Asthama in detail according to standard medicine textbooks
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive data from multiple standard textbooks. Let me compile the complete, detailed response on asthma.
Asthma - A Comprehensive Overview from Standard Medical Textbooks
(Sources: Textbook of Family Medicine 9e; Murray & Nadel's Textbook of Respiratory Medicine; Harriet Lane Handbook 23e; Creasy & Resnik's Maternal-Fetal Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e)
1. Definition
Asthma is a chronic inflammatory airway disease characterized by recurring acute episodes of reversible airway obstruction, with return to normal lung function between episodes. Although bronchospasm is a component of the reversible airway obstruction, current guidelines emphasize the inflammatory pathophysiology as the primary driver - leading to mucosal edema, excessive secretions, histologic remodeling of the airways, and bronchospasm of smooth muscle origin.
"Asthma is defined as an inflammatory, episodic, obstructive lung disease that is completely reversible." - Textbook of Family Medicine 9e, p. 311
2. Epidemiology
- Affects >300 million people worldwide and causes loss of >15 million disability-adjusted life-years (DALYs) annually (Global Initiative for Asthma)
- The most common chronic disease of childhood; prevalence is increasing globally
- In the United States, ~20 million Americans (~72 per 1,000) report currently having asthma; 6.1 million children (83 per 1,000) are affected
- Results in
384,000 hospital admissions/year in the US, with an average charge >$20,000 per hospitalization ($8 billion total annually) - High-disparity condition: Hospitalization rates in the US are 3.3 times higher for Black than for White patients; low-income and uninsured patients consistently receive worse care and have worse outcomes
- Family Medicine 9e, p. 311
3. Etiology and Risk Factors
The strongest risk factors for developing asthma:
| Risk Factor | Notes |
|---|---|
| Household smoke exposure | Most important modifiable environmental trigger |
| Family history of asthma or atopy | Atopic dermatitis, allergic rhinitis |
| Family history of nasal polyps | Suggests IgE-mediated atopic disease |
| Aspirin hypersensitivity | Suggests Samter's triad / NSAID-exacerbated disease |
| Low-income/uninsured status | Linked to worse outcomes |
Common triggers: Respiratory infections (most common in children <5), inhaled allergens (dust mites, cockroach, pet dander), cigarette smoke, cold air, exercise, GERD, aspirin/NSAIDs, occupational exposures (diisocyanates, flour, latex).
4. Pathophysiology
The pathophysiology of asthma involves three interrelated processes:
4.1 Airway Inflammation
- Triggered by inhaled allergens or irritants
- Involves mast cells, eosinophils, T-lymphocytes (Th2-predominant), basophils, and dendritic cells
- Release of chemical mediators: histamine, leukotrienes (LTC4, LTD4, LTE4), prostaglandins, cytokines (IL-4, IL-5, IL-13)
- Results in mucosal edema, increased mucus secretion, and subepithelial fibrosis
- In fatal asthma: decreased lymphatic vessel density associated with airway edema and fibrotic changes (Murray & Nadel)
4.2 Bronchospasm / Airway Smooth Muscle Contraction
- Airway smooth muscle (ASM) is the cell type responsible for bronchospasm and bronchoconstriction
- Can be triggered directly (inhaled irritants) or via parasympathetic overactivity
- The pathophysiology involves local release of chemical mediators in the airway and, possibly, overactivity of the parasympathetic nervous system (Morgan & Mikhail, Clinical Anesthesiology)
- Both immunologic (IgE-mediated) and non-immunologic pathways can initiate bronchospasm
4.3 Airway Remodeling (Chronic Disease)
- With recurrent inflammation: angiogenesis, subepithelial fibrosis, extracellular matrix deposition
- Results in fixed or partially reversible obstruction in severe/longstanding disease
- VEGF-C/D-driven lymphangiogenesis occurs in chronic airway inflammation; blocking lymphangiogenesis increases airway edema (Murray & Nadel)
Physiological Consequence
Airway obstruction is most severe in expiration (dynamic collapse), making breathing difficult and fatiguing. FEV1 and peak expiratory flow rate (PEFR) are reduced; FEV1/FVC ratio falls below 70%.
5. Clinical Presentation
Symptoms
- Episodic shortness of breath
- Wheezing (typically expiratory)
- Chest tightness
- Chronic or nocturnal cough - cough-variant asthma (especially in children)
- Symptoms precipitated by exercise, cold air, allergens, or infections
- Relief with rescue inhaled beta-agonists (albuterol)
Physical Examination Findings
| Finding | Significance |
|---|---|
| Prolonged expiratory phase | Earliest sign of airway obstruction |
| Expiratory wheezing | Classic sign; can be elicited by forced expiration |
| Both inspiratory + expiratory wheeze | More severe obstruction |
| Silent chest (no wheeze) | Very severe obstruction - minimal airflow |
| Nasal flaring, pursed lips | Respiratory distress |
| Use of accessory muscles | Moderate-severe exacerbation |
| Central/acral cyanosis | Severe hypoxia |
| Pulsus paradoxus >20 mmHg | Marker of severe acute exacerbation |
6. Diagnosis
Spirometry (Gold Standard)
- Essential criterion for airway obstruction: FEV1/FVC ratio <70%
- Diagnosis of asthma requires reversibility: Improvement in FEV1 of >200 mL OR >12% after inhaled bronchodilator
- Asthma is defined as completely reversible between episodes - office spirometry during an asymptomatic period may be normal
Peak Flow Monitoring
- Measures liters/second; best of 3 attempts
- Results compared against age/sex/height nomograms, or the patient's personal best during remission
- Useful for home monitoring and self-management
Additional Diagnostics
- Methacholine challenge (bronchial provocation): Used when spirometry is normal but asthma is suspected - measures PC20 (concentration causing 20% drop in FEV1)
- Chest radiography: Not always required in classic cases; may show hyperinflation; false-positive infiltrates/atelectasis can occur during acute episodes
- Patients >40 years with new-onset asthma require complete workup to rule out other causes of airway obstruction (cardiac, malignancy, COPD)
ATS Impairment Rating (Murray & Nadel)
The American Thoracic Society grades asthma impairment across 3 domains:
- Post-bronchodilator FEV1 (scored 0-4, with <50% = score 4)
- Reversibility or airway hyperresponsiveness (PC20 value)
- Minimum medication need (no medication to daily systemic steroids)
- Total score determines Impairment Class 0-V (Class V = uncontrolled despite maximal treatment)
7. Classification by Severity (NAEPP/GINA Guidelines)
Classification is based on two domains: Impairment (symptom frequency, lung function) and Risk (exacerbation frequency):
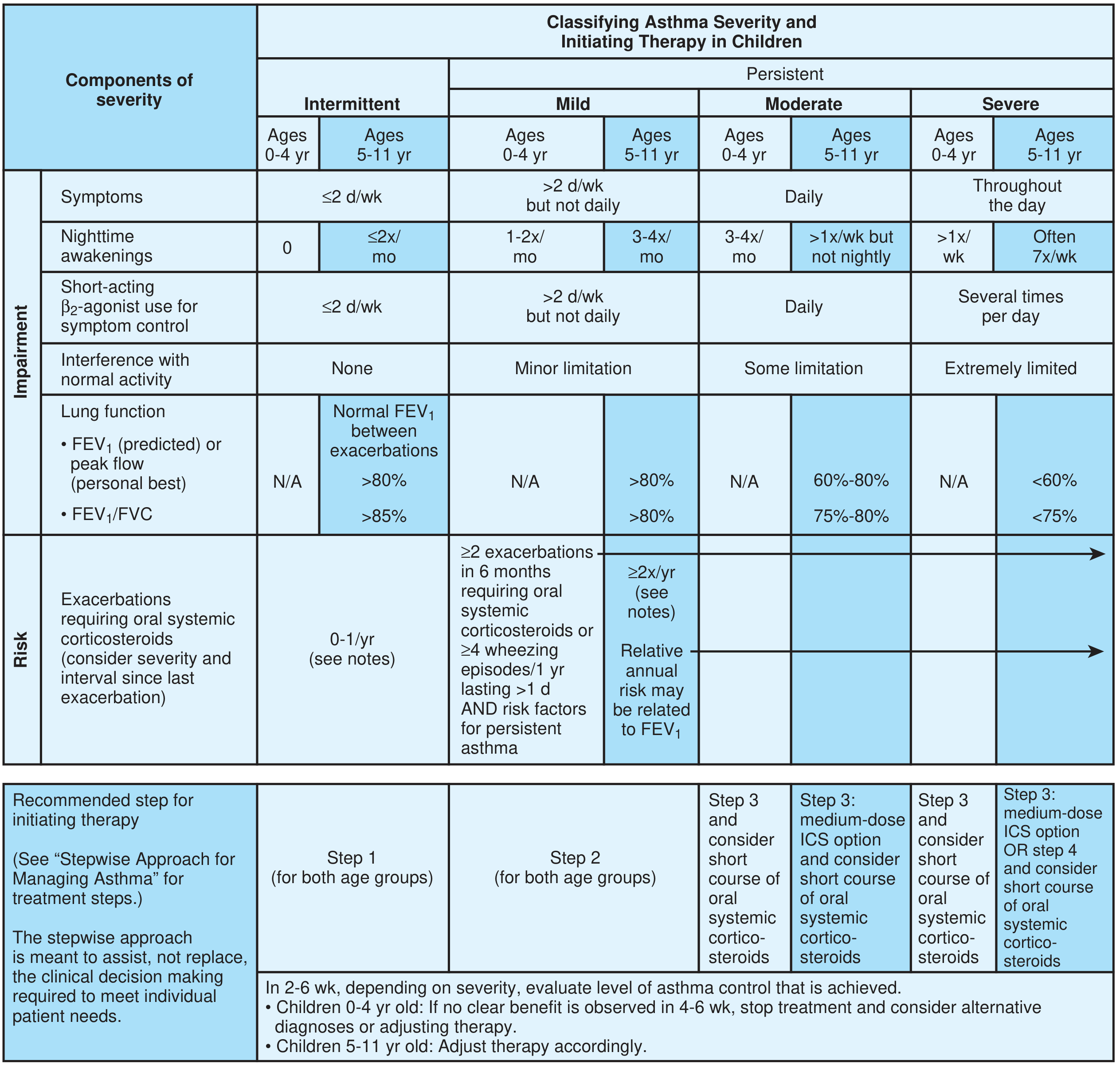
Asthma severity classification per NAEPP EPR-3, showing stepwise treatment initiation based on symptom frequency, nighttime awakenings, FEV1, and exacerbation risk - Textbook of Family Medicine 9e
Adults and Children ≥12 years
| Category | Daytime Symptoms | Nighttime Symptoms | FEV1 or PEFR | SABA Use |
|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2x/month | >80% | ≤2 days/week |
| Mild Persistent | >2 days/week, not daily | 3-4x/month | >80% | >2 days/week, not daily |
| Moderate Persistent | Daily | >1x/week, not nightly | 60-80% | Daily |
| Severe Persistent | Throughout the day | Often 7x/week | <60% | Several times/day |
Classification rule: Assign the patient to the most severe step in which ANY feature occurs.
8. Treatment
8.1 The NAEPP Framework: MAP
Every patient should have a personal asthma care plan summarized by the MAP mnemonic:
- Management plan - daily medications, peak-flow monitoring
- Action plan - what to do during acute symptoms or falling peak flow
- Prevention plan - controlling triggers, preventing flare-ups
8.2 Acute Exacerbations
First-line:
- Inhaled short-acting beta-2 agonist (SABA) - albuterol (salbutamol). A metered-dose inhaler with spacer is at least as effective as a nebulizer for delivering albuterol (meta-analysis evidence; Castro-Rodriguez & Rodrigo, 2004)
- Oxygen by nasal cannula or mask
- IV fluids for hydration
Add-on for severe airflow obstruction in ED:
- Ipratropium bromide (anticholinergic) added to albuterol produces additional bronchodilation and reduces hospital admissions (Level A evidence; Plotnick & Ducharme, 2000)
Systemic corticosteroids:
- Methylprednisolone (IV), dexamethasone (IM), prednisone/methylprednisolone (oral)
- Given as 3-5 day burst therapy; no taper needed for short courses
- Patients with chronic/severe exacerbations may require prolonged tapering
IV Magnesium Sulfate:
- Significant benefit in decreasing hospitalization rates, improving PFTs and clinical symptom scores (Cheuk et al., 2005)
- NAEPP EPR-3 recommends considering IV MgSO4 or heliox-driven albuterol nebulization in patients who fail to respond to 1 hour of conventional therapy
- Heliox alone (without albuterol) is NOT effective
Theophylline: NOT recommended in acute ED or in-hospital treatment
8.3 Long-term Controller Therapy (Stepwise Approach)
| Step | Preferred Treatment | Notes |
|---|---|---|
| Step 1 (Intermittent) | SABA PRN | No daily controller needed |
| Step 2 (Mild Persistent) | Low-dose ICS daily | ICS most effective first-line controller (Level A) |
| Step 3 (Moderate Persistent) | Low-medium ICS + LABA | LABA more effective add-on than leukotriene antagonist |
| Step 4 (Moderate-Severe) | Medium-high ICS + LABA | |
| Step 5 (Severe Persistent) | High-dose ICS + LABA ± systemic corticosteroid | Consider specialist referral |
| Step 6 | As above + biologics / omalizumab | Anti-IgE, anti-IL-5 agents |
Key points on controller therapy:
- ICS are the cornerstone - significantly reduce exacerbations and hospitalizations vs. all alternative agents (Sin et al., 2004; Level A)
- LABAs must NOT be used as monotherapy - FDA black-box warning for higher risk of death when used without ICS
- Adding LABA to low/medium ICS is preferred over increasing ICS dose to high
- Leukotriene receptor antagonists (montelukast, zafirlukast) are less effective than LABAs as add-on but useful in aspirin-sensitive or allergic asthma
- Theophylline is an acceptable but not preferred alternative to LABA as second-line add-on controller
- Most ICS benefits achieved at lower doses - always use minimum effective dose
8.4 Inhaled Corticosteroid Pharmacokinetics (Murray & Nadel)
- Low oral bioavailability is critical because up to 80% of ICS deposits in the oropharynx and is swallowed
- Oral bioavailabilities: beclomethasone ~20%, fluticasone ~1%, mometasone <1%, ciclesonide = activated only in lung tissue
- Systemic exposure risks: short-term growth suppression in children, decreased bone mineral density, possible increased cataracts
- Asthmatic patients have less systemic absorption from inhaled fluticasone than normal subjects (due to more proximal deposition from reduced airway caliber)
9. Environmental Control / Prevention
- Eliminating passive smoke exposure is the single most important environmental intervention
- Cockroach and dust mite allergen reduction combined with tobacco smoke avoidance in urban children reduced both allergen levels and asthma symptom days (Morgan et al., 2004)
- Teaching self-monitoring and self-management with an action plan is effective in reducing exacerbations (Gibson et al., 2002; Level A)
- Nurse care managers, community health workers, and peer counselors (parents of asthmatic children) improve outcomes, particularly across cultural and linguistic barriers
- The Cochrane review of 49 controlled trials found no evidence that physical or chemical methods targeting dust mite allergens alone have benefit
10. Asthma in Special Populations
Asthma in Pregnancy (Creasy & Resnik's Maternal-Fetal Medicine)
- Affects ~4% of pregnant women; 1/3 experience exacerbations during pregnancy
- Severe asthma can increase risk of: preterm labor, low birth weight, perinatal death, preeclampsia
- Normal pregnancy: progesterone causes increased tidal volume (450 → 600 mL) and minute ventilation; FEV1, PEFR, and FVC remain unchanged
- Residual volume decreases (1000 → 800 mL); mild respiratory alkalosis (PaCO2 27-32 mmHg, pH 7.45)
- FEV1 is the best parameter for assessing degree of obstruction in pregnant asthmatics
- Management principles: objective lung function assessment, fetal monitoring, avoidance of triggers, pharmacotherapy, patient education
- Most asthma medications are safe in pregnancy; poorly controlled asthma poses far greater risk to mother and fetus than the medications used to treat it
Asthma in Children <5 Years (Family Medicine 9e)
- Most common trigger: viral URI
- Diagnosis relies solely on clinical presentation (no reliable lab tests at this age)
- Long-term control therapy indicated if: consistent symptomatic treatment >2x/week, severe exacerbations <6 weeks apart, or positive Asthma Predictive Index (API)
- Positive API = ≥3 wheezing episodes in the first 3 years AND either: (1 major criterion) parental asthma or physician-diagnosed atopic dermatitis, OR (2 minor criteria) wheezing apart from colds, peripheral eosinophilia >4%, food sensitization
- MDI with spacer is as good as or better than nebulizers in children (Level A)
Asthma and Obstructive Sleep Apnea (Murray & Nadel)
- Prevalence and incidence of OSA are increased in asthmatic patients
- Obese asthmatic patients represent a particularly difficult-to-control phenotype
- OSA severity (apnea-hypopnea index) directly correlates with severe asthma exacerbations
- CPAP improves asthma quality of life, reduces exacerbations, and reduces bronchodilator use in patients with co-existing OSA
11. Monitoring and Follow-up
- Peak-flow meter: 3 measurements each morning; best value recorded; compare to personal best
- Overuse of SABA (daily use, increasing use, lack of expected effect, ~1 canister/month) = indicator of inadequate control - signals need to initiate or intensify long-term controller therapy
- Consultation with an asthma specialist recommended for moderate-severe persistent asthma; consider for mild persistent
- NAEPP guideline principle: "Step down therapy to the least medication necessary to maintain control" - gain control quickly, then step down
12. Differential Diagnosis
Conditions to exclude, especially in atypical presentations or patients >40 years:
- COPD (post-bronchodilator obstruction not fully reversible; FEV1/FVC <70% but not completely reversed)
- Vocal cord dysfunction
- Congestive heart failure ("cardiac asthma")
- Pulmonary embolism
- Foreign body aspiration (especially in children)
- Endobronchial tumor
- GERD-induced cough
- Allergic bronchopulmonary aspergillosis (ABPA)
Summary Table
| Feature | Detail |
|---|---|
| Definition | Chronic inflammatory, reversible obstructive airway disease |
| Key mediators | IgE, histamine, leukotrienes, IL-4, IL-5, IL-13 |
| Diagnosis | FEV1/FVC <70% + reversibility (>12% or >200 mL after bronchodilator) |
| Severity | Intermittent → Mild → Moderate → Severe Persistent |
| Acute Rx | SABA + ipratropium + O2 + systemic steroids ± IV MgSO4 |
| Controller Rx | ICS (cornerstone) → add LABA → biologics for severe |
| Avoid | LABA monotherapy, theophylline in acute setting |
| Monitoring | Peak flow, FEV1, SABA use frequency |
| Self-management | Written action plan (MAP), trigger avoidance, education |
Sources: Textbook of Family Medicine 9e (pp. 311-316); Murray & Nadel's Textbook of Respiratory Medicine 2-Volume; Harriet Lane Handbook 23e; Creasy & Resnik's Maternal-Fetal Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e; NAEPP Expert Panel Report 3 (2007); GINA Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.