy |
| Severe metabolic acidosis | pH not correcting with bicarbonate therapy |
| Uremic complications | Uremic encephalopathy, pericarditis, bleeding |
| Fluid overload | Refractory to diuretics; pulmonary oedema |
| Severe azotemia | Rapidly rising urea/creatinine |
Absolute Renal Indications (where PD is preferred over HD):
| Indication | Why PD preferred |
|---|---|
| Vascular access failure | No HD access available |
| Haemodynamic instability | PD is gentler; no rapid fluid shifts |
| Children under 5 years | Small vessels; PD technically easier |
| Severe peripheral vascular disease | HD access not possible |
| Severe impaired cardiac function | Cannot tolerate HD haemodynamic stress |
| Bleeding diathesis | PD requires no anticoagulation (heparin) |
| Needle phobia | No vascular cannulation required |
Non-Renal Indications:
| Condition | Mechanism of Benefit |
|---|---|
| Drug/toxin poisoning | Removes dialyzable toxins via peritoneal diffusion |
| Refractory congestive heart failure | Slow, continuous fluid removal; haemodynamically safe |
| Hepatic failure | Removes ammonia and small toxins |
| Hypothermia | Instilling warm dialysate (37-40°C) warms the body core |
| Hyperthermia | Instilling cooled dialysate removes body heat |
| Pancreatitis | Clears inflammatory mediators from peritoneum (historical use) |
| Neonatal metabolic disorders | Hyperammonaemia, organic acidaemias in newborns |
Special Contexts:
| Setting | Role of Acute PD |
|---|---|
| Resource-limited settings | Gold standard RRT where HD machines, CRRT, or electricity unavailable |
| COVID-19 pandemic | Used in developed countries when HD/CRRT machines were exhausted |
| Disaster medicine | Portable, simple, gravity-driven - deployable in field hospitals |
| Malaria with AKI | Particularly in sub-Saharan Africa and Southeast Asia |
| Neonatal AKI | Very-low-birth-weight infants (even 825g) with AKI |
3. ACUTE PD APPARATUS
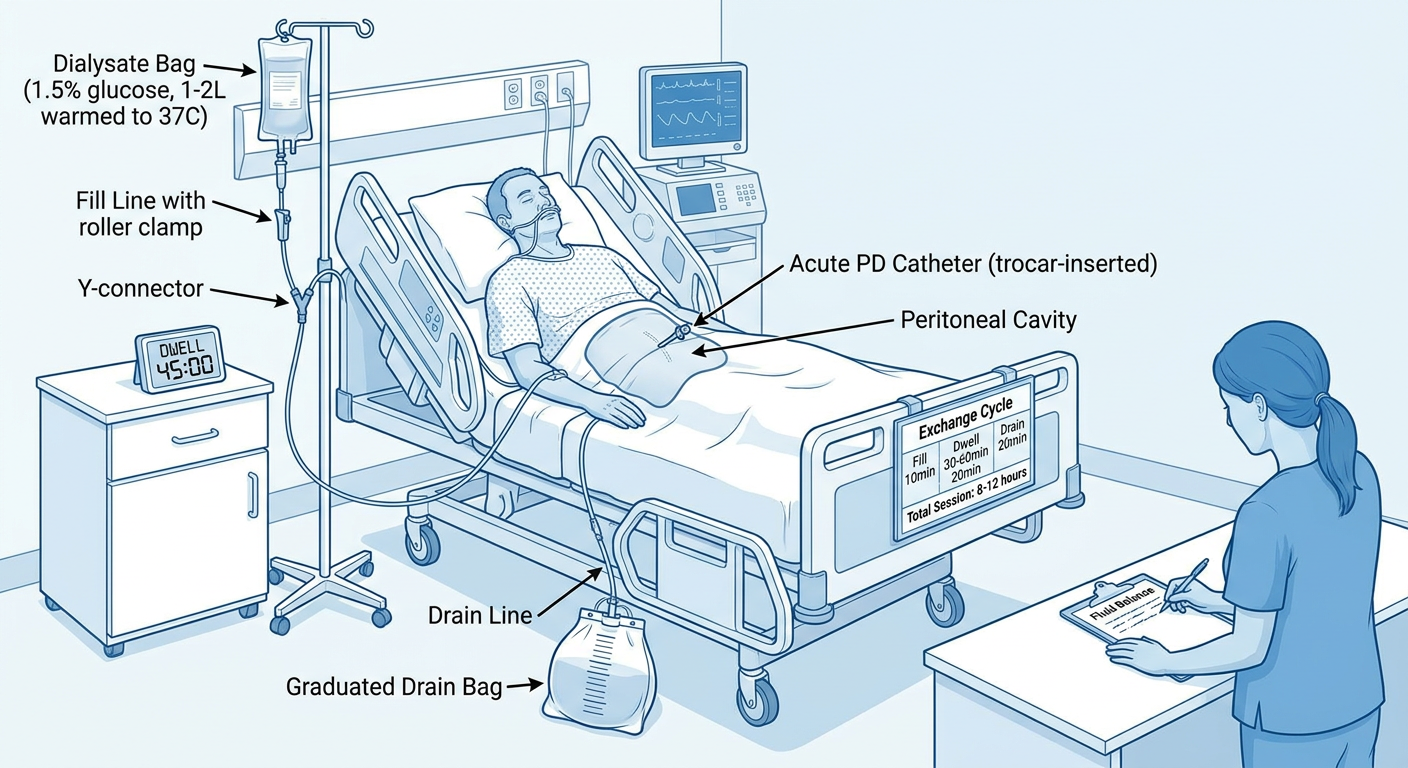
Full Equipment List:
| Component | Acute PD Specification | Notes |
|---|---|---|
| Acute PD catheter | Rigid/semi-rigid trocar catheter OR Tenckhoff silicone | Trocar for emergency; Tenckhoff for planned acute use |
| Catheter insertion kit | Trocar + cannula; or Seldinger guidewire kit | Sterile; single-use |
| Dialysate bags | 1-2 L bags, 1.5%, 2.5%, or 4.25% glucose | Standard commercial PD fluid |
| IV pole / stand | Height-adjustable | Gravity-driven fill from above |
| Fill tubing | Standard IV/PD tubing with roller clamp | Connects bag to catheter |
| Y-connector | Joins fill and drain lines to single catheter | Or use two separate lines |
| Drain tubing | Tubing from catheter to drain bag | Gravity-driven drainage downward |
| Graduated drain bag | Sterile, large (3-5L), with volume markings | Accurate fluid balance measurement |
| Fluid warmer | Warming cabinet, dry warmer, or warm water bath | Warm all bags to 37°C before use |
| Local anaesthetic | 1-2% lidocaine | Skin and subcutaneous infiltration |
| Surgical tray | Scalpel, sutures, forceps, drapes | Catheter insertion |
| Dressing materials | Sterile gauze, transparent dressing, tape | Exit site coverage |
| Heparin | 500 units/L of dialysate | Added when fibrin/clots present in effluent |
| Bedside timer / clock | Any accurate timer | Time each dwell (30-60 min) |
| Exchange chart / fluid balance sheet | Paper or electronic | Record all fill/drain volumes, times, balance |
| Gloves, mask, sterile drapes | Full aseptic setup | Mandatory throughout |
Acute PD Catheter Types:
| Type | Use | Pros | Cons |
|---|---|---|---|
| Rigid trocar catheter | True emergency, bedside | Fastest to insert; no equipment needed | High complication rate; short-term only (24-48h) |
| Semi-rigid (Cook-type) | Emergency/bedside Seldinger | Quicker than surgical; safer than rigid trocar | Some skill needed |
| Tenckhoff silicone (planned acute) | Planned urgent-start | Best long-term; lower complication rate | Needs surgical/fluoroscopic placement |
| Surgical Tenckhoff | Operating theatre | Safest; can be used long-term | Requires theatre, anaesthesia |
4. ACUTE PD CATHETER INSERTION - TECHNIQUES
A. Blind (Trocar/Seldinger) Technique - Bedside:
- Empty bladder (catheterise if needed)
- Decompress stomach (NG tube if needed)
- Position: supine; identify insertion point (midline, 2-3 cm below umbilicus or left/right paramedian)
- Mark and avoid prior surgical scars
- Skin prep with chlorhexidine; sterile drapes applied
- Infiltrate skin, subcutaneous tissue, and rectus sheath with 1-2% lidocaine
- Small 1 cm skin incision at marked point
- Insert trocar-cannula perpendicular to skin → advance with controlled pressure until "give" felt as peritoneum entered
- Remove trocar inner stylet; insert catheter through cannula → direct toward pelvis (pouch of Douglas)
- Withdraw cannula; secure catheter to skin with suture and sterile dressing
- Test function: fill 500 mL, drain - confirm free flow
B. Seldinger (Guidewire) Technique - Bedside:
- Local anaesthesia; 18G needle inserted at same midline point
- Enter peritoneum; confirm with aspiration of peritoneal fluid
- Insert guidewire through needle → remove needle
- Dilate tract over guidewire
- Advance catheter over guidewire into pelvis
- Remove guidewire; secure catheter; test fill/drain
C. Surgical / Laparoscopic Placement (planned acute):
- Performed under GA/LA in operating theatre
- Allows direct visualisation, omentum management
- Enables permanent Tenckhoff placement
- Used when urgent-start chronic PD is planned
Low-volume PD may begin within 24 hours of catheter placement if urgent RRT is needed (before normal 2-4 week healing window), using low volumes and supine positioning to minimise leak risk.
5. ACUTE PD PROCEDURE - STEP BY STEP
Preparation Before Each Session:
- Confirm correct dialysate bag (1.5% for maintenance; 2.5-4.25% for fluid removal)
- Warm all dialysate bags to 37°C (cold dialysate causes discomfort, hypothermia, and vasoconstriction)
- Add additives if prescribed:
- Heparin 500 units/L - prevents fibrin clot blockage of catheter
- KCl - only if patient is hypokalaemic (most AKI patients are hyperkalaemic - no KCl)
- Insulin - for hyperglycaemic patients using high-glucose dialysate
- Set up and prime the fill and drain tubing
- Don mask and gloves; maintain aseptic technique throughout
The Exchange Cycle (repeated 10-24 times per session):
┌─────────────────────────────────────────────────────┐
│ ACUTE PD EXCHANGE CYCLE │
│ │
│ STEP 1: FILL (5-10 minutes) │
│ Open fill clamp → 1-2L warm dialysate flows │
│ by gravity into peritoneal cavity │
│ Close fill clamp when bag empties │
│ ↓ │
│ STEP 2: DWELL (30-60 minutes) │
│ Both clamps CLOSED │
│ Diffusion: urea, creatinine, K⁺, toxins move │
│ from blood → dialysate down concentration gradient │
│ UF: water moves by osmosis into dialysate │
│ Start timer; document time │
│ ↓ │
│ STEP 3: DRAIN (15-20 minutes) │
│ Open drain clamp → spent dialysate drains │
│ by gravity into drain bag below │
│ Measure and record drain volume + appearance │
│ Close drain clamp │
│ ↓ │
│ Hang NEW dialysate bag → REPEAT cycle │
└─────────────────────────────────────────────────────┘
Session Parameters:
| Parameter | Acute PD Value |
|---|---|
| Session duration | 8-12 hours (may run 24h continuous in critical patients) |
| Exchanges per session | 10-24 |
| Fill volume | 1.0-2.0 L (start low: 500mL-1L if early acute; 2L when stable) |
| Dwell time | 30-60 minutes |
| Total fluid used/session | 20-40 L |
| Frequency | Daily or alternate days depending on clinical need |
| Glucose concentration | 1.5% (maintenance); 2.5% (mild fluid excess); 4.25% (severe fluid overload) |
| Dialysate temperature | 37°C |
| Heparin in bag | 500 units/L (if turbid effluent) |
Fluid Balance Monitoring (Critical in Acute Setting):
| Record | Why |
|---|---|
| Volume instilled (fill) | Exact fill volume prescribed |
| Volume drained (effluent) | Measure from graduated drain bag |
| Net UF = Drain - Fill | Positive = fluid removed; Negative = fluid retained (leak or malfunction) |
| Effluent appearance | Clear = normal; Cloudy = possible peritonitis; Blood-stained = trauma |
| Time started / ended | For accurate dwell timing |
| Cumulative daily balance | Running total of fluid removed |
High-Volume Acute PD:
- Fill volume: 2L per exchange
- Very short dwell: 15-30 minutes
- 24-40 exchanges per 24 hours
- Total volume: up to 40-80 L/day
- Equivalent clearance to continuous renal replacement therapy (CRRT) in some studies
6. ACUTE PD - PROS AND CONS
✅ ADVANTAGES (PROS)
Clinical Advantages:
| Advantage | Detail |
|---|---|
| Haemodynamically gentle | No rapid fluid/electrolyte shifts; safe in hypotension and cardiogenic shock |
| No anticoagulation needed | Critical advantage in post-operative, trauma, or bleeding patients where heparin is contraindicated |
| No vascular access required | Avoids arteriovenous cannulation; critical when veins are exhausted or thrombosed |
| Preserves residual kidney function | No acute volume depletion or haemodynamic stress vs HD |
| Effective for hyperkalemia & acidosis | Achieves correction comparable to HD when performed at sufficient frequency |
| Treats fluid overload | Effective even in cardiorenal syndrome and refractory CHF |
| Continuous solute removal | Gentle continuous clearance; avoids disequilibrium syndrome |
| Non-renal indications | Removes toxins, warms/cools body; no other modality can do this |
| Usable in neonates/infants | Safe even in very-low-birth-weight neonates; vascular access in neonates is extremely difficult |
| Safe in pregnancy | Avoids haemodynamic stress of HD |
Logistical/Operational Advantages:
| Advantage | Detail |
|---|---|
| No electricity required | Gravity-driven; critical in resource-poor settings and disaster zones |
| No expensive HD machine | Only requires bags, tubing, IV pole |
| Minimal skill for gravity method | Can be performed by trained nurses; no nephrologist at bedside for each exchange |
| Available globally | Usable in any hospital with basic surgical and dialysis supplies |
| Low infrastructure cost | Most cost-effective RRT modality |
| COVID-19 / surge capacity | Can rapidly scale RRT when HD/CRRT machines are depleted |
| Rapid setup | Bedside trocar insertion; PD can start within 30-60 minutes of decision |
❌ DISADVANTAGES (CONS)
Clinical Disadvantages:
| Disadvantage | Detail |
|---|---|
| Slower solute clearance than HD | Lower per-hour efficiency; standard acute PD may be insufficient in highly catabolic patients (e.g., rhabdomyolysis, tumour lysis) |
| Less efficient UF than CRRT/HD | High-volume PD needed to match CRRT clearance |
| Peritonitis risk | Multiple bag changes; breach of sterility risk at every exchange; peritonitis incidence up to 1 episode per patient-year |
| Glucose absorption | Glucose from dialysate absorbed systemically → hyperglycaemia (especially with 4.25% bags) |
| Protein loss | 5-15g protein lost per day in dialysate → worsens malnutrition in already catabolic AKI patients |
| Respiratory compromise | Intraperitoneal fluid raises diaphragm → worsens respiratory failure; critically ill/ventilated patients may not tolerate 2L fill volumes |
| Catheter complications | Blockage, kinking, leak, visceral injury (bowel/bladder perforation during trocar insertion) |
| Contraindicated in abdominal pathology | Recent abdominal surgery, peritonitis, adhesions, ostomies may preclude use |
| UF failure risk | High-transport membranes or previous peritonitis may limit UF |
Procedural / Technical Disadvantages:
| Disadvantage | Detail |
|---|---|
| Trocar insertion complications | Bowel perforation; bladder injury; vessel injury; haemorrhage |
| Labour intensive | Nursing staff must measure, record, and change bags every 30-60 minutes |
| Large fluid volumes | 20-40 L/day requires significant supply chain and storage |
| Slow correction of severe hyperkalaemia | If K⁺ >7 mmol/L with ECG changes, HD/CRRT is preferred for faster correction |
| Abdominal distension | May worsen abdominal compartment syndrome in critically ill |
7. CONTRAINDICATIONS TO ACUTE PD
| Type | Conditions |
|---|---|
| Absolute | Active intra-abdominal infection (not PD peritonitis itself); intra-abdominal catastrophe (ruptured viscus, bowel ischaemia); confirmed UF failure Type II; loss of peritoneal surface from extensive adhesions |
| Relative | Recent abdominal surgery (bowel anastomosis); abdominal wall hernias; ostomies or feeding tubes; severe obesity; diaphragmatic defects; ventriculo-peritoneal shunts; severe respiratory failure (cannot tolerate increased IAP) |
8. ACUTE PD vs OTHER RRT MODALITIES
| Feature | Acute PD | Intermittent HD | CRRT |
|---|---|---|---|
| Speed of correction | Slow-moderate | Fast | Moderate (continuous) |
| Haemodynamic tolerance | Excellent | Poor | Good |
| Anticoagulation | Not needed | Heparin usually | Heparin/citrate |
| Vascular access | Not needed | Essential | Essential |
| Machine required | No | Yes | Yes |
| Electricity | Not needed | Yes | Yes |
| Nursing burden | High (frequent changes) | Moderate | High |
| Cost | Lowest | Moderate | Highest |
| Protein loss | Yes (5-15g/day) | Minimal | Low |
| Glucose load | Yes | Minimal | Minimal |
| Available in resource-poor | Yes | Limited | No |
| Best for severe AKI | Moderate | Yes | Yes |
| Best for hypotension/shock | Yes | Less suitable | Yes |
9. SPECIAL CONSIDERATIONS IN ACUTE PD
Additives to Dialysate:
| Additive | Dose | Indication |
|---|---|---|
| Heparin | 500 units/L | Fibrinous/turbid effluent; catheter blockage |
| KCl | 2-4 mmol/L | Only if patient is hypokalaemic |
| Insulin (regular) | Per sliding scale | Hyperglycaemia from glucose-containing dialysate |
| Antibiotics (IP) | Per ISPD protocol | Peritonitis treatment |
| Do NOT add: | Calcium, potassium routinely | Standard dialysate already contains calcium; K⁺ only if levels low |
Managing Turbid (Cloudy) Effluent:
- Cloudy effluent = possible peritonitis → sample immediately for cell count, culture, Gram stain
- Diagnosis: WBC >100/mm³ with >50% neutrophils
- Empiric intraperitoneal antibiotics: gram-positive coverage (vancomycin or 1st-gen cephalosporin) + gram-negative coverage (3rd-gen cephalosporin or aminoglycoside)
Urgent Start Protocol (Catheter placed <2 weeks ago):
- Use low volume (500mL-1L) fills
- Patient supine throughout (reduces pressure on exit site)
- APD cycler preferred if available (lower leak risk than manual CAPD in this setting)
- Dry abdomen when patient is upright or mobilising
- Gradually increase fill volume to 2L over 2-4 weeks
10. SUMMARY TABLE
| Feature | Acute PD |
|---|---|
| Definition | Temporary PD for AKI or acute medical emergencies |
| Primary indication | AKI requiring urgent RRT |
| Catheter | Rigid trocar (emergency) or Tenckhoff (planned) |
| Exchange volume | 1-2 L per cycle |
| Dwell time | 30-60 minutes |
| Exchanges per session | 10-24 |
| Session duration | 8-12 hours (or continuous 24h) |
| Unique advantage | No machine, no electricity, no anticoagulation |
| Key risk | Peritonitis; catheter complications |
| Efficiency vs HD | Lower per-hour; adequate with high-volume protocol |
| Ideal setting | Resource-limited; haemodynamically unstable; no vascular access |