dysfunctional uterine bleeding
Reading File
Finding Sources
Searching PubMed
"dysfunctional uterine bleeding" OR "abnormal uterine bleeding"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Dysfunctional Uterine Bleeding (DUB)
Definition and Modern Terminology
Dysfunctional uterine bleeding (DUB) refers to uterine bleeding that lacks an underlying structural abnormality - it is a diagnosis of exclusion. The bleeding stems primarily from hormonal disturbances rather than from organic pathology such as polyps, fibroids, endometritis, or neoplasms.
Note on current nomenclature: The term "dysfunctional uterine bleeding" has been largely replaced in modern gynecology by the broader term Abnormal Uterine Bleeding (AUB), with the FIGO classification system using the PALM-COEIN acronym to categorize causes (see below). However, DUB remains in widespread clinical and pathology use, particularly in reference to anovulatory and ovulatory hormonal causes without structural lesions.
- Tintinalli's Emergency Medicine, p. 649
Pathophysiology
Normal menstruation requires the finely-timed, cyclical interplay of the hypothalamic-pituitary-ovarian (HPO) axis. Any disruption produces DUB. There are two main mechanisms:
1. Anovulatory DUB (Most Common)
The most frequent cause of DUB is failure to ovulate. Without ovulation:
- No corpus luteum forms
- Progesterone is absent
- Estrogen stimulates the endometrium unopposed, causing continuous proliferation
- The endometrium becomes thickened and eventually sheds irregularly, producing unpredictable, often heavy bleeding
- Bleeding tends to occur at less frequent intervals than organic causes
This is most common at two extremes:
- Menarche: Immaturity of the HPO axis
- Perimenopause: Incipient ovarian failure
Robbins & Kumar Basic Pathology, p. 595; Goldman-Cecil Medicine, p. 2555
2. Ovulatory DUB (Luteal Phase Defect)
Less common. Results from an inadequate luteal phase - insufficient progesterone production by the corpus luteum - leading to early endometrial breakdown.
Causes of Anovulation
| Category | Examples |
|---|---|
| Physiological | Perimenarchal, perimenopausal fluctuations in HPO axis |
| Endocrine disorders | Thyroid disease (hypo/hyperthyroidism), adrenal disease, Cushing syndrome, pituitary prolactinoma (elevates prolactin, suppresses GnRH → reduced LH/FSH) |
| Ovarian lesions | Polycystic ovary syndrome (PCOS), granulosa cell tumors |
| Metabolic disturbances | Obesity, malnutrition, chronic systemic diseases, eating disorders, excessive exercise |
| Other | Liver disease (impairs estrogen metabolism), renal disease, stress |
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 927; Tintinalli's, p. 651
Causes of AUB by Age Group (PALM-COEIN Framework)
The modern PALM-COEIN classification distinguishes:
- Structural (PALM): Polyp, Adenomyosis, Leiomyoma, Malignancy/hyperplasia
- Non-structural (COEIN): Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not otherwise classified
| Age Group | Common Causes |
|---|---|
| Prepuberty | Precocious puberty (hypothalamic, pituitary, or ovarian origin) |
| Adolescence | Anovulatory cycle, coagulation disorders (von Willebrand disease most common - up to 20% of heavy bleeders) |
| Reproductive age | Pregnancy complications (ectopic, miscarriage), leiomyomas, adenomyosis, polyps, endometrial hyperplasia, anovulatory/ovulatory DUB, oral contraceptive use |
| Perimenopausal | Anovulatory DUB, anatomic lesions (carcinoma, hyperplasia, polyps) |
| Postmenopausal | Endometrial atrophy (most common), anatomic lesions (carcinoma, hyperplasia, polyps) |
Robbins & Kumar Basic Pathology (Table 17.2); Goldman-Cecil Medicine, p. 2555
Histopathology
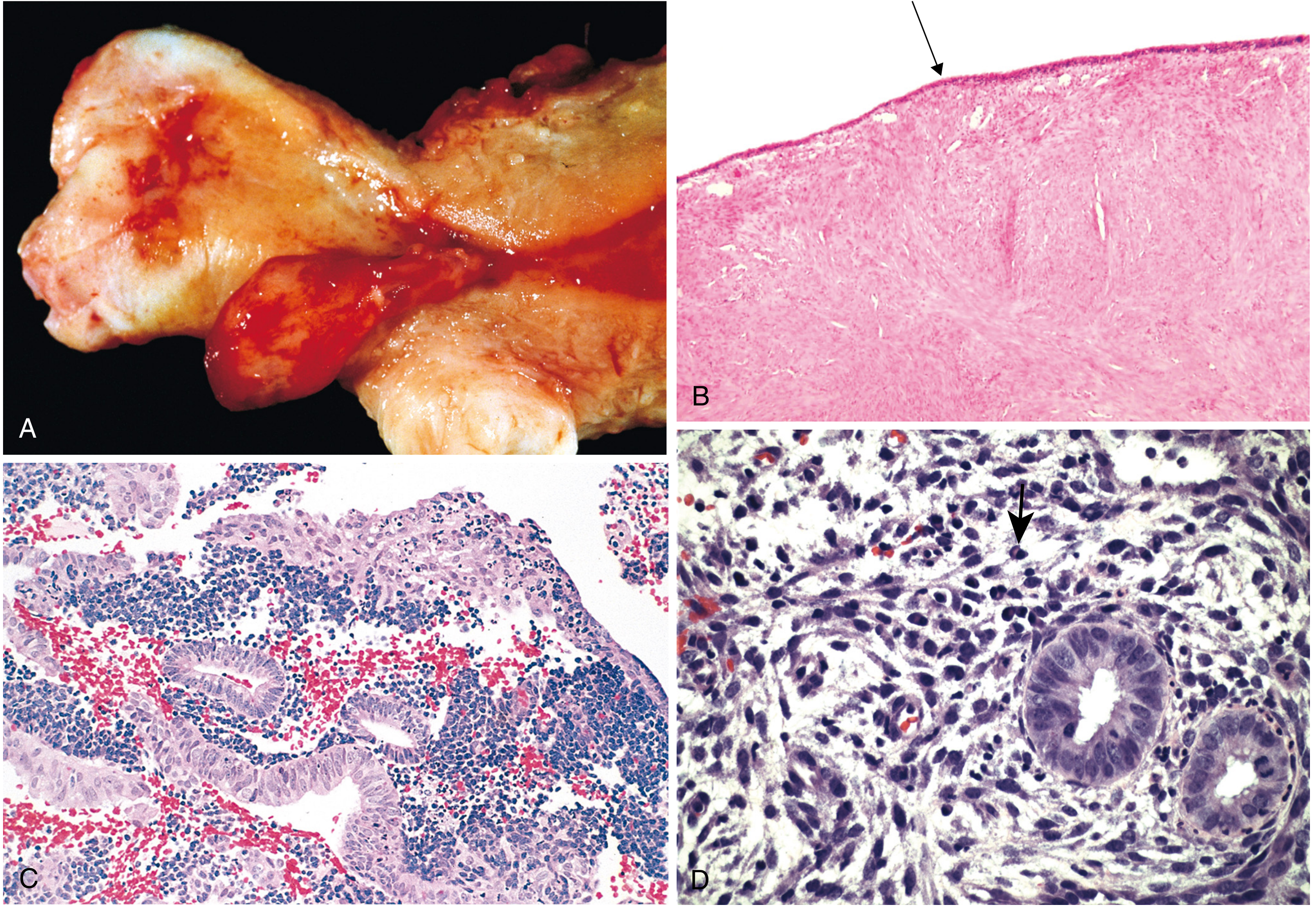
Fig. 22.20 - Robbins, Cotran & Kumar: Common causes of abnormal uterine bleeding. (C) shows the hallmark of anovulatory DUB - proliferative endometrial glands with stromal breakdown in the absence of secretory transformation.
In anovulatory DUB, the endometrium shows:
- Proliferative phase glands (no secretory transformation because progesterone is absent)
- Stromal breakdown and areas of irregular shedding
- No predecidual change
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 927
Clinical Features
- Normal menstrual blood loss: ≤30 mL per cycle; >80 mL is abnormal
- Normal cycle: 4.5-8 days duration, 24-38 day interval
- DUB is typically painless, in contrast to dysmenorrhea associated with endometriosis or fibroids
- Anovulatory DUB: irregular, unpredictable, often heavy; prolonged amenorrhea followed by heavy bleeding
- Signs of anemia in severe/chronic cases
- Hirsutism, obesity, galactorrhea may point toward endocrinologic causes (PCOS, hyperprolactinemia)
Tintinalli's Emergency Medicine, p. 649; Goldman-Cecil Medicine, p. 2555
Diagnosis (Exclusion-Based)
DUB is a diagnosis of exclusion. Always rule out:
Step 1 - History: Bleeding pattern (duration, frequency, amount), family history of bleeding disorders, medications (OCP, anticoagulants, SSRIs, tamoxifen, herbal supplements like ginseng), sexual history
Step 2 - Exclude pregnancy (urine/serum hCG - mandatory)
Step 3 - Physical examination: Hemodynamic stability, pelvic exam, speculum exam to exclude cervical/vaginal causes
Step 4 - Laboratory tests:
- Complete blood count, platelets
- Coagulation studies (including von Willebrand disease screen: heavy menses since menarche, postpartum hemorrhage, surgery/dental bleeding, bruising)
- Thyroid function tests (TSH)
- Fasting glucose
- Serum prolactin if suspected
Step 5 - Endometrial sampling (biopsy or D&C):
- All women >35 years with abnormal bleeding
- Any patient with risk factors for endometrial carcinoma (prolonged anovulatory bleeding, obesity, diabetes, unopposed estrogen)
Step 6 - Imaging: Transvaginal ultrasound or sonohysterography to exclude polyps, fibroids, and structural lesions
Goldman-Cecil Medicine, p. 2556; Tintinalli's, p. 649
Treatment
Management depends on acuity, age, and desire for fertility.
A. Acute / Massive Bleeding (ED Setting)
| Agent | Dose | Notes |
|---|---|---|
| Conjugated equine estrogen (IV) | 25 mg IV every 4-6 hours (up to 3 doses) | Stops bleeding within hours; give antiemetics; contraindicated if VTE, thrombophilia, vascular disease, or malignancy |
| Combined OCP | 1 pill every 6 hours x 5-7 days (off-label) | Bleeding should cease within 24 hours; warn patient of withdrawal bleed 2-4 days after stopping |
| Tranexamic acid | As per local protocol | Antifibrinolytic; useful in ovulatory heavy bleeding |
| Blood transfusion | If anemia is profound | |
| Curettage (D&C) | If bleeding continues despite hormonal therapy | Diagnostic and temporarily therapeutic |
Goldman-Cecil Medicine, p. 2556; Tintinalli's, p. 651
B. Chronic / Non-Acute Management
Medical (first-line):
- Combined oral contraceptives (cyclic): If pregnancy not desired - regulates cycle, reduces blood loss
- Progestin therapy: Medroxyprogesterone acetate 5-10 mg orally for 10 days/month; or norethindrone 5 mg daily
- Levonorgestrel-IUD (Mirena): Highly effective for ovulatory AUB and heavy menstrual bleeding
- NSAIDs: Effective for ovulatory heavy bleeding (reduce prostaglandin-mediated blood loss)
- GnRH agonists/antagonists (e.g., elagolix 300 mg BD, relugolix 40 mg/day): For uterine fibroids causing AUB
If pregnancy desired:
- Induce ovulation (clomiphene citrate or gonadotropins)
Surgical (second-line / when medical therapy fails):
- Endometrial ablation: Effective but not 100%; ~29% of patients may require hysterectomy by 5 years
- Uterine artery embolization: For fibroid-related bleeding; ~31% ultimately require hysterectomy
- Hysterectomy: Reserved for refractory cases or malignancy; definitive treatment
Berek & Novak's Gynecology, p. 1411; Goldman-Cecil Medicine, p. 2556; Sabiston Textbook of Surgery, p. 1411
Key Risk: Endometrial Hyperplasia and Carcinoma
Prolonged anovulatory bleeding results in unopposed estrogen stimulation of the endometrium. This can progress:
Anovulatory DUB → Endometrial Hyperplasia → Endometrial Carcinoma
Risk factors that increase this progression:
- Obesity (adipose tissue converts androgens to estrogens)
- PCOS
- Prolonged use of exogenous estrogens without progesterone
- Estrogen-producing ovarian tumors (granulosa-theca cell tumors)
This is why endometrial sampling is mandatory in women >35 years or with prolonged anovulatory bleeding before initiating hormonal treatment.
Robbins & Kumar Basic Pathology, p. 611
Summary Table
| Feature | Anovulatory DUB | Ovulatory DUB |
|---|---|---|
| Mechanism | No ovulation → no progesterone | Luteal phase defect |
| Pattern | Irregular, unpredictable, heavy | Regular intervals, but heavy |
| BBT chart | Monophasic | Biphasic but shortened luteal phase |
| Endometrium | Proliferative glands, stromal breakdown | May show secretory changes |
| Age group | Perimenarche, perimenopause, PCOS | Reproductive age |
| Malignancy risk | Elevated (unopposed estrogen) | Low |
Recent evidence note: A 2025 systematic review (PMID 39617186) on etiology and diagnosis of heavy menstrual bleeding in adolescents and adults highlights that coagulation disorders (particularly von Willebrand disease) are substantially underdiagnosed as a cause - reinforcing the importance of screening all patients with heavy bleeding since menarche, especially adolescents.
This is a shared conversation. Sign in to Orris to start your own chat.