Anterolateral system of ascending pathways use Guyton and Hall and ganong as your reference
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both textbooks and the key diagrams. Let me compose the full, well-structured answer.
Anterolateral System of Ascending Pathways
Overview
The anterolateral system (also called the ventrolateral spinothalamic pathway) is one of the two major ascending somatosensory systems. It is fundamentally different from the dorsal column-medial lemniscal system in the type of information it carries and the precision with which it does so.
Guyton & Hall defines the sensations carried by the anterolateral system as:
- Pain
- Thermal sensations (both warm and cold)
- Crude touch and pressure - capable only of crude localizing ability on the body surface
- Tickle and itch sensations
- Sexual sensations
Ganong frames it this way: the ventrolateral spinothalamic pathway mediates pain and temperature, while the dorsal column (medial lemniscal) pathway handles touch, vibratory sense, and proprioception.
Anatomy of the Anterolateral Pathway
(Guyton & Hall, Ch. 48)
First-order neurons (peripheral afferents):
- Signals from nociceptors, thermoreceptors, and crude mechanoreceptors travel via small, thinly myelinated (Aδ) and unmyelinated (C) fibers to the spinal cord through the dorsal roots.
Dorsal horn origin:
- The anterolateral pathway fibers originate mainly from dorsal horn laminae I, IV, V, and VI - the zones where the relevant dorsal root sensory fibers terminate after entering the cord.
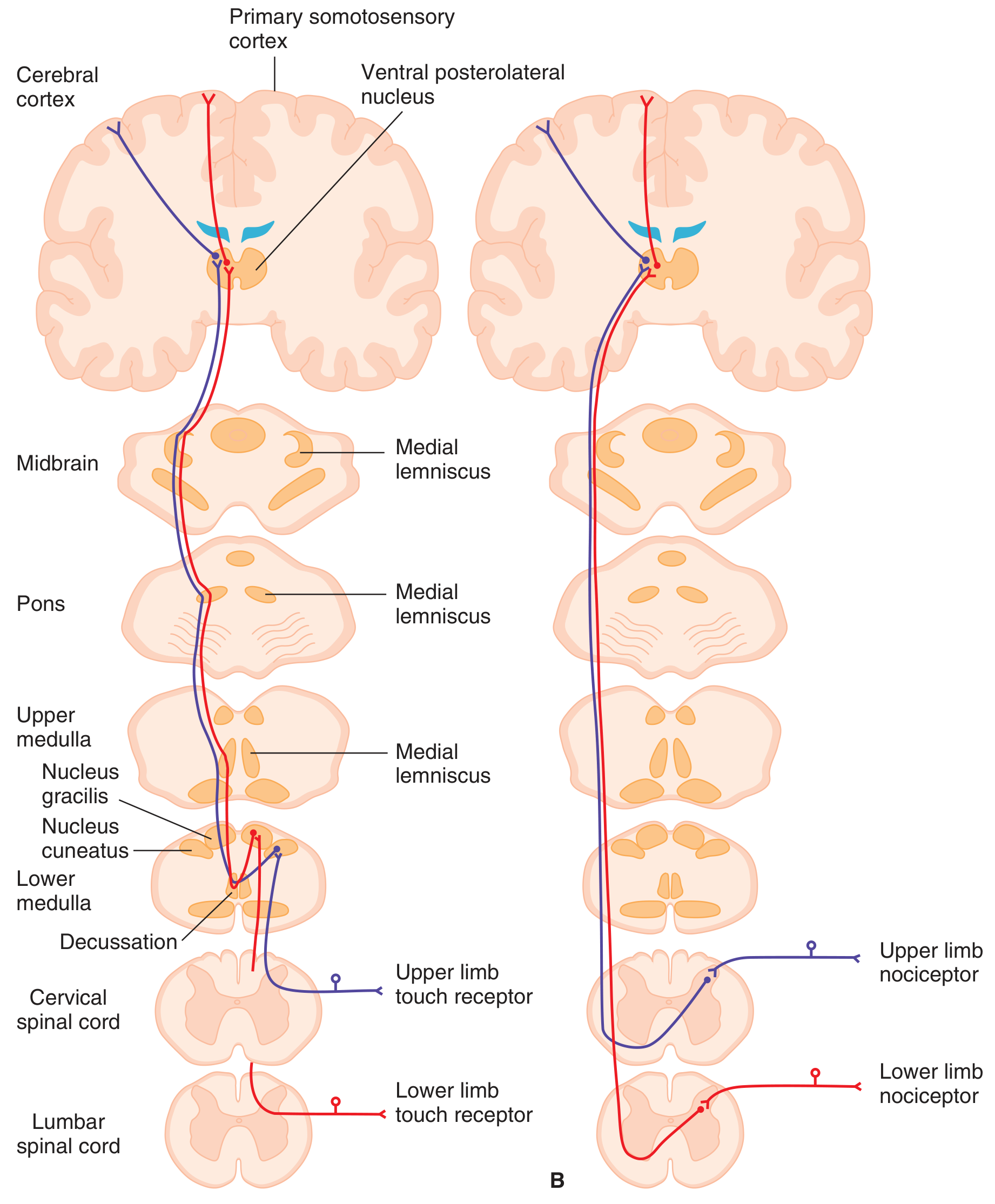
Decussation:
- The axons of second-order neurons cross immediately in the anterior commissure of the spinal cord to the opposite (contralateral) anterior and lateral white columns.
- This is a key contrast with the dorsal column system, which ascends ipsilaterally and crosses only at the medulla.
Ascent:
- After crossing, fibers ascend as two named tracts:
- Lateral spinothalamic tract - primarily carries pain and temperature
- Anterior spinothalamic tract - primarily carries crude touch and pressure
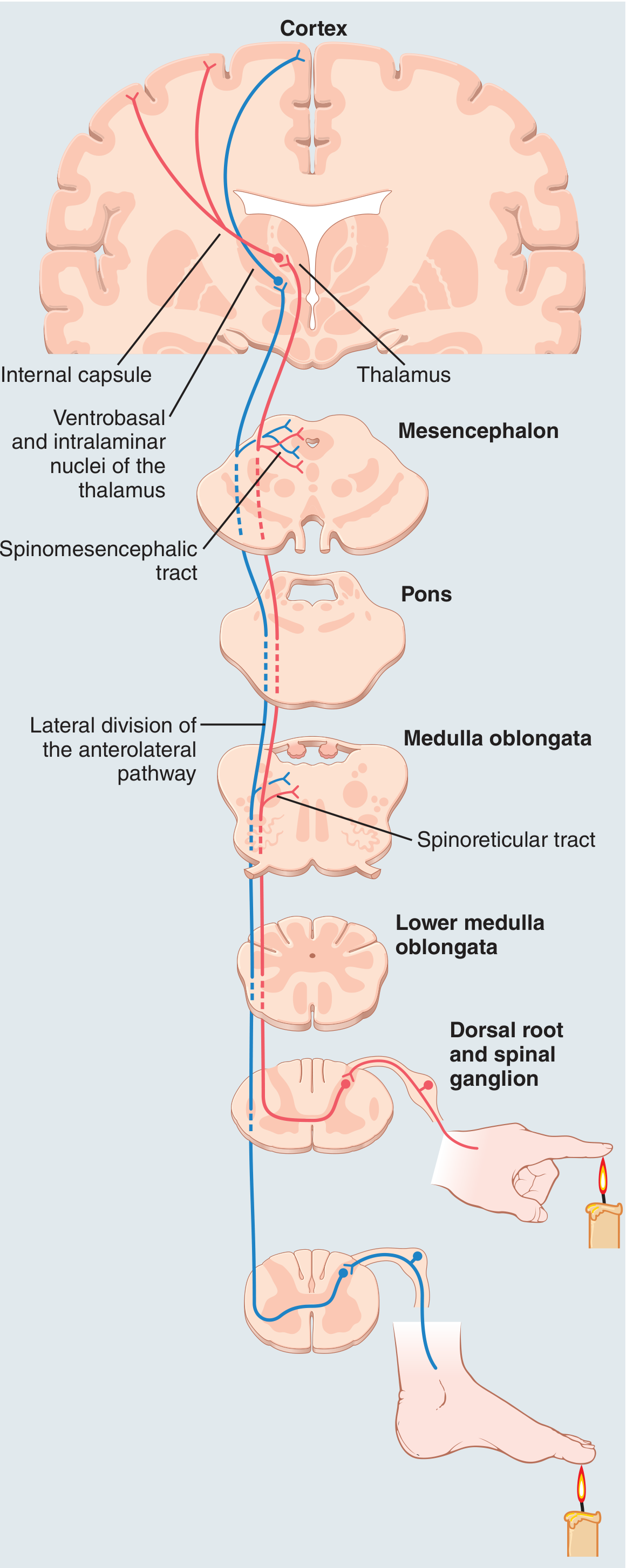
Thalamic termination:
The upper terminus of the spinothalamic tracts is two-fold:
- Reticular nuclei of the brainstem - especially relevant for pain signals
- Two thalamic complexes:
- Ventrobasal complex (VPL nucleus) - receives mainly tactile signals from the anterolateral path and relays them to the somatosensory cortex (same target as dorsal column signals)
- Intralaminar nuclei - receives most pain signals (relayed from brainstem reticular nuclei)
Ganong adds: some dorsal horn neurons receiving nociceptive input project via the spinoreticular pathway to the centrolateral nucleus of the thalamus.
Cortical Projections and Functional Components
(Ganong, Ch. 8)
PET and fMRI studies show that pain activates:
- Primary somatosensory cortex (S1) and secondary somatosensory cortex (S2) - contralateral side
- Cingulate gyrus - contralateral
- Amygdala, frontal lobe, insular cortex
This gives rise to two functional components of pain:
| Component | Pathway | Function |
|---|---|---|
| Discriminative | VPL thalamus → primary somatosensory cortex | Pain localization |
| Motivational-affective | Brainstem reticular formation → centrolateral thalamus → frontal lobe + limbic system + insular cortex | Emotional/aversive quality of pain |
Visceral sensation travels through the same spinothalamic tracts and thalamic radiations as somatic sensation, with cortical receiving areas intermixed with somatic areas.
Characteristics of Transmission (Guyton & Hall, Ch. 48)
The anterolateral system is a cruder transmission system compared to the dorsal column-medial lemniscal system. Key differences:
| Feature | Anterolateral System | Dorsal Column System |
|---|---|---|
| Conduction velocity | 8-40 m/sec (1/3 to 1/2 of DC system) | ~70-80 m/sec |
| Spatial localization | Poor | Precise |
| Intensity gradation | ~10-20 gradations | Up to 100 gradations |
| Rapidly changing signals | Poorly transmitted | Well transmitted |
| Decussation level | Spinal cord (each segment) | Lower medulla |
Even with these limitations, the anterolateral system is the exclusive pathway for pain, temperature, tickle, itch, and sexual sensations. These modalities are not transmitted by the dorsal column-medial lemniscal system at all.
Somatotopic Organization
(Ganong, Ch. 8)
Within the ventrolateral spinothalamic tract, fibers are somatotopically arranged:
- Sacral fibers are positioned most laterally
- Cervical fibers are positioned most medially
(Note: this is the opposite arrangement from the dorsal columns, where sacral fibers are most medial.)
This organization is clinically relevant - a central cord lesion may spare sacral pain/temperature fibers (sacral sparing), while an anterolateral cordotomy for pain relief selectively interrupts pain and temperature from contralateral structures below the level of cut.
Effects of Lesions
(Ganong, Ch. 8)
- Damage to the ventrolateral spinothalamic pathway → contralateral loss of pain and temperature sensation below the level of the lesion.
- Dorsal column damage → ipsilateral loss of touch, vibration, and proprioception below the lesion.
This dissociation is the anatomical basis of Brown-Séquard syndrome (spinal hemisection): ipsilateral motor paralysis + ipsilateral loss of discriminative touch/vibration + contralateral loss of pain/temperature starting 1-2 segments below the lesion.
- Thalamic lesions → can cause thalamic pain syndrome (Déjerine-Roussy) during recovery - characterized by chronic burning pain contralateral to the side of the infarct.
- Primary somatosensory cortex damage → does not abolish somatic sensation but impairs ability to localize noxious stimuli in time, space, and intensity; irritation causes contralateral paresthesia.
- Cingulate cortex damage → impairs recognition of the aversive nature of a noxious stimulus.
Summary Comparison: Anterolateral vs. Dorsal Column Systems
| Feature | Anterolateral System | Dorsal Column-ML System |
|---|---|---|
| Modalities | Pain, temperature, crude touch, tickle, itch, sexual sensation | Discriminative touch, vibration, proprioception |
| Fiber type | Aδ and C (small, slow) | Aβ (large, fast) |
| 1st synapse | Dorsal horn (laminae I, IV, V, VI) | Dorsal column nuclei (gracilis/cuneatus) in medulla |
| Decussation | At each cord segment (anterior commissure) | Lower medulla (sensory decussation) |
| Thalamic relay | VPL + intralaminar nuclei | VPL (ventrobasal complex) |
| Cortical target | S1, S2, cingulate, insular, frontal (limbic) | S1 (postcentral gyrus) primarily |
| Localization | Poor | Precise |
| Conduction velocity | 8-40 m/sec | ~70+ m/sec |
References:
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Ch. 48 (Sensory Transmission; Anterolateral System)
- Ganong's Review of Medical Physiology, 26th Ed., Ch. 8 (Somatosensory Pathways; Ventrolateral Spinothalamic Tract; Effects of CNS Lesions)
Explain the pain modulation pathways (descending controls and gate control theory)
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed from both Guyton & Hall and Ganong. Here is the complete, well-structured answer.
Pain Modulation Pathways: Descending Controls and Gate Control Theory
1. Gate Control Theory (Spinal Level)
The Basic Concept
(Ganong, Ch. 8)
The gate control theory, originally proposed by Melzack and Wall (1965), explains how non-painful sensory input can suppress pain at the level of the spinal cord. The key observation is simple and familiar: rubbing or shaking an injured area reduces pain. The mechanism is as follows:
- Activation of large-diameter, low-threshold mechanoreceptor afferents (Aα and Aβ fibers) - which carry innocuous touch and vibration - sends collaterals into the dorsal horn.
- The activity of these large-fiber afferents reduces the responsiveness of dorsal horn neurons to input from nociceptive afferents (Aδ and C fibers).
- The large fibers in effect "close the gate" on pain transmission before it can ascend.
This mechanism is the scientific rationale behind Transcutaneous Electrical Nerve Stimulation (TENS), which uses surface electrodes to selectively activate Aα and Aβ fibers near the site of injury to produce analgesia.
Cellular Mechanism in the Dorsal Horn
(Ganong, Ch. 8)
At the cellular level, the dorsal horn acts as the gate. Interneurons in the superficial laminae contain enkephalin and dynorphin (endogenous opioid peptides). These opioidergic interneurons are strategically placed where nociceptive afferents terminate and can modulate transmission in two ways:
Presynaptic inhibition:
- Opioid receptors on the terminals of nociceptive fibers (and in the dorsal root ganglia)
- Opioid binding → decreased Ca²⁺ influx → reduced duration of action potential → decreased transmitter (glutamate + neuropeptides) release from the nociceptive terminal
Postsynaptic inhibition:
- Opioid receptors on dendrites of dorsal horn projection neurons
- Opioid binding → increased K⁺ conductance → hyperpolarization of the dorsal horn neuron → decreased response to excitatory synaptic input
- Also reduces amplitude of the EPSP produced by nociceptor stimulation
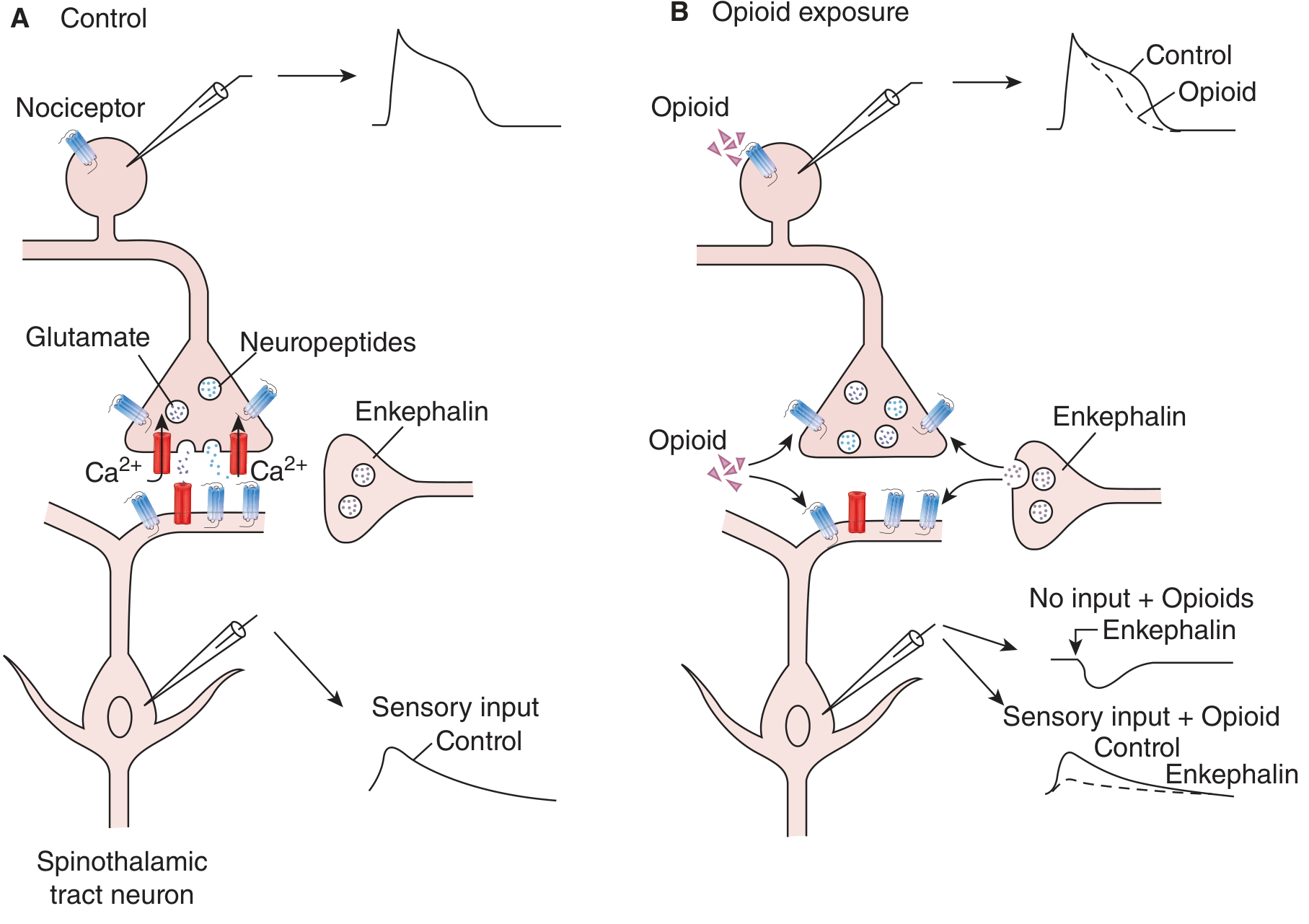
Panel A shows normal nociceptive transmission (Ca²⁺ influx → glutamate/neuropeptide release → spinothalamic tract activation). Panel B shows how opioids block this at both presynaptic (DRG) and postsynaptic (dorsal horn) levels.
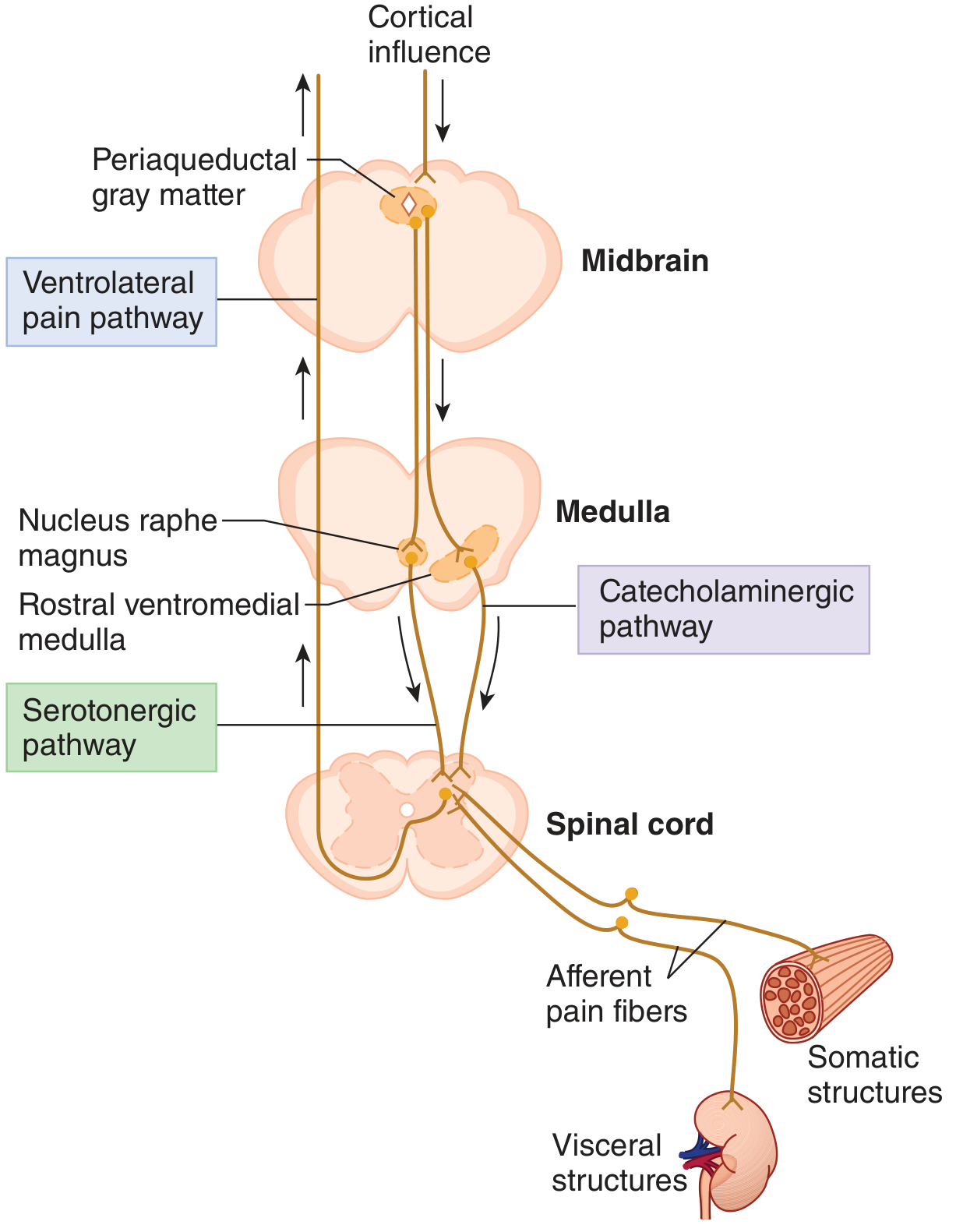
2. Descending Pain Modulation (Supraspinal Control)
The Three-Component Analgesia System
(Guyton & Hall, Ch. 49)
The brain possesses an intrinsic pain suppression (analgesia) system. The degree to which different people react to pain varies tremendously, partly because the brain can actively suppress incoming pain signals. This system has three major components arranged in a descending hierarchy:
Component 1 - Supraspinal origin:
- Periaqueductal gray (PAG) matter surrounding the aqueduct of Sylvius in the mesencephalon and upper pons
- Periventricular nuclei of the hypothalamus, adjacent to the third ventricle
- Medial forebrain bundle (hypothalamus)
- These areas receive higher cortical influences and are the starting point of the descending cascade
Component 2 - Brainstem relay:
- PAG and periventricular neurons send signals to:
- Raphe magnus nucleus - a thin midline nucleus in the lower pons/upper medulla (serotonergic)
- Nucleus reticularis paragigantocellularis - located laterally in the medulla (catecholaminergic)
- Electrical stimulation of the PAG or raphe magnus nucleus can suppress many strong pain signals entering via dorsal spinal roots
Component 3 - Spinal cord output:
- Second-order signals descend via the dorsolateral columns of the spinal cord
- They reach a pain inhibitory complex in the dorsal horns
- Here, analgesia signals block pain before it is relayed to the brain
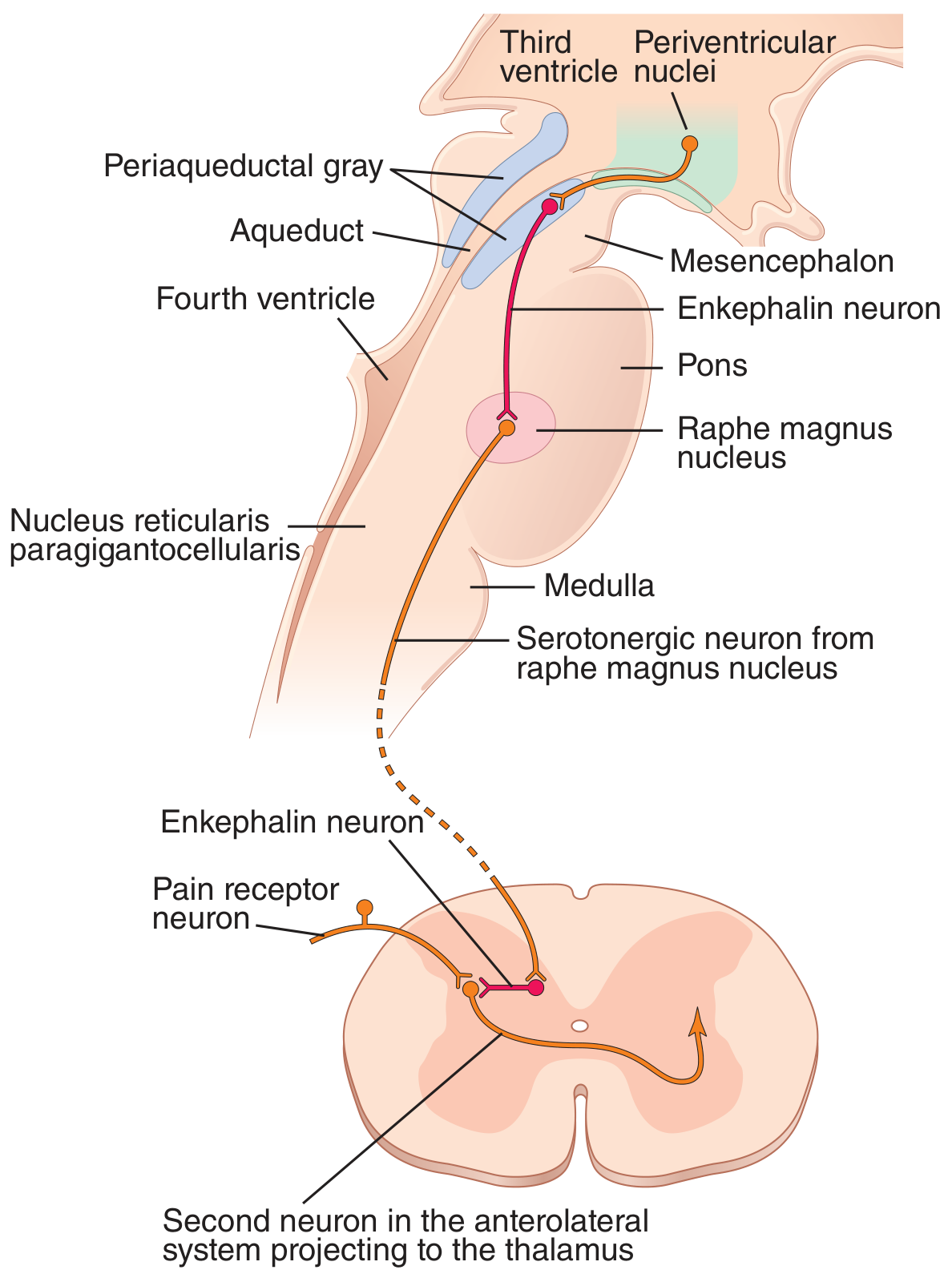
Shows: Periventricular nuclei and PAG → enkephalin fibers → raphe magnus → serotonergic descending fibers → dorsal horn enkephalin interneurons → presynaptic/postsynaptic inhibition of C and Aδ pain fibers.
Neurotransmitters in the Descending System
(Guyton & Hall Ch. 49; Ganong Ch. 8)
| Level | Transmitter | Source | Action |
|---|---|---|---|
| PAG/periventricular → raphe magnus | Enkephalin | Periventricular and PAG neurons | Released at raphe magnus nucleus endings |
| Raphe magnus → dorsal horn | Serotonin | Raphe magnus serotonergic neurons | Descends via dorsolateral columns; activates dorsal horn enkephalin interneurons |
| Dorsal horn interneurons | Enkephalin | Local interneurons (triggered by serotonin from raphe) | Pre- and postsynaptic inhibition of Aδ and C fiber input |
| Locus coeruleus → dorsal horn | Norepinephrine | Pontine catecholaminergic neurons | Released in dorsal horn; analgesic effect |
| Rostral ventromedial medulla → dorsal horn | Norepinephrine | Catecholaminergic neurons | Inhibit dorsal horn nociceptive neurons |
Ganong summarizes the pathway: PAG → nucleus raphe magnus (serotonergic) + rostral ventromedial medulla (catecholaminergic) → dorsal horn enkephalin interneurons → inhibition of nociceptive transmission.
The Brain's Opiate System - Endorphins and Enkephalins
(Guyton & Hall, Ch. 49)
About a dozen endogenous opioid-like substances have been identified - all are breakdown products of three large protein precursors:
- Pro-opiomelanocortin → β-endorphin (found in hypothalamus and pituitary)
- Proenkephalin → met-enkephalin and leu-enkephalin (found in brainstem and spinal cord, within the analgesia system)
- Prodynorphin → dynorphin (same areas as enkephalins, lower quantities)
Injection of minute quantities of morphine into the PAG or periventricular nuclei produces extreme analgesia - this works because morphine mimics these endogenous ligands at their receptors. Opioid receptors are distributed throughout the analgesia system: dorsal horn, PAG, raphe magnus, and hypothalamus.
3. Inhibition by Tactile Signals (Peripheral Gate)
(Guyton & Hall, Ch. 49)
Stimulation of large-type Aβ sensory fibers from peripheral tactile receptors can depress transmission of pain signals from the same body area, through local lateral inhibition in the spinal cord. This explains:
- Why rubbing skin near a painful area brings relief
- Why liniments work for pain relief
- The mechanism behind acupuncture - both psychogenic excitation of the central analgesia system and activation of Aβ fibers contribute
- The basis of TENS (transcutaneous electrical nerve stimulation)
4. Stress-Induced Analgesia
(Ganong, Ch. 8)
Soldiers wounded in battle often feel no pain until the battle is over - a classic example of stress-induced analgesia. Mechanisms include:
- Release of norepinephrine (from brainstem catecholaminergic neurons) in the amygdala - which mediates the motivational-affective responses to pain
- Release of endogenous cannabinoids (2-arachidonylglycerol/2AG and anandamide), acting on CB1 receptors (euphoria, analgesia) and CB2 receptors (expressed on activated microglia in neuropathic pain states, reducing inflammatory response)
5. Clinical Correlates and Applications
| Clinical Application | Mechanism |
|---|---|
| TENS | Activates Aα/Aβ fibers → closes gate at dorsal horn |
| Acupuncture | Activates ascending sensory pathways → PAG and brainstem serotonergic/catecholaminergic nuclei → endogenous opioid release (blocked by naloxone) |
| Morphine/opioids | Mimic endogenous enkephalins at dorsal horn, PAG, and DRG receptors |
| Spinal cord stimulation | Electrodes stimulate dorsal sensory columns → activate gate control and possibly descending inhibition |
| Thalamic/PAG stimulation | Deep brain stimulation electrodes in intralaminar nuclei or periventricular area → patient-controlled dramatic pain relief |
| Antidepressants (SNRIs/TCAs) for chronic pain | Enhance descending serotonergic and noradrenergic inhibitory pathways |
Summary Diagram of the Full System
Cortex / Limbic system
↓
Periventricular nuclei (hypothalamus)
↓ [enkephalin]
Periaqueductal Gray (PAG) - midbrain
↓
Nucleus Raphe Magnus (pons/medulla) Locus Coeruleus (pons)
[serotonergic] [noradrenergic]
↓ dorsolateral columns ↓
Dorsal Horn (spinal cord)
↑ [large Aβ fiber input - gate control]
Enkephalin interneurons
→ Presynaptic inhibition of C/Aδ terminals (↓ Ca²⁺ → ↓ glutamate/neuropeptide release)
→ Postsynaptic inhibition of dorsal horn neurons (↑ K⁺ → hyperpolarization)
↓ BLOCKED
Pain signal does NOT ascend spinothalamic tract
References:
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Ch. 49 (Pain Suppression/Analgesia System; Endorphins and Enkephalins; Inhibition by Tactile Signals)
- Ganong's Review of Medical Physiology, 26th Ed., Ch. 8 (Processing Information in the Dorsal Horn - Gate Control; Roles of PAG and Brainstem; Stress-Induced Analgesia)
This is a shared conversation. Sign in to Orris to start your own chat.