Liver sepsis
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"liver" AND "sepsis" AND "organ dysfunction"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough answer. Here is a comprehensive synthesis:
Liver in Sepsis
Overview
Hepatic involvement in sepsis is the most common cause of jaundice in ICU patients. Approximately 50% of patients with septic shock develop some degree of liver dysfunction, which is independently associated with increased mortality. - Harrison's Principles of Internal Medicine 22E
The Liver's Role in Sepsis Defense
The liver occupies a unique anatomical and immunological position: it receives all portal drainage from the gastrointestinal tract, making it the last barrier preventing bacteria and their toxins from reaching the systemic circulation. Key players include:
-
Kupffer cells - phagocytose bacteria, release pro-inflammatory cytokines and chemokines, bind platelets, and detoxify bacterial endotoxin
-
Hepatocytes - synthesize lipopolysaccharide-binding protein (LBP), an acute-phase reactant that binds LPS and amplifies the immune response
-
Hepatic sinusoidal endothelial cells - contribute to microbial trapping
-
Neutrophils - recruited to liver sinusoids, release NETs (neutrophil extracellular traps) to trap pathogens
-
Schwartz's Principles of Surgery, 11th Ed.
Two Phases of Hepatic Involvement
Phase 1 - Ischemic/Hypoperfusion Injury
Hepatic hypoperfusion occurs early in septic shock. This leads to:
- Poor synthetic function
- Elevated serum aminotransferases (AST/ALT)
- Centrilobular (zone 3) necrosis in severe cases
Phase 2 - Inflammatory/Immune-Mediated Injury
As the liver mounts its defensive response, the immune activation becomes injurious:
-
Kupffer cell activation recruits neutrophils, which in turn injure hepatocytes
-
Hepatic endothelial cells acquire procoagulant and pro-inflammatory properties
-
Endotoxin-mediated compromise of the hepatic microvasculature causes decreased sinusoidal blood flow and fibrin microthrombus formation
-
Result: pronounced hepatocellular necrosis
-
Sleisenger & Fordtran's Gastrointestinal and Liver Disease
LPS Signaling Pathway (Gram-Negative Sepsis)
Gram-negative bacteria carry lipopolysaccharide (LPS), specifically the lipid A moiety, which is extraordinarily potent - mere nanograms injected in humans can produce manifestations of septic shock. The signaling cascade:
- LBP (produced by hepatocytes) binds lipid A → forms LBP-LPS complex
- LBP-LPS complex interacts with CD14 (membrane or soluble form)
- CD14 presents LPS to the TLR4/MD-2 transmembrane receptor complex
- TLR4 activation signals via two pathways:
- MyD88-dependent pathway → NFκB activation → pro-inflammatory cytokines (TNF-α, IL-1β, IL-6)
- TRIF-dependent (MyD88-independent) pathway → IFN-β production
The liver is also a major source of soluble CD14 in circulation, enabling LPS responses in cells that don't express membrane CD14.
- Schwartz's Principles of Surgery, 11th Ed.
Cholestasis of Sepsis
Mechanisms
Sepsis affects the liver by three main mechanisms (Robbins & Cotran):
- Direct intrahepatic bacterial infection - abscess formation, bacterial cholangitis
- Ischemia - from hypotension (especially dangerous in cirrhosis)
- Response to circulating microbial products - most common cause of cholestasis; especially with gram-negative organisms
Pathogenesis of Cholestasis
Sepsis-induced cholestasis is attributed to:
- Impaired bile formation
- Decreased bile flow in a non-obstructive pattern
- Downregulation of hepatocyte bile acid transporters by inflammatory cytokines
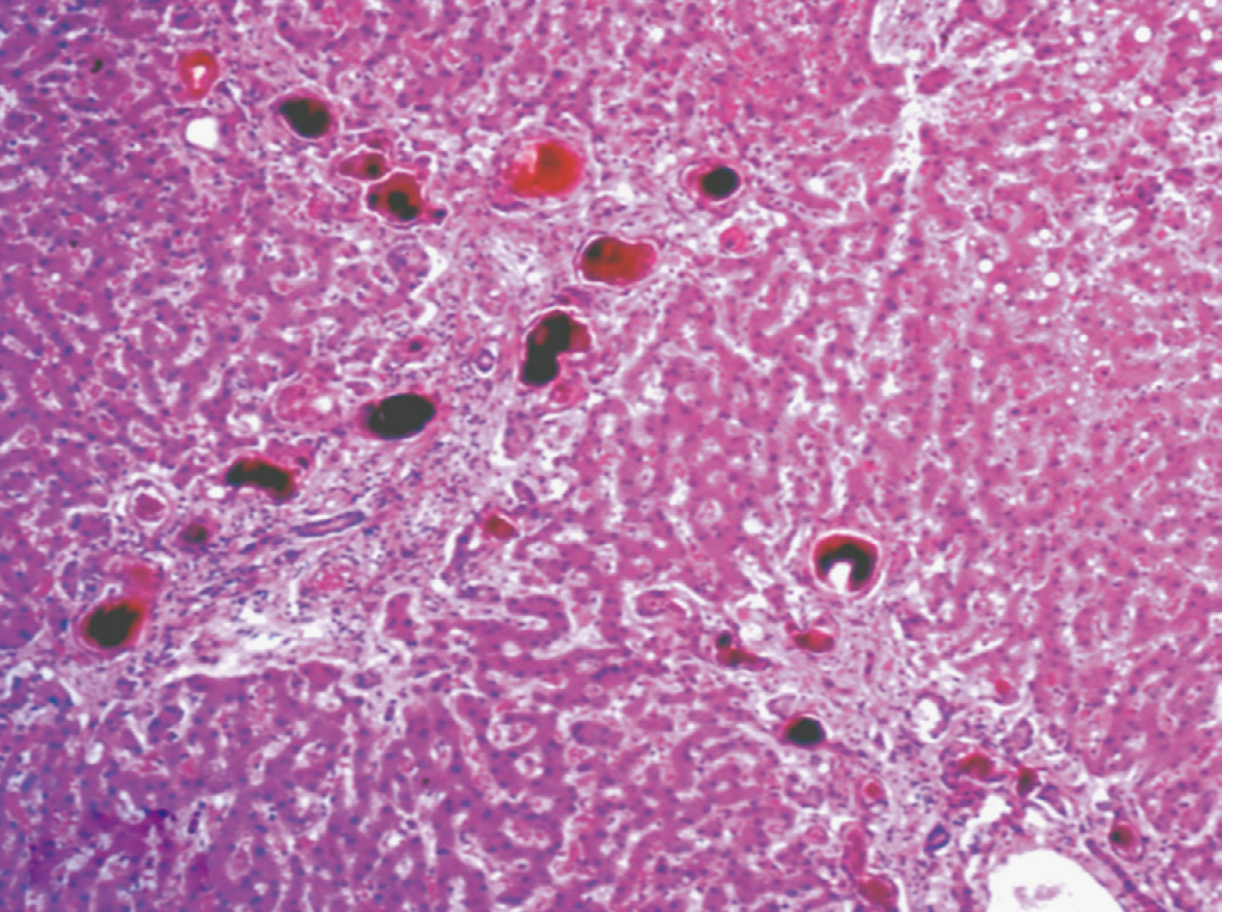
Histopathology
Characteristic morphologic findings include:
- Canalicular cholestasis with bile plugs
- Bile plugs within dilated canals of Hering and bile ductules at the portal-parenchymal interface ("ductular" or "cholangiolar cholestasis")
- Inflammation and hepatocellular injury are typically mild
Fig. 18.33 - Ductular cholestasis of sepsis (Robbins & Cotran):
In autopsy studies of fatal sepsis, hepatitis and steatosis are detected in most patients, while portal inflammation, centrilobular necrosis, hepatocellular apoptosis, and cholangitis may also be found. - Harrison's 22E
Clinical Features
| Feature | Detail |
|---|---|
| Symptoms | Right upper quadrant pain, jaundice, asterixis (severe) |
| Labs | Elevated bilirubin (predominantly conjugated), elevated ALP; elevated transaminases if marked hypotension occurred |
| Pattern | Cholestatic > hepatocellular (in typical sepsis) |
| Jaundice | Most common cause of jaundice in ICU patients |
Special Population - Neonates
Hepatic involvement in sepsis is much more common in neonates than in adults - E. coli and group B Streptococcus are the most common pathogens. Neonatal sepsis-associated cholestasis carries significant morbidity.
Cirrhosis and Sepsis
The importance of the liver in defense against systemic infections is highlighted by the fact that cirrhotic patients have:
- More frequent hospitalizations associated with sepsis
- Increased likelihood of death from sepsis compared to those with normal livers
This reflects the loss of Kupffer cell mass, impaired bacterial clearance, and coagulopathy of chronic liver disease. - Sleisenger & Fordtran
Management
- Treat the underlying infection - source control, appropriate antibiotics
- Avoid hypotension - maintain hepatic perfusion with fluid resuscitation and vasopressors
- Avoid hepatotoxic medications
- Abdominal ultrasound - perform in all septic patients with elevated serum bilirubin to evaluate for biliary obstruction, cholecystitis, and cholangitis (to rule out surgically correctable causes)
- No specific liver-directed therapy exists; recovery depends on infection control
- Harrison's Principles of Internal Medicine 22E
Lab Findings by Pattern
| Finding | Significance |
|---|---|
| Elevated conjugated bilirubin | Cholestasis of sepsis (most common) |
| Elevated ALP | Cholestatic pattern |
| Mildly elevated AST/ALT | Mild hepatocellular injury |
| Markedly elevated AST/ALT | Hepatic ischemia / "shock liver" |
| Coagulopathy (elevated PT/INR) | Loss of synthetic function |
| Cholestatic pattern + leukopenia | Classic pattern of gram-negative sepsis (Henry's Clinical Diagnosis) |
Key takeaway: The liver is both a critical defender against sepsis and a major victim of it. Its dual role - clearing bacteria/LPS via Kupffer cells while also amplifying the inflammatory cascade - means hepatic dysfunction in sepsis is both a marker of severity and a contributor to further systemic injury.
This is a shared conversation. Sign in to Orris to start your own chat.