Here are all 17 answers in complete university examination format (7 marks each), based on BD Chaurasia's Human Anatomy (Vols. 1-4) and Vishram Singh (Vols. 1-3), supplemented by Gray's Anatomy for Students:
FIRST YEAR MBBS - HUMAN ANATOMY
UPPER LIMB - COMPLETE ANSWERS (7 Marks Each)
Q1. Describe the Attachments of Rotator Cuff Muscles.
Definition: The rotator cuff (musculotendinous cuff) is a functional group of four muscles that surround the shoulder joint and blend with its capsule, providing dynamic stability.
The Four Rotator Cuff Muscles (Mnemonic: SITS)
| Muscle | Origin | Insertion | Nerve Supply | Action |
|---|
| Supraspinatus | Supraspinous fossa of scapula | Superior facet of greater tubercle of humerus | Suprascapular nerve (C4, C5, C6) | Initiates abduction (first 15°) |
| Infraspinatus | Infraspinous fossa of scapula | Middle facet of greater tubercle of humerus | Suprascapular nerve (C5, C6) | Lateral rotation |
| Teres minor | Upper two-thirds of lateral border of scapula | Inferior facet of greater tubercle of humerus | Axillary nerve (C5, C6) | Lateral rotation |
| Subscapularis | Subscapular fossa (medial surface of scapula) | Lesser tubercle and crest of humerus | Upper and lower subscapular nerves (C5, C6) | Medial rotation and adduction |
Diagram: Rotator Cuff Muscles
POSTERIOR VIEW:
Supraspinous fossa
|
Supraspinatus -----> Greater tubercle (Superior facet)
Infraspinatus -----> Greater tubercle (Middle facet)
Teres Minor -------> Greater tubercle (Inferior facet)
ANTERIOR VIEW:
Subscapular fossa
|
Subscapularis -----> Lesser tubercle
[Glenoid cavity]
Humerus head surrounded by cuff tendons
blending with joint capsule
How they form the cuff:
- The tendons of all four muscles blend with the fibrous capsule of the shoulder joint.
- Supraspinatus: covers superior aspect of joint capsule.
- Infraspinatus + Teres minor: cover posterior aspect.
- Subscapularis: covers anterior aspect.
- The inferior aspect has no cuff muscle (site of dislocation).
Clinical Significance:
- Rotator cuff tear: Most common in supraspinatus (avascular zone near insertion). Causes painful arc syndrome (60°-120° abduction).
- Subacromial impingement: Supraspinatus tendon compressed between greater tubercle and coracoacromial arch.
(Ref: BD Chaurasia Vol. 1, Chapter on Shoulder Muscles; Vishram Singh Vol. 1, Upper Limb)
Q2. Attachments, Actions and Nerve Supply of Deltoid Muscle.
Introduction:
Deltoid is a large, multipennate, triangular muscle covering the shoulder joint on all sides except medially. It is named after the Greek letter "delta" (inverted triangle).
ATTACHMENTS:
Origin (from anterior to posterior):
- Clavicular part (anterior): Anterior surface and border of lateral one-third of clavicle.
- Acromial part (middle): Lateral margin and superior surface of acromion process.
- Spinous part (posterior): Lower lip of crest of spine of scapula, as far back as the deltoid tubercle.
Insertion:
- Deltoid tuberosity on the anterolateral surface of the shaft of humerus (V-shaped roughening at the junction of upper and middle thirds).
ACTIONS:
| Part | Action |
|---|
| Anterior (clavicular) | Flexion + medial rotation of arm |
| Middle (acromial) | Abduction of arm (15°-90°) |
| Posterior (spinous) | Extension + lateral rotation of arm |
| All three together | Abduction (powerful from 15°-90°) |
- The middle deltoid is the chief abductor of the arm (works with supraspinatus).
- It assists the rotator cuff muscles in stabilizing the shoulder joint.
NERVE SUPPLY:
- Axillary nerve (C5, C6) - posterior cord of brachial plexus.
- The nerve winds around the surgical neck of the humerus within the quadrilateral space.
- It pierces the deep surface of the deltoid to supply it.
- It also gives the upper lateral cutaneous nerve of arm (sensory - over badge area/regimental badge area).
Diagram: Deltoid Muscle
Clavicle (lateral 1/3)
|
________↓_______________
| Acromion |
| Spine of Scapula |
|_________________________|
| | |
(3 heads merging)
|
Deltoid tuberosity
(shaft of humerus)
Axillary nerve (C5,C6) - from posterior cord
→ enters via quadrilateral space
→ supplies deltoid & teres minor
→ gives upper lateral cutaneous nerve of arm
Structures Deep to (Under Cover of) Deltoid:
Shoulder joint, surgical neck of humerus, axillary nerve, posterior circumflex humeral vessels, subacromial bursa, supraspinatus insertion.
Clinical Note:
- Deltoid paralysis from axillary nerve injury (e.g., surgical neck fracture) causes inability to abduct arm between 15°-90°. Area of sensory loss: over lower deltoid ("badge area").
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q3. Enumerate Structures Under Cover of Deltoid Muscle.
The deltoid muscle acts as a "tent" covering multiple important structures.
Structures Under Cover of Deltoid:
A. Bones and Joints:
- Head of humerus
- Surgical neck of humerus
- Greater tubercle of humerus
- Shoulder (glenohumeral) joint
B. Muscles:
- Supraspinatus (and its tendon)
- Infraspinatus (and its tendon)
- Teres minor (and its tendon)
- Subscapularis (anteriorly)
- Coracobrachialis (partially)
- Short and long heads of biceps brachii (partially)
C. Bursae:
- Subacromial bursa (subdeltoid bursa) - lies between the deltoid and supraspinatus; communicates with shoulder joint in 30% cases
D. Nerves:
- Axillary nerve - winds around surgical neck in quadrilateral space, supplies deltoid and teres minor
- Upper lateral cutaneous nerve of arm (terminal branch of axillary nerve)
E. Vessels:
- Posterior circumflex humeral artery (from axillary artery, 3rd part) - accompanies axillary nerve
- Anterior circumflex humeral artery (contributes to arterial anastomosis)
- Deltoid branch of thoracoacromial artery (to anterior deltoid)
Diagram:
DELTOID (Roof/Tent)
↓
┌──────────────────────────┐
│ Supraspinatus tendon │
│ Shoulder joint capsule │
│ Surgical neck of humerus │
│ Subacromial bursa │
│ Axillary nerve │
│ Post. circumflex hum. a. │
└──────────────────────────┘
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q4. Attachment of Pectoralis Major Muscle.
Introduction:
Pectoralis major is a large, fan-shaped muscle of the anterior thoracic wall forming the anterior wall of the axilla.
ORIGIN (Three Heads):
| Head | Origin |
|---|
| Clavicular head | Anterior surface of medial half of clavicle |
| Sternocostal head | Anterior surface of sternum (manubrium + body); costal cartilages of 2nd-6th ribs; aponeurosis of external oblique |
| Abdominal head (when present) | Anterior layer of rectus sheath |
INSERTION:
- Crest of the greater tubercle (lateral lip of bicipital groove) of the humerus.
- The insertion is a bilaminar tendon with a characteristic twist:
- The clavicular head passes down and inserts into the lower part of the crest.
- The sternocostal head passes up and inserts into the upper part (forming a U-shaped fold).
- This twisted arrangement increases mechanical advantage.
Diagram: Pectoralis Major Attachments
Clavicle (medial half)
|
Sternum -----+------ Clavicular head
Ribs 2-6 ----+------ Sternocostal head
Ext. oblique -+
\
\ (fan-shaped convergence)
\
→ Crest of Greater Tubercle
(Lateral lip of bicipital groove)
BILAMINAR TWISTED TENDON
Nerve Supply:
- Medial pectoral nerve (C8, T1) - supplies mainly sternocostal head.
- Lateral pectoral nerve (C5, C6, C7) - supplies mainly clavicular head.
Actions:
- Adduction and medial rotation of arm.
- Clavicular head: flexion of arm.
- Sternocostal head: extension from flexed position.
- Accessory muscle of inspiration (if arm fixed).
Clinical Note:
- Pectoralis major forms the anterior fold of axilla.
- Assessed by asking patient to push hands on hips (adduction against resistance).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q5. Attachments, Actions and Nerve Supply of Serratus Anterior Muscle.
Introduction:
Serratus anterior is the "prime mover" of scapular rotation and protrusion. It forms the medial wall of axilla and lies on the lateral thoracic wall. Called "boxing muscle" or "big swing muscle."
ORIGIN:
- Outer surfaces and superior borders of lateral aspects of ribs 1-8 (or 1-9).
- By 8 fleshy digitations that interdigitate with the digitations of the external oblique.
INSERTION:
The muscle inserts in two parts along the costal (anterior) surface of the medial border of scapula:
- Upper digitations (ribs 1, 2): Costal surface of superior angle of scapula.
- Middle digitations (ribs 3, 4): Costal surface of medial border of scapula (along its length).
- Lower digitations (ribs 5-8/9): Costal surface of inferior angle of scapula (most important - these pull the inferior angle forward and laterally).
NERVE SUPPLY:
- Long thoracic nerve (Nerve of Bell) - C5, C6, C7.
- Origin: arises from anterior rami of C5, C6, C7 in the neck.
- It runs down the superficial surface of serratus anterior on the thoracic wall.
- It is vulnerable to injury during mastectomy or axillary lymph node dissection.
ACTIONS:
| Action | Mechanism |
|---|
| Protraction (forward movement) of scapula | Pulls medial border of scapula forward |
| Rotation of scapula (upward/lateral rotation) | Lower digitations pull inferior angle forward; acromion rotates upward - essential for full abduction above 90° |
| Holds scapula against thoracic wall | Prevents winging |
| Assists in deep inspiration | Raises ribs when scapula is fixed |
Diagram: Serratus Anterior
Scapula (medial border - costal surface)
↑
| Superior angle
| ←-------- ribs 1,2
| Medial border
| ←-------- ribs 3,4
| Inferior angle
| ←-------- ribs 5-8 (most powerful)
|
──────────────────
Ribs 1-8 (lateral surface - digitations)
Long thoracic nerve (C5,C6,C7) → runs on surface of muscle
Clinical Note: Winged Scapula
- Injury to long thoracic nerve (during mastectomy, axillary dissection, stab wounds) paralyzes serratus anterior.
- Results in winging of scapula: medial border of scapula protrudes posteriorly (especially when pushing against a wall).
- Patient cannot fully abduct arm above 90° (upward rotation of glenoid is impaired).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q6. Describe the Boundaries and Contents of Carpal Tunnel. Explain Carpal Tunnel Syndrome.
CARPAL TUNNEL - Definition:
A fibro-osseous tunnel at the wrist, located deep to the flexor retinaculum, through which tendons and the median nerve pass from the forearm into the palm.
BOUNDARIES:
| Wall | Structure |
|---|
| Floor (posterior) | Concavity formed by carpal bones: scaphoid and trapezium (lateral); lunate, capitate, hamate (medial) |
| Roof (anterior) | Flexor retinaculum (transverse carpal ligament) |
| Medial wall | Hook of hamate + pisiform |
| Lateral wall | Tubercle of scaphoid + tubercle of trapezium |
CONTENTS (10 Structures):
9 Tendons + 1 Nerve:
| Contents | Detail |
|---|
| Median nerve | Lies just deep to flexor retinaculum, most lateral in the tunnel |
| 4 tendons of Flexor Digitorum Superficialis | Arranged in 2 pairs (middle + ring anterior to index + little) |
| 4 tendons of Flexor Digitorum Profundus | Lie posterior to FDS tendons |
| 1 tendon of Flexor Pollicis Longus | Lies in its own synovial sheath, most lateral |
NOTE:
- Flexor carpi radialis passes through a separate tunnel in the flexor retinaculum (not inside carpal tunnel proper).
- Palmaris longus lies superficial to the retinaculum.
- Ulnar nerve and vessels pass through Guyon's canal, not the carpal tunnel.
Diagram: Carpal Tunnel (Cross-Section)
FLEXOR RETINACULUM (Roof)
________________________________
| FPL | FDS | FDS | FDP |
| (lat)| (M,R)| (I,L)| |
| | FDP (4) | |
| Median |________________________________
| nerve ← lies laterally under retinaculum
|________________________________________|
Scaphoid Trapezium Capitate Hamate (Floor/sides)
Key: FPL=Flexor Pollicis Longus, FDS=Flexor Digitorum Superficialis, FDP=Flexor Digitorum Profundus
CARPAL TUNNEL SYNDROME (CTS):
Definition: Compression of the median nerve within the carpal tunnel, the most common entrapment neuropathy.
Causes (increase tunnel pressure):
- Idiopathic (most common)
- Pregnancy, hypothyroidism, diabetes mellitus (fluid retention)
- Rheumatoid arthritis (tenosynovitis)
- Acromegaly
- Post-colles' fracture
Clinical Features:
Symptoms:
- Burning pain and paraesthesia (tingling) in lateral three-and-a-half fingers (thumb, index, middle, lateral half of ring) - median nerve distribution.
- Pain worse at night (nocturnal pain - characteristic).
- Pain radiates up the forearm.
- Relief by hanging hand out of bed or "flick" sign.
Signs:
- Wasting of thenar eminence (later stages).
- Weakness of thumb (opposition, abduction).
- Sensory loss over lateral 3½ digits (palm side).
Special Tests:
- Tinel's sign: Tapping over carpal tunnel at wrist reproduces tingling in median nerve distribution.
- Phalen's test: Forced wrist flexion for 60 seconds reproduces symptoms.
- Reverse Phalen's test: Wrist extension worsens symptoms.
Treatment:
- Conservative: wrist splinting (neutral), corticosteroid injection, NSAIDs.
- Surgical: decompression by dividing flexor retinaculum (carpal tunnel release).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students)
Q7. Specify the Nerve Supply and Actions of Interossei of Hand.
INTEROSSEI - Introduction:
Interossei are intrinsic muscles of the hand lying between the metacarpals. There are two groups: palmar and dorsal.
A. DORSAL INTEROSSEI (4 muscles)
Attachments:
- Origin: By two heads from adjacent sides of metacarpal bones (bipennate).
- Insertion: Into bases of proximal phalanges and extensor expansions.
- 1st dorsal interosseous: Radial side of index finger (proximal phalanx + extensor expansion)
- 2nd dorsal interosseous: Radial side of middle finger
- 3rd dorsal interosseous: Ulnar side of middle finger
- 4th dorsal interosseous: Ulnar side of ring finger
Actions (DAB - Dorsal ABduct):
- Abduction of fingers away from axis of hand (middle finger as axis).
- Flexion of metacarpophalangeal joints.
- Extension of interphalangeal joints (via extensor expansion).
B. PALMAR INTEROSSEI (3 or 4 muscles - 3 according to BD Chaurasia)
Attachments:
- Origin: From the side of metacarpal shaft facing the axis of hand.
- Insertion: Base of proximal phalanx and extensor expansion of same finger.
- 1st palmar interosseous: Ulnar side of index finger
- 2nd palmar interosseous: Radial side of ring finger
- 3rd palmar interosseous: Radial side of little finger
Actions (PAD - Palmar ADduct):
- Adduction of fingers toward axis (middle finger).
- Flexion of metacarpophalangeal joints.
- Extension of interphalangeal joints.
NERVE SUPPLY of ALL Interossei:
- Deep branch of ulnar nerve (C8, T1).
- All 7 interossei (4 dorsal + 3 palmar) are supplied by the deep branch of the ulnar nerve.
Diagram: Interossei of Hand
INDEX MIDDLE RING LITTLE
| | | |
D1 D1↔D2 D2↔D3 D3↔D4
(abduct) (abduct)
Axis of hand = middle finger
DAB = Dorsal ABducts
PAD = Palmar ADducts
All supplied by: Deep branch of Ulnar nerve (C8, T1)
Combined action with Lumbricals:
- Both interossei and lumbricals together produce the "intrinsic-plus position": MCP flexion + IP extension.
- This is the position for writing ("pen grip").
Clinical Note:
- Ulnar nerve palsy causes loss of all interossei → clawing of ring and little fingers (more severe in little and ring due to loss of lumbricals to these two also).
- Froment's sign: Patient uses FPL to substitute for adductor pollicis (ulnar nerve palsy - flexes IP joint of thumb when gripping paper).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
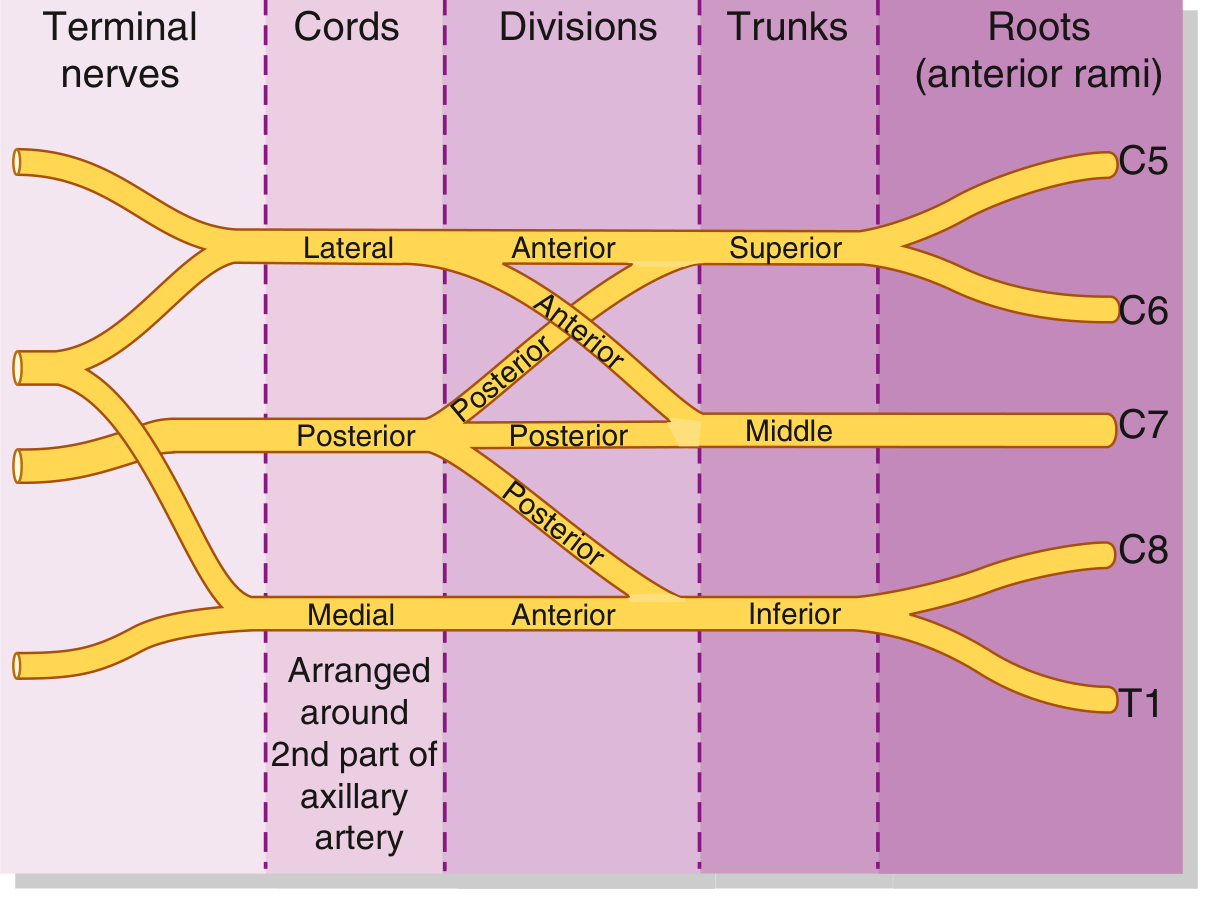
Q8. Draw and Explain the Diagram of Brachial Plexus.
BRACHIAL PLEXUS - Introduction:
The brachial plexus is a somatic nerve plexus formed from the anterior rami of C5-T1, which supply the entire upper limb. It is formed in the posterior triangle of the neck and the axilla.
COMPONENTS: ROOTS - TRUNKS - DIVISIONS - CORDS - BRANCHES
BRACHIAL PLEXUS DIAGRAM (BD Chaurasia Style)
Roots: C5 C6 C7 C8 T1
\ / | \ /
Trunks: Upper Middle Lower
(C5,6) (C7) (C8,T1)
| | |
A P A P A P (A=Anterior, P=Posterior)
Divisions: \ | | | | /
\ | | | / |
Cords: Lateral Posterior Medial
(C5,6,7) (C5-T1) (C8,T1)
\ | /
ROOTS (5 Roots):
- C5, C6, C7, C8, T1 (anterior rami)
- Pass between anterior and middle scalene muscles.
TRUNKS (3 Trunks):
| Trunk | Roots | Location |
|---|
| Superior (Upper) | C5 + C6 | Posterior triangle of neck |
| Middle | C7 | Posterior triangle |
| Inferior (Lower) | C8 + T1 | Lies on rib I |
DIVISIONS (6 Divisions):
- Each trunk divides into an anterior and posterior division (6 total).
CORDS (3 Cords):
| Cord | Formation | Relation to Axillary Artery |
|---|
| Lateral cord | Anterior divisions of upper + middle trunks (C5,6,7) | Lateral to artery |
| Medial cord | Anterior division of lower trunk (C8, T1) | Medial to artery |
| Posterior cord | Posterior divisions of ALL 3 trunks (C5-T1) | Posterior to artery |
BRANCHES:
From Roots:
- Nerve to serratus anterior (long thoracic nerve) - C5, C6, C7
- Nerve to rhomboids (dorsal scapular nerve) - C5
- Nerve to subclavius - C5, C6
From Trunks:
- Suprascapular nerve (upper trunk) - C5, C6
From Cords:
| Cord | Branches |
|---|
| Lateral cord | Lateral pectoral nerve; musculocutaneous nerve; lateral root of median nerve |
| Medial cord | Medial pectoral nerve; medial cutaneous nerve of arm; medial cutaneous nerve of forearm; ulnar nerve; medial root of median nerve |
| Posterior cord | Upper subscapular nerve; nerve to latissimus dorsi (thoracodorsal nerve); lower subscapular nerve; axillary nerve; radial nerve |
Full Diagram (Simplified):
C5─────┐
C6─────┤ UPPER TRUNK ──── ant.div. ──┐
| post.div.──┐ |
C7──── MIDDLE TRUNK ── ant.div. ──┼──┤→ LATERAL CORD → Musculocutaneous
post.div.──┼──┼┐ + Lat.root of Median N.
C8─────┐ | |||
T1─────┤ LOWER TRUNK ── ant.div.──┼──┼┘→ MEDIAL CORD → Ulnar N.
post.div.──┘ | + Med.root of Median N.
└──→ POSTERIOR CORD → Radial + Axillary N.
MEDIAN NERVE = Lateral root (C5,6,7) + Medial root (C8,T1)
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students, p. 858)
Q9. Explain the Anatomical Basis of Deformity of Erb's Paralysis.
DEFINITION:
Erb's palsy (Erb's paralysis) results from injury to the upper trunk of the brachial plexus (C5, C6), specifically at Erb's point - the junction of C5 and C6 nerve roots, just above the clavicle at the superior trunk.
ANATOMICAL BASIS OF ERB'S POINT:
- Located 2 cm above the clavicle at the junction of C5 and C6.
- At this point: anterior primary rami of C5 and C6 join to form the upper trunk.
CAUSES:
- Obstetric (most common): Excessive stretching of neck during delivery (shoulder dystocia, arm pulled over head).
- Adults: Motorcycle accidents (fall on neck + shoulder), direct blow.
MUSCLES PARALYSED (C5, C6 muscles):
All muscles supplied by C5 and/or C6:
| Nerve | Muscles Paralysed |
|---|
| Suprascapular (C5,C6) | Supraspinatus, Infraspinatus |
| Axillary (C5,C6) | Deltoid, Teres minor |
| Musculocutaneous (C5,C6) | Biceps brachii, Brachialis, Coracobrachialis |
| Upper subscapular (C5) | Subscapularis (partially) |
| Radial (C5,C6) | Brachioradialis |
THE CLASSIC DEFORMITY: "Waiter's Tip Position"
The position results from imbalance - paralyzed muscles are overpowered by their intact antagonists:
| Function Lost | Muscle Paralysed | Unopposed Muscle | Result |
|---|
| Abduction | Deltoid + Supraspinatus | Pectorals | Arm adducted |
| Flexion at elbow | Biceps, Brachialis | Triceps (C7) | Elbow extended |
| Supination | Biceps, Supinator | Pronators (C8,T1) | Forearm pronated |
| Lateral rotation | Infraspinatus, Teres minor | Subscapularis (med. rotation) | Arm medially rotated |
Diagram: Waiter's Tip / Porter's Tip Deformity
Head
|
| (neck laterally flexed opposite side at injury)
──────┤
|
Arm: |──── Adducted (pectorals unopposed)
|──── Medially rotated (subscapularis unopposed)
|──── Elbow extended (triceps unopposed)
|──── Forearm pronated (pronators unopposed)
|──── Wrist flexed
↓
APPEARANCE: Arm hangs limply at side, medially rotated,
forearm pronated like a "WAITER EXPECTING A TIP"
Sensory Loss:
- Over regimental badge area (deltoid) - lateral cutaneous nerve of arm (C5).
- Along lateral forearm - lateral cutaneous nerve of forearm (C6).
Comparison: Erb's vs Klumpke's Palsy:
| Feature | Erb's Palsy | Klumpke's Palsy |
|---|
| Roots | C5, C6 | C8, T1 |
| Cause | Neck-shoulder traction | Arm pulled upward |
| Deformity | Waiter's tip | Claw hand |
| Muscles | Shoulder + elbow muscles | Intrinsic hand muscles |
| Horner's syndrome | Absent | Present (T1 rami - sympathetics) |
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q10. Pronation and Supination.
DEFINITIONS:
- Supination: Rotation of forearm so that the palm faces anteriorly/upward (anatomical position). Radius and ulna are parallel.
- Pronation: Rotation of forearm so that the palm faces posteriorly/downward. Radius crosses over ulna.
JOINTS INVOLVED:
- Superior (proximal) radio-ulnar joint - pivot joint (head of radius in radial notch of ulna).
- Inferior (distal) radio-ulnar joint - pivot joint (head of ulna in ulnar notch of radius).
- Both joints act simultaneously (syndesmosis in middle too).
MUSCLES OF SUPINATION:
| Muscle | Nerve | Role |
|---|
| Biceps brachii | Musculocutaneous (C5,C6) | Powerful supinator (especially with elbow flexed at 90°) |
| Supinator | Posterior interosseous nerve (C6) | Supinates at all positions |
| Brachioradialis | Radial nerve | Returns forearm to midprone position |
MUSCLES OF PRONATION:
| Muscle | Nerve | Role |
|---|
| Pronator teres | Median nerve (C6,C7) | Main pronator |
| Pronator quadratus | Anterior interosseous nerve (C8) | Prime mover, works at all speeds |
| Brachioradialis | Radial nerve | Returns to midprone |
| Flexor carpi radialis | Median nerve | Assists |
Diagram: Pronation and Supination
SUPINATION: PRONATION:
Thumb side up Thumb side down
Radius parallel to ulna Radius crosses ulna
Ulna Ulna
| |
| Radius | ┌─Radius
| (parallel) | / (crossed)
| | /
PALM FACES UP PALM FACES DOWN
Axis of movement: Through head of radius (superior) +
head of ulna (inferior)
Range of Motion:
- Supination: 0°-90° (can go to 90°)
- Pronation: 0°-85°
Clinical Note:
- "Screwdriver" principle: Supination is stronger than pronation (hence screws are right-handed).
- Biceps brachii is the most powerful supinator when elbow is flexed at 90°.
- "Pulled elbow" (Nursemaid's elbow): Radial head subluxes from annular ligament in children - causes sudden pronation with elbow extended.
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q11. Median Nerve in Hand and Forearm.
MEDIAN NERVE - Origin:
- Formed by lateral root (C5,6,7 from lateral cord) and medial root (C8,T1 from medial cord) of brachial plexus.
- Forms a V (inverted) around the axillary artery.
IN THE FOREARM:
Course:
- Enters forearm by passing between the two heads of pronator teres (humeral head and ulnar head).
- Passes deep to the fibrous arch of flexor digitorum superficialis.
- Runs between FDS (anteriorly) and FDP (posteriorly) in the middle of forearm.
- At the lower forearm, becomes superficial between FDS and flexor carpi radialis tendons.
- Enters the palm via the carpal tunnel deep to the flexor retinaculum.
Branches in Forearm:
| Branch | Muscles Supplied |
|---|
| Muscular branches | Pronator teres (C6,C7) |
| Flexor carpi radialis (C6,C7) |
| Palmaris longus (C7,C8) |
| Flexor digitorum superficialis (C7,C8,T1) |
| Anterior interosseous nerve | Flexor pollicis longus (C8,T1) |
| Flexor digitorum profundus - lateral half (C8,T1) |
| Pronator quadratus (C8,T1) |
Palmar cutaneous branch:
- Arises 5 cm above wrist, passes superficial to flexor retinaculum (NOT through carpal tunnel).
- Supplies skin of lateral part of palm.
IN THE HAND:
Course:
- Exits carpal tunnel and immediately gives the recurrent (thenar) branch.
Branches in Hand:
| Branch | Supply |
|---|
| Recurrent (thenar) branch | Abductor pollicis brevis, Flexor pollicis brevis (superficial head), Opponens pollicis - the LOAF muscles |
| 1st and 2nd lumbrical nerves | 1st and 2nd lumbricals |
| Palmar digital nerves (3½ fingers) | Thumb (both sides), Index (both sides), Middle (both sides), Lateral half of ring finger - also supply nail beds and pulps |
Diagram: Median Nerve in Forearm and Hand
AXILLA → ARM (no branches) → ELBOW →
FOREARM:
Pronator teres ←────────┐
FCR, Palmaris longus ←──┤ Median nerve
FDS ←───────────────────┤ (between FDS/FDP)
FPL, lat. FDP, ←────────┤ (via AIN)
Pronator quadratus ←────┘
Palmar cutaneous branch ← above wrist (superficial to retinaculum)
CARPAL TUNNEL → HAND:
Recurrent branch:
- Abd.pollicis brevis
- Opponens pollicis
- Flex.poll.brevis (sup)
1st, 2nd lumbricals
Palmar digital nerves:
→ Both sides thumb
→ Both sides index
→ Both sides middle
→ Lat. half ring finger
(= lateral 3½ fingers)
Median Nerve Injury Summary:
| Level | Deformity | Loss |
|---|
| At elbow (above pronator teres) | "Hand of Benediction" when trying to make a fist | All above muscles |
| At wrist (carpal tunnel) | Ape thumb deformity (thenar wasting), Carpal tunnel syndrome | Thenar muscles + 1st, 2nd lumbricals + sensation |
- "Hand of Benediction": Index + middle fingers remain extended (FDP lateral half + FDS for index/middle paralysed), ring and little finger flex (ulnar innervated FDP intact).
- Ape thumb deformity (Simian hand): Thumb falls into plane of palm (opposition lost, thenar wasting).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q12. Musculocutaneous Nerve.
ORIGIN:
- Terminal branch of the lateral cord of brachial plexus.
- Root value: C5, C6, C7.
COURSE:
- Arises from the lateral cord in the axilla, lateral to axillary artery.
- Pierces the coracobrachialis muscle (first structure it supplies).
- Runs obliquely downward and laterally between biceps brachii (anterior) and brachialis (posterior).
- Reaches the lateral side of the arm just above the elbow.
- Pierces the deep fascia lateral to the biceps tendon.
- Becomes the lateral cutaneous nerve of forearm (terminal cutaneous branch).
BRANCHES AND DISTRIBUTION:
Motor Branches (in axilla and arm):
| Muscle | Root Value |
|---|
| Coracobrachialis | C5, C6, C7 |
| Biceps brachii (both heads) | C5, C6 |
| Brachialis | C5, C6 (shares with radial n. laterally) |
Sensory Branch:
- Lateral cutaneous nerve of forearm: Supplies skin of lateral surface of forearm (anterior and posterior), from elbow to the wrist.
Diagram: Musculocutaneous Nerve
LATERAL CORD (C5,C6,C7)
|
↓
Axilla → pierces CORACOBRACHIALIS
|
↓
Between BICEPS (ant.) and BRACHIALIS (post.)
|
Supplies: BICEPS BRACHII
Supplies: BRACHIALIS
|
↓ (pierces deep fascia lateral to biceps tendon)
LATERAL CUTANEOUS NERVE OF FOREARM
(supplies lateral forearm skin)
Actions of muscles supplied:
- Coracobrachialis: Flexion and adduction of arm at shoulder.
- Biceps brachii: Flexion of elbow, supination of forearm, flexion at shoulder (long head - maintains humeral head in glenoid).
- Brachialis: Pure flexor of elbow (workhorse of elbow flexion).
Clinical Notes:
- Isolated musculocutaneous nerve injury is uncommon.
- Causes: penetrating injury in axilla, shoulder dislocation, heavy backpacking ("rucksack palsy" - though usually brachial plexus).
- Effects of injury:
- Weakness of elbow flexion and supination.
- Loss of biceps jerk reflex.
- Sensory loss over lateral forearm.
- The nerve may occasionally have communications with the median nerve (variant).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students)
Q13. Specify Origin, Insertion and Distribution of Radial Nerve.
RADIAL NERVE - Origin:
- Largest terminal branch of the posterior cord of brachial plexus.
- Root value: C5, C6, C7, C8, (T1) - all roots of brachial plexus.
COURSE AND DISTRIBUTION:
In Axilla:
- Lies posterior to axillary artery.
- Gives branches: posterior cutaneous nerve of arm, nerve to long head of triceps.
- Passes between long head of triceps (medially) and the humerus.
In Arm (Radial Groove / Spiral Groove):
- Winds around the spiral groove (radial groove) of the humerus with the profunda brachii artery.
- Courses from medial-posterior to lateral-anterior.
Branches in Arm:
| Branch | Supply |
|---|
| Posterior cutaneous nerve of arm | Posterior arm skin |
| Lower lateral cutaneous nerve of arm | Lower lateral arm skin |
| Posterior cutaneous nerve of forearm | Posterior forearm skin |
| Muscular branches to triceps (all 3 heads) | Extension at elbow |
| Nerve to anconeus | Assists extension |
| Nerve to brachioradialis | Forearm semi-pronation |
| Nerve to extensor carpi radialis longus | Wrist extension |
At Cubital Fossa:
- Lies between brachialis medially and brachioradialis laterally ("radial tunnel" area).
- Divides into superficial and deep branches just in front of lateral epicondyle.
Superficial Branch:
- Sensory only.
- Runs under brachioradialis in forearm.
- Emerges at lower forearm laterally.
- Supplies dorsal skin of lateral 3½ fingers (proximal phalanges only; distal phalanges by median nerve).
Deep Branch (Posterior Interosseous Nerve - PIN):
- Motor only (after giving radial nerve branches in forearm).
- Passes between superficial and deep heads of supinator muscle (arcade of Frohse).
- Winds around lateral aspect of radius.
- Enters posterior compartment of forearm.
- Supplies all extensors in posterior compartment:
| Muscle | Action |
|---|
| Extensor carpi radialis brevis | Wrist extension |
| Supinator | Supination |
| Extensor digitorum | Extension of fingers |
| Extensor digiti minimi | Extension of little finger |
| Extensor carpi ulnaris | Wrist extension + ulnar deviation |
| Abductor pollicis longus | Abduction of thumb |
| Extensor pollicis brevis | Extension of thumb (proximal phalanx) |
| Extensor pollicis longus | Extension of thumb (distal phalanx) |
| Extensor indicis | Extension of index finger |
Diagram: Distribution of Radial Nerve
POSTERIOR CORD
|
RADIAL NERVE (C5-C8,T1)
|
├── Axilla: to triceps (long head), post. cut. n. of arm
|
├── Spiral groove of humerus: triceps (med+lat heads), brachioradialis, ECRL
|
├── Cubital fossa: DIVIDES
| | |
| SUPERFICIAL BR. DEEP BR. (PIN)
| (sensory) through supinator
| dorsal lat 3½ fingers to all extensors
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q14. Describe Root Value, Muscles Supplied and Clinical Anatomy of Radial Nerve.
ROOT VALUE:
C5, C6, C7, C8, (T1) - from posterior cord of brachial plexus.
MUSCLES SUPPLIED (Complete List):
In Arm:
- Triceps brachii (all 3 heads - extension at elbow)
- Anconeus (extension at elbow)
- Brachioradialis (flexion at elbow in midprone position)
- Extensor carpi radialis longus (wrist extension + radial deviation)
Via Deep Branch (PIN) - In Forearm (Posterior Compartment):
5. Extensor carpi radialis brevis
6. Supinator
7. Extensor digitorum communis
8. Extensor digiti minimi
9. Extensor carpi ulnaris
10. Abductor pollicis longus
11. Extensor pollicis brevis
12. Extensor pollicis longus
13. Extensor indicis proprius
CLINICAL ANATOMY - Sites of Injury:
1. Crutch Palsy (Axillary Level):
- Compression by crutch or "Saturday night palsy" (also at arm level - sleep on chair).
- All muscles paralysed.
- Wrist drop + finger drop + triceps paralysis + loss of reflexes.
- Sensory loss over posterior arm, forearm, and dorsal hand.
2. Fracture Shaft of Humerus (Spiral Groove - Most common site):
- Radial nerve injured in spiral groove by midshaft humeral fracture.
- Triceps is SPARED (branches given before spiral groove).
- Classic wrist drop: Inability to extend wrist and fingers.
- Sensory loss over anatomical snuffbox area (dorsal hand, lateral 3½ fingers - proximal phalanges).
- Triceps reflex present; brachioradialis reflex lost.
3. Posterior Interosseous Nerve (PIN) Palsy:
- At or below radial head (fracture head of radius, lipoma, arcade of Frohse compression).
- No wrist drop (ECRL spared - supraepicondylar).
- Finger drop (cannot extend fingers at MCP).
- Wrist deviates radially (ECRL intact, ECU paralysed).
- No sensory loss (PIN is purely motor).
4. Superficial Radial Nerve Compression:
- At wrist (tight watch band, de Quervain's surgery).
- Sensory loss only over dorsal lateral hand.
- No motor loss.
Diagram: Wrist Drop
Wrist: ─────┐ NORMAL position
│
Wrist drop: ──────── (gravity - no wrist extensors)
← Cannot extend wrist
← Finger drop (cannot extend at MCP)
← Thumb cannot be extended/abducted
Signs: Loss of brachioradialis jerk
Sensory: anatomical snuffbox + dorsal lateral hand
Key Clinical Points:
- Wrist drop is the hallmark of radial nerve palsy.
- Triceps is usually SPARED in shaft of humerus fractures.
- Most humeral shaft fractures with radial nerve injury recover spontaneously (neurapraxia).
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1)
Q15. Specify the Parts, Course and Branches of the Axillary Artery.
DEFINITION:
The axillary artery is the continuation of the subclavian artery from the lateral border of the first rib to the lower border of the teres major muscle (where it becomes the brachial artery).
PARTS (3 Parts - Divided by Pectoralis Minor):
- 1st Part: From lateral border of rib I to upper border of pectoralis minor.
- 2nd Part: Behind pectoralis minor.
- 3rd Part: From lower border of pectoralis minor to lower border of teres major.
RELATIONS:
- Surrounded by the three cords of brachial plexus (lateral, medial, posterior cords), hence the name.
- Axillary vein is medial.
BRANCHES (3-2-3 Rule):
1st Part (1 branch):
| Branch | Supply |
|---|
| Superior (supreme) thoracic artery | Intercostal spaces 1 and 2; pectoral muscles |
2nd Part (2 branches):
| Branch | Supply |
|---|
| Thoracoacromial artery | Divides into 4 branches: acromial, deltoid, pectoral, clavicular |
| Lateral thoracic artery | Serratus anterior; pectoral muscles; breast (lateral mammary branches) |
3rd Part (3 branches):
| Branch | Supply |
|---|
| Subscapular artery (largest branch) | Divides into: thoracodorsal (to latissimus dorsi) + circumflex scapular artery (anastomosis around scapula) |
| Anterior circumflex humeral artery | Anastomoses around surgical neck of humerus |
| Posterior circumflex humeral artery (larger) | Quadrilateral space with axillary nerve; anastomoses around shoulder |
Diagram: Axillary Artery and Branches
SUBCLAVIAN ARTERY
|
| (crosses lat. border of rib I)
↓
─────────────────────────────────────────
1st PART: ──────────────────── Superior thoracic a.
|
Pectoralis Minor (posterior relation)
|
─────────────────────────────────────────
2nd PART: ──────────────────── Thoracoacromial a.
──────────────────── Lateral thoracic a.
|
─────────────────────────────────────────
3rd PART: ──────────────────── Subscapular a.
├── Thoracodorsal a.
└── Circumflex scapular a.
──────────────────── Ant. circumflex humeral a.
──────────────────── Post. circumflex humeral a.
|
| (crosses lower border teres major)
↓
BRACHIAL ARTERY
Mnemonic: "Send The Lord's Souls Above Palms"
(Superior thoracic, Thoracoacromial, Lateral thoracic,
Subscapular, Anterior circumflex, Posterior circumflex)
Clinical Notes:
- Axillary artery can be compressed against the humerus for emergency bleeding control.
- Axillary artery aneurysm may compress cords of brachial plexus.
- In shoulder dislocation, the anterior circumflex humeral artery or the axillary artery itself may be injured.
- The posterior circumflex humeral artery accompanies the axillary nerve through the quadrilateral space.
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students, p. 842)
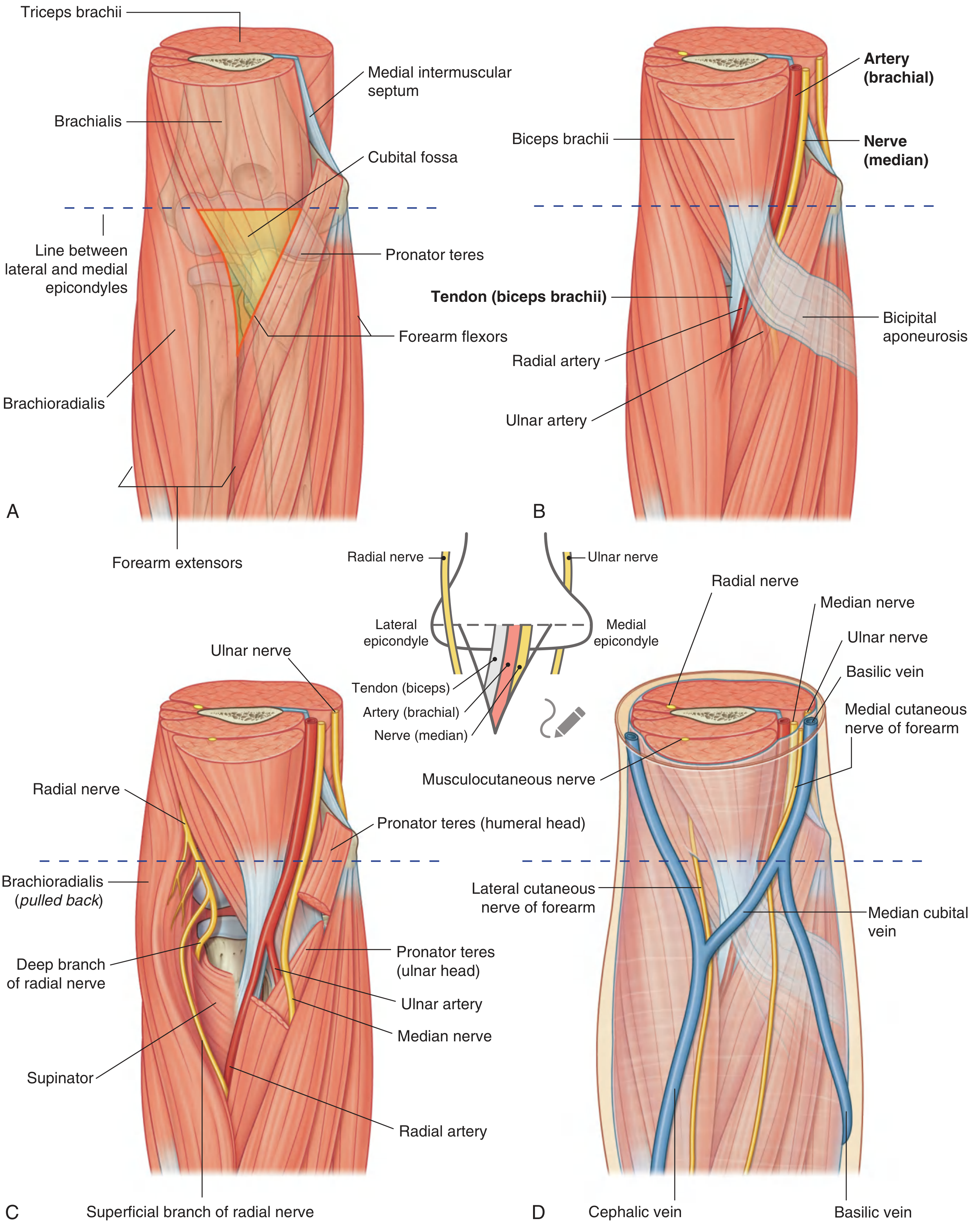
Q16. Cubital Fossa.
DEFINITION:
The cubital fossa is a triangular depression located anterior to the elbow joint (in the antecubital region), forming an important area of transition between the arm and the forearm.
BOUNDARIES:
| Boundary | Structure |
|---|
| Base (superiorly) | Imaginary horizontal line connecting medial and lateral epicondyles of humerus |
| Medial boundary | Lateral border of pronator teres (arises from medial epicondyle) |
| Lateral boundary | Medial border of brachioradialis (arises from lateral supraepicondylar ridge) |
| Apex | Where pronator teres and brachioradialis meet inferiorly |
| Floor (deep) | Brachialis muscle (medially) + Supinator muscle (laterally) |
| Roof (superficial) | Deep fascia + skin + bicipital aponeurosis (over central part) |
CONTENTS (Medial to Lateral: TAN):
Tendon of biceps, Artery (brachial), Nerve (median)
| Structure | Position |
|---|
| Median nerve | Most medial of deep structures |
| Brachial artery | Medial; bifurcates into radial + ulnar arteries at apex |
| Tendon of Biceps brachii | Central |
| Radial nerve | Deep to brachioradialis (lateral margin of fossa) |
| (Radial nerve divides here) | Into superficial and deep (posterior interosseous) branches |
Roof Contents:
- Median cubital vein - connects cephalic to basilic vein (important for intravenous access and venepuncture).
- Medial and lateral cutaneous nerves of forearm.
- Cephalic and basilic veins.
Diagram: Cubital Fossa
Lateral epicondyle Medial epicondyle
| |
|←─── BASE ───────→|
| |
Brachioradialis ←────────────────────→ Pronator Teres
(lateral wall) (medial wall)
\ /
\ /
──────APEX──────
CONTENTS (deep, lateral to medial):
Radial n. Biceps tendon Brachial a. Median n.
(under brachioradialis)
ROOF: Deep fascia + Bicipital aponeurosis + skin
FLOOR: Brachialis + Supinator
SUPERFICIAL (in roof): Median cubital vein, cutaneous nerves
Applied Anatomy:
- Venepuncture: Median cubital vein in cubital fossa roof is the standard site for IV cannulation, blood sampling. The bicipital aponeurosis protects the brachial artery and median nerve from inadvertent puncture.
- Blood pressure measurement: Brachial artery in cubital fossa is the site for auscultation (Korotkoff sounds).
- Brachial artery injury: Results in Volkmann's ischaemia → compartment syndrome → Volkmann's ischaemic contracture (flexion deformity of forearm and hand).
- Biceps tendon rupture: Palpable gap in cubital fossa.
- Radial nerve entrapment in radial tunnel (lateral to cubital fossa) can cause lateral epicondylitis-like pain.
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students, p. 889)
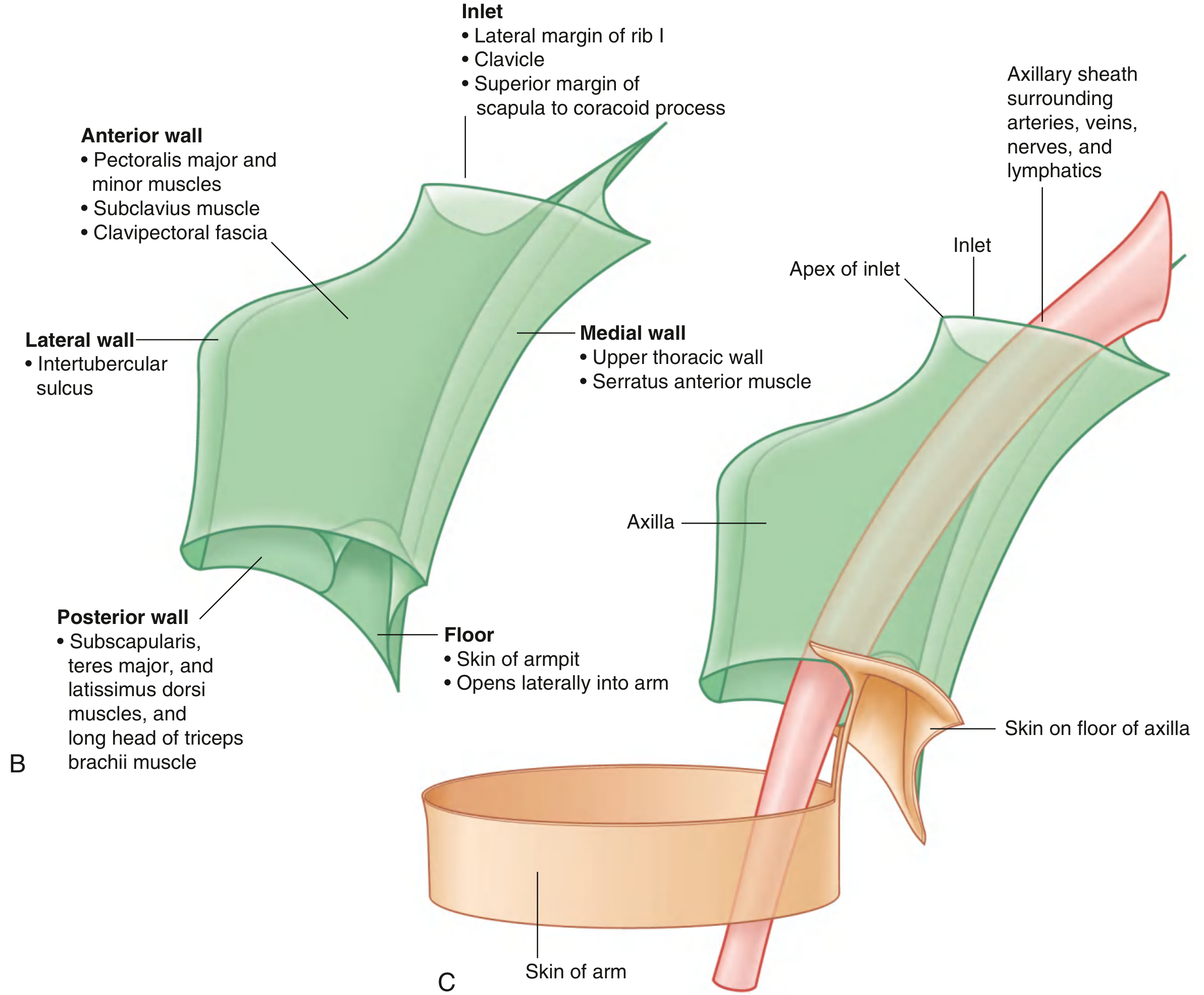
Q17. Axilla - Boundaries, Contents and Applied Anatomy.
DEFINITION:
The axilla is a pyramidal space (like an inverted 4-sided pyramid) at the junction of the arm and thorax, forming the gateway to the upper limb through which all major neurovascular structures pass.
BOUNDARIES (4 Walls + Apex + Base):
APEX (Inlet):
- Bounded by: posterior surface of clavicle (anteriorly) + superior border of scapula (posteriorly) + lateral border of rib I (medially).
- Through the apex pass: axillary vessels, brachial plexus trunks.
BASE (Floor):
- Skin, superficial fascia, and axillary fascia between the anterior and posterior folds.
- Covered by coarse axillary hair.
| Wall | Structures |
|---|
| Anterior wall | Pectoralis major (superficial) + Pectoralis minor + Subclavius + Clavipectoral fascia |
| Posterior wall | Subscapularis (upper) + Teres major (lower) + Latissimus dorsi (lower, most inferior) |
| Medial wall | Serratus anterior on lateral surface of ribs 1-4 + intercostals |
| Lateral wall | Narrow; intertubercular groove of humerus (bicipital groove); biceps brachii (short head) + coracobrachialis |
Diagram: Axilla (Walls)
APEX (Inlet)
↑
┌─────────────────────┐
Anterior │ Pect. Major │ Posterior
Wall │ Pect. Minor │ Wall
│ Subclavius │ Subscapularis
│ │ Teres Major
│ │ Lat. Dorsi
└─────────────────────┘
Medial wall: Serratus ant. on ribs
Lateral wall: Bicipital groove (humerus)
↓
BASE (Floor)
Skin + Axillary fascia
[Pyramidal space - apex directed upward toward neck]
CONTENTS of Axilla:
A. Axillary Artery (and branches):
- Divided into 3 parts by pectoralis minor.
- 6 branches (1+2+3): Superior thoracic, Thoracoacromial, Lateral thoracic, Subscapular, Ant. and Post. circumflex humeral.
B. Axillary Vein:
- Medial to axillary artery.
- Begins at lower border of teres major.
- Receives cephalic vein and tributaries.
- Becomes subclavian vein at lateral border of rib I.
C. Brachial Plexus:
- In axilla: the cords and their terminal branches.
- Lateral cord (C5,6,7): musculocutaneous nerve + lateral root of median nerve + lateral pectoral nerve.
- Medial cord (C8,T1): ulnar nerve + medial root of median nerve + medial cutaneous nerves + medial pectoral nerve.
- Posterior cord (C5-T1): axillary nerve + radial nerve + subscapular nerves + thoracodorsal nerve.
D. Axillary Lymph Nodes (5 Groups):
| Group | Location | Drainage |
|---|
| Anterior (pectoral) | Along lateral thoracic vessel | Breast (lateral), chest wall |
| Posterior (subscapular) | Along subscapular vessel | Back, posterior shoulder |
| Lateral (brachial) | Along axillary vein | Entire upper limb |
| Central | Fat in center of axilla | Receives from anterior, posterior, lateral groups |
| Apical (infraclavicular) | At apex, along axillary vein | All other groups; drains to subclavian trunk |
E. Other Contents:
- Axillary sheath (prolongation of prevertebral fascia enclosing artery, vein, cords).
- Axillary fat (fills space).
- Tail of Spence (axillary tail of breast - extends into axilla).
- Long thoracic nerve (on serratus anterior).
- Intercostobrachial nerve (T2 lateral cutaneous branch).
APPLIED ANATOMY:
-
Breast cancer and axillary lymph nodes:
- Lymph from lateral breast drains to axillary nodes (especially anterior/pectoral group).
- Sentinel node biopsy and axillary clearance are done in breast cancer staging.
- Injury to long thoracic nerve during axillary clearance → winging of scapula.
- Injury to thoracodorsal nerve → weakness of latissimus dorsi.
- Injury to intercostobrachial nerve (T2) → sensory loss over medial upper arm.
-
Axillary nerve injury (surgical neck of humerus fracture or shoulder dislocation):
- Loss of deltoid action (abduction 15°-90°).
- Loss of sensation over badge area.
-
Brachial plexus injury:
- Penetrating injuries in axilla can damage cords.
- Pancoast tumor invades lower trunk (Klumpke's type lesion + Horner syndrome).
-
Axillary artery aneurysm or injury:
- Can compress brachial plexus cords.
- Injury in shoulder dislocation.
-
Crutch palsy:
- Pressure on axillary contents from ill-fitting crutch → brachial plexus (posterior cord) compression → wrist drop.
-
Axillary vein thrombosis:
- Paget-Schroetter syndrome: effort thrombosis of axillary vein in young athletes.
(Ref: BD Chaurasia Vol. 1; Vishram Singh Vol. 1; Gray's Anatomy for Students, pp. 841-842)
KEY DIAGRAMS SUMMARY (For Exam Use)
Brachial Plexus - Parts and components (Gray's Anatomy for Students)
Axilla - Walls and boundaries (Gray's Anatomy for Students)
Cubital Fossa - Margins and Contents (Gray's Anatomy for Students)
QUICK REVISION MNEMONICS
| Topic | Mnemonic |
|---|
| Rotator cuff muscles | SITS (Supraspinatus, Infraspinatus, Teres minor, Subscapularis) |
| Cubital fossa contents (medial to lateral) | TAN (Tendon, Artery, Nerve) + Radial nerve lateral |
| Axillary artery branches | STL-SAP (Superior thoracic, Thoracoacromial, Lateral thoracic - Subscapular, Ant. circumflex, Post. circumflex) |
| Brachial plexus components | R-T-D-C-B (Roots, Trunks, Divisions, Cords, Branches) |
| Dorsal interossei | DAB (Dorsal ABduct) |
| Palmar interossei | PAD (Palmar ADduct) |
| Median nerve hand muscles | LOAF (Lumbricals 1&2, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis superficial head) |
| Erb's palsy roots | C5, C6 = "C5-C6 - Waiter's Tip" |
| Klumpke's palsy roots | C8, T1 = "C8-T1 - Claw hand" |
All 17 answers are based on BD Chaurasia's Human Anatomy (Vols. 1-4) and Vishram Singh (Vols. 1-3), cross-referenced with Gray's Anatomy for Students. Good luck with your first-year anatomy exam!