Intussusception & Volvulus General surgery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Now I have comprehensive information from multiple surgical textbooks. Let me compile the full structured response.
Intussusception & Volvulus - General Surgery
INTUSSUSCEPTION
Definition & Terminology
Intussusception is the "telescoping" of intestine, where a proximal segment of bowel (the intussusceptum) invaginates into a distal segment (the intussuscipiens). The advancing edge of the intussusceptum is called the lead point.
- Bailey & Love's Short Practice of Surgery, 28th Ed.
- Fischer's Mastery of Surgery, 8th Ed.
Epidemiology
| Feature | Pediatric | Adult |
|---|---|---|
| Age peak | 6-9 months (range 3 months - 3 years) | Any age, typically older |
| Incidence | ~56/100,000 per year (US) | Rare |
| Etiology | Mostly idiopathic (>96%) | Almost always pathological lead point |
| Lead point nature | Viral lymphoid hyperplasia (Peyer patches) | Malignant in ~50% of cases |
Types by Location
- Ileocolic (most common, >80%) - begins proximal to ileocaecal valve, apex in ascending or transverse colon
- Ileoileal - small bowel to small bowel; often transient, self-resolving
- Jejunoileal
- Colocolic
- Ileocaecal - the ileocaecal valve itself may serve as the lead point
Pathophysiology
The invaginating segment carries its mesentery with it. This leads to:
- Venous and lymphatic obstruction
- Oedema and mucosal congestion ("redcurrant jelly" stool)
- Arterial compromise if untreated → ischaemia → gangrene → perforation
Lead Points
Benign (pediatric):
- Lymphoid hyperplasia / Peyer patches (post-viral - most common)
- Meckel diverticulum
- Enteric duplication cyst
- Hamartoma (Peutz-Jeghers syndrome)
- Cecal polyp
- Burkitt lymphoma (rare)
- Appendiceal pathology (appendicitis, carcinoid)
Pathological (adult, ~50% malignant):
- Colonic or small bowel carcinoma
- Lymphoma
- Metastatic deposits
- Lipoma
- Inflammatory polyps
Pathological lead points are more common in children >2 years and with recurrent intussusception.
Clinical Features (Pediatric - Classic Triad)
- Colicky pain - episodic, infant draws up legs
- Vomiting
- "Redcurrant jelly" stool - blood and mucus per rectum (late sign)
Examination:
- Between episodes: child initially appears well
- Dehydration
- Abdominal distension
- Palpable right upper quadrant mass (the intussusceptum)
- Paucity of gas in right iliac fossa
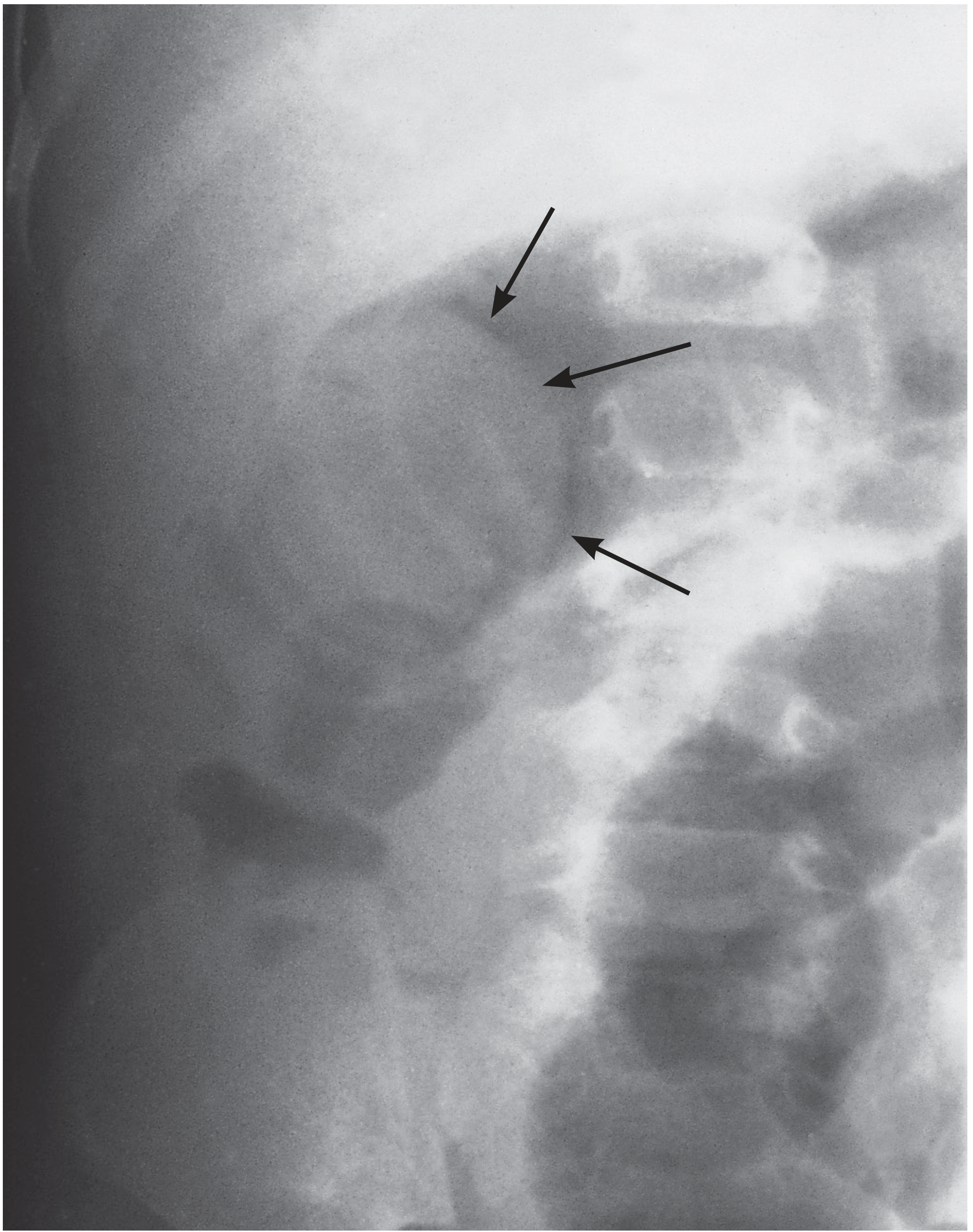
Investigations
| Investigation | Finding |
|---|---|
| Plain AXR | Small bowel obstruction; soft-tissue mass; paucity of gas in RIF; meniscus sign |
| Abdominal USS | Concentric "target sign" (axial view); "pseudo-kidney" sign (longitudinal view) - first-line investigation |
| CT abdomen | Confirms in adults; identifies lead point |
Prognostic note: A normal bowel gas pattern on AXR predicts the highest success rate for enema reduction. Obstruction on AXR is associated with significantly lower reduction success rates.
Intraoperative Photo: Ileocolic Intussusception

Ileocolic intussusception causing small bowel obstruction - Bailey & Love's Short Practice of Surgery
Treatment
Resuscitation First (Always)
- IV fluids
- Broad-spectrum antibiotics
- Nasogastric drainage
Non-Operative Reduction (First-line, if no contraindications)
Air (pneumatic) reduction enema - success recognised by air flowing into the small bowel through the ileocaecal valve
Air enema reduction - Bailey & Love's Short Practice of Surgery
- >70% are reducible non-operatively
- A key criterion: reflux of the reduction medium through the ileocaecal valve into the terminal ileum confirms complete reduction
- Delayed repeat enema (2-4 hours later) is reasonable if partial reduction was achieved on first attempt
Contraindications to enema reduction:
- Peritonitis
- Perforation
- Haemodynamic shock
Operative Management
Indicated when:
- Non-operative reduction fails
- Known pathological lead point
- Peritonitis or shock
- Ischaemia/gangrene (strangulation)
Approach: open or laparoscopic
- Irreducible, infarcted, or lead-point-driven intussusception requires bowel resection
- Colonic perforation during pneumatic reduction is rare but requires emergency surgery
Recurrence
- ~5% after non-operative reduction
- Recurrence should raise suspicion of a pathological lead point
VOLVULUS
Definition & Pathophysiology
Volvulus is a twist (axial rotation) of a bowel segment about its mesentery.
- >180° torsion → luminal obstruction
- >360° torsion → vascular occlusion (mesenteric vessels)
Mechanism of ischaemia:
- Mechanical twisting obstructs mesenteric veins → thrombosis
- Increasing intraluminal pressure (bacterial fermentation/gas) impairs capillary perfusion
- Arterial occlusion if torsion is severe enough
Classification
Primary volvulus - congenital cause:
- Congenital malrotation of gut
- Abnormal mesenteric attachments or congenital bands
- Examples: volvulus neonatorum, caecal volvulus, sigmoid volvulus
Secondary volvulus (more common in adults):
- Rotation around an acquired adhesion or stoma
Sites of Volvulus
| Site | Notes |
|---|---|
| Sigmoid colon | Most common in adults; requires a mesentery to allow twisting |
| Caecum | Second most common; requires a hypermobile caecum |
| Transverse colon | Rare; requires a persistent dorsal mesentery |
| Splenic flexure | Rare |
| Small intestine | Neonatal midgut volvulus (life-threatening) |
Sigmoid Volvulus
Predisposing Factors

Causes predisposing to sigmoid volvulus - Bailey & Love's Short Practice of Surgery
Three anatomical prerequisites:
- Overloaded pelvic colon (elongated sigmoid)
- Long pelvic mesocolon
- Narrow posterior mesenteric attachment
Additional factors: high-residue diet, constipation, adhesions, chronic psychotropic drug use, pelvic masses, pregnancy
Demographics:
- Common in West/East Africa - most common cause of large bowel obstruction in indigenous black African population, seen in younger patients
- In Western countries - predominantly elderly, institutionalised, with comorbidities
- Rotation is almost always anticlockwise
Clinical Presentation
- Massive colonic distension - the key feature
- Pain is unusual in sigmoid volvulus; if present, it is a warning sign of ischaemia
- History may not always be forthcoming given frailty of typical patients
- Can be classified as:
- Fulminant: sudden onset, severe pain, early vomiting, rapidly deteriorating
- Indolent: insidious onset, slow progressive, less pain, late vomiting
Investigations
Plain AXR: Useful but not always diagnostic - shows massive distension of a dilated loop, often appearing as an inverted "U" or "coffee bean" sign
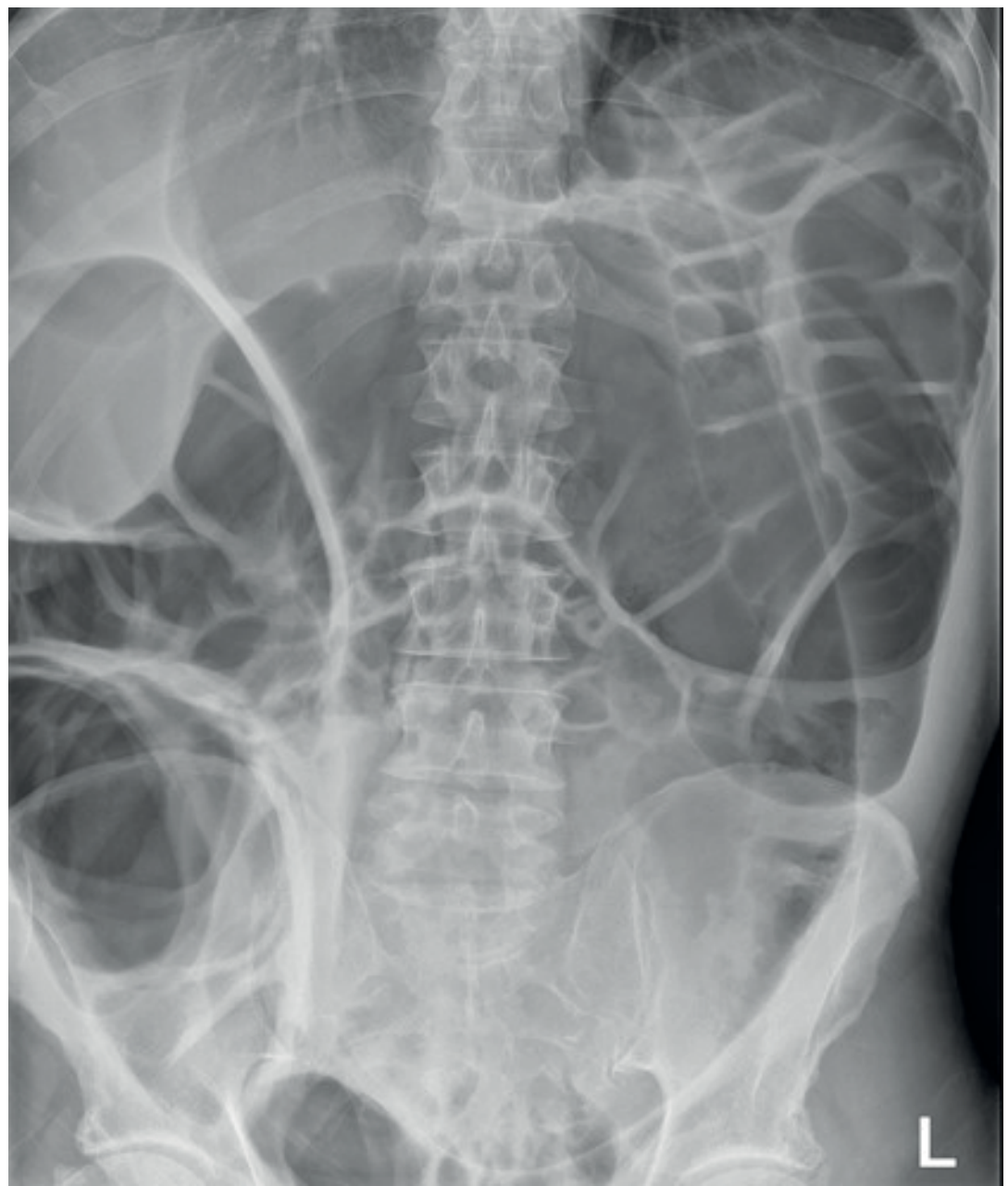
AXR: sigmoid volvulus - massive colonic distension - Bailey & Love's Short Practice of Surgery
CT: Mainstay of diagnosis - shows the "whirl sign" (twisted bowel and mesentery, proportional to degree of rotation)
Water-soluble contrast enema: Shows "bird's beak" deformity at the site of the twist
Treatment
Step 1 - Non-operative decompression (first-line):
- Rigid sigmoidoscope or colonoscope
- Allows direct vision, assessment of mucosal viability, and derotation
- On successful derotation: insert a well-lubricated flatus tube and leave for 2-5 days
Findings indicating ischaemia (abandon derotation - immediate surgery):
- Bloody bowel contents
- Discoloured mucosa
- Attempted derotation in this situation risks circulatory collapse and death
Step 2 - Elective definitive surgery (high recurrence rate necessitates this):
- Resection of the entire sigmoid colon
- Can be done laparoscopically or via minilaparotomy (large bowel size negates some laparoscopic benefit)
- In very unfit patients: percutaneous endoscopic colostomy (colonoscope-placed drainage tube through abdominal wall into sigmoid to fix bowel in untwisted position)
Emergency surgery (when ischaemia/necrosis present):
- Ligate mesenteric vessels before untwisting to theoretically prevent systemic release of ischaemic toxins
- Avoid anastomosis in contaminated/ischaemic field
- Hartmann's procedure or Paul-Mikulicz double-barrelled stoma preferred
Caecal Volvulus
- Patient profile: typically younger and otherwise well (vs. elderly in sigmoid)
- Predisposing factors: hypermobile caecum, adhesions, pelvic masses, pregnancy, gastric banding
- Endoscopic decompression is often unsuccessful and merely delays treatment
- Treatment: Urgent right hemicolectomy is indicated
Volvulus Neonatorum (Midgut Volvulus)
- Secondary to intestinal malrotation
- Potentially catastrophic - life-threatening emergency
- The midgut twists around the superior mesenteric artery
- Requires immediate surgical detorsion (Ladd's procedure)
Compound Volvulus (Ileosigmoid Knotting)
- Rare
- The long pelvic mesocolon allows the ileum to twist around the sigmoid colon
- Results in gangrene of one or both segments
- Presents with acute intestinal obstruction but comparatively mild distension
- Radiograph: distended ileal loops within a distended sigmoid
- Treatment: operative decompression, resection, and anastomosis
Volvulus - Summary Box
| Feature | Sigmoid Volvulus | Caecal Volvulus | Midgut Volvulus (Neonatal) |
|---|---|---|---|
| Age group | Elderly / African adults | Younger adults | Neonates |
| Anatomy | Long mesocolon, narrow base | Hypermobile caecum | Malrotation |
| Key symptom | Massive distension (pain = ischaemia) | Pain + distension | Bilious vomiting, shock |
| First-line Rx | Endoscopic derotation + flatus tube | Surgery | Emergency Ladd's procedure |
| Definitive Rx | Sigmoid colectomy | Right hemicolectomy | Ladd's procedure |
| Emergency Rx (ischaemia) | Hartmann's / Paul-Mikulicz stoma | Right hemicolectomy | Bowel resection if infarcted |
Key Radiology Pearls
| Sign | Condition | Modality |
|---|---|---|
| Target sign / pseudo-kidney sign | Intussusception | USS |
| Bird's beak | Volvulus (sigmoid/caecal) | Contrast enema |
| Whirl sign | Volvulus | CT |
| Coffee bean sign | Sigmoid volvulus | AXR |
| X-marks-the-spot (two overlapping transition points) | Caecal volvulus | CT |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Fischer's Mastery of Surgery 8th Ed. | Grainger & Allison's Diagnostic Radiology | ROSEN's Emergency Medicine | Sleisenger & Fordtran's GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.