Auscultation of heart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of cardiac auscultation, drawn from Guyton & Hall Medical Physiology, Gray's Anatomy for Students, and the Harriet Lane Handbook.
Auscultation of the Heart
Auscultation means listening to body sounds, usually with a stethoscope. Cardiac auscultation allows detection of the normal heart sounds, extra sounds, and murmurs produced by valve abnormalities or structural defects.
1. Normal Heart Sounds
A normal heart produces two sounds per cycle, classically described as "lub-dub":
| Sound | Cause | Timing | Best Heard At |
|---|---|---|---|
| S1 ("lub") | Closure of mitral + tricuspid (AV) valves | Start of systole | Apex / left lower sternal border (LLSB) |
| S2 ("dub") | Closure of aortic + pulmonary (semilunar) valves | End of systole | Left upper sternal border (LUSB) |
| S3 | Blood oscillating in early-to-mid diastole as ventricles fill | Early-mid diastole | Apex / LLSB |
| S4 | Atrial contraction against stiff ventricle | Late diastole (pre-systole) | Apex |
S1 details: The main cause is vibration of the AV valve leaflets immediately after closure, plus vibration of adjacent ventricular walls and chordae tendineae. It is longer (~0.14 s) and lower-pitched than S2. - Guyton and Hall Textbook of Medical Physiology
S2 details: Caused by sudden closure of the semilunar valves at end-systole, with elastic recoil of blood bouncing back from the arterial walls. It is shorter (~0.11 s) and higher-pitched than S1 because the semilunar valves are tauter and the arteries are less elastic than the ventricles. - Guyton and Hall Textbook of Medical Physiology
S2 splitting: S2 has two components - aortic closure (A2) and pulmonary closure (P2). Physiologic splitting widens with inspiration (increased venous return delays pulmonary valve closure). Heard best at the LUSB.
-
Widely split S2: Ebstein anomaly, RBBB
-
Widely split and fixed S2: ASD, RV volume/pressure overload, RBBB
-
Single S2: Pulmonary hypertension, pulmonary/aortic atresia, severe AS
-
Paradoxically split S2 (splits on expiration): Severe AS, LBBB, Wolff-Parkinson-White (type B)
-
Harriet Lane Handbook
S3 ("ventricular gallop"): Occurs at the beginning of the middle third of diastole due to oscillation of blood between ventricular walls. Its frequency is often below the audible threshold (~20 cycles/sec). It may be normal in children, adolescents, and young adults, but in older adults it usually signals systolic heart failure.
S4 ("atrial gallop"): Produced by atrial contraction forcing blood into a non-compliant ventricle. Always considered pathologic - indicates decreased ventricular compliance (e.g., LV hypertrophy). - Harriet Lane Handbook
2. Auscultation Areas on the Chest
The valves are not listened to directly over their anatomical location; instead, sounds are conducted downstream along the blood flow path.
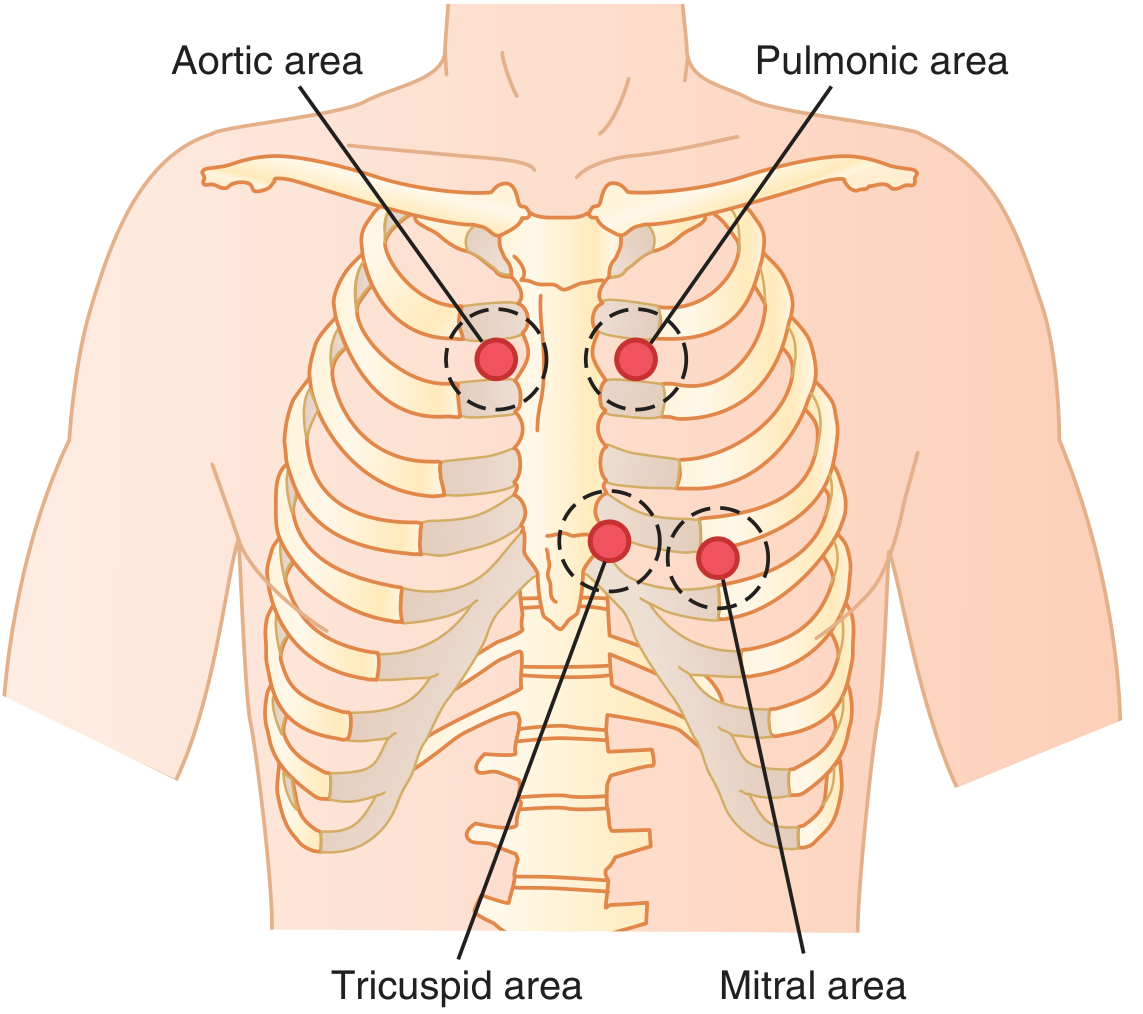
Figure: Chest areas from which sounds from each valve are best heard. - Guyton and Hall Textbook of Medical Physiology
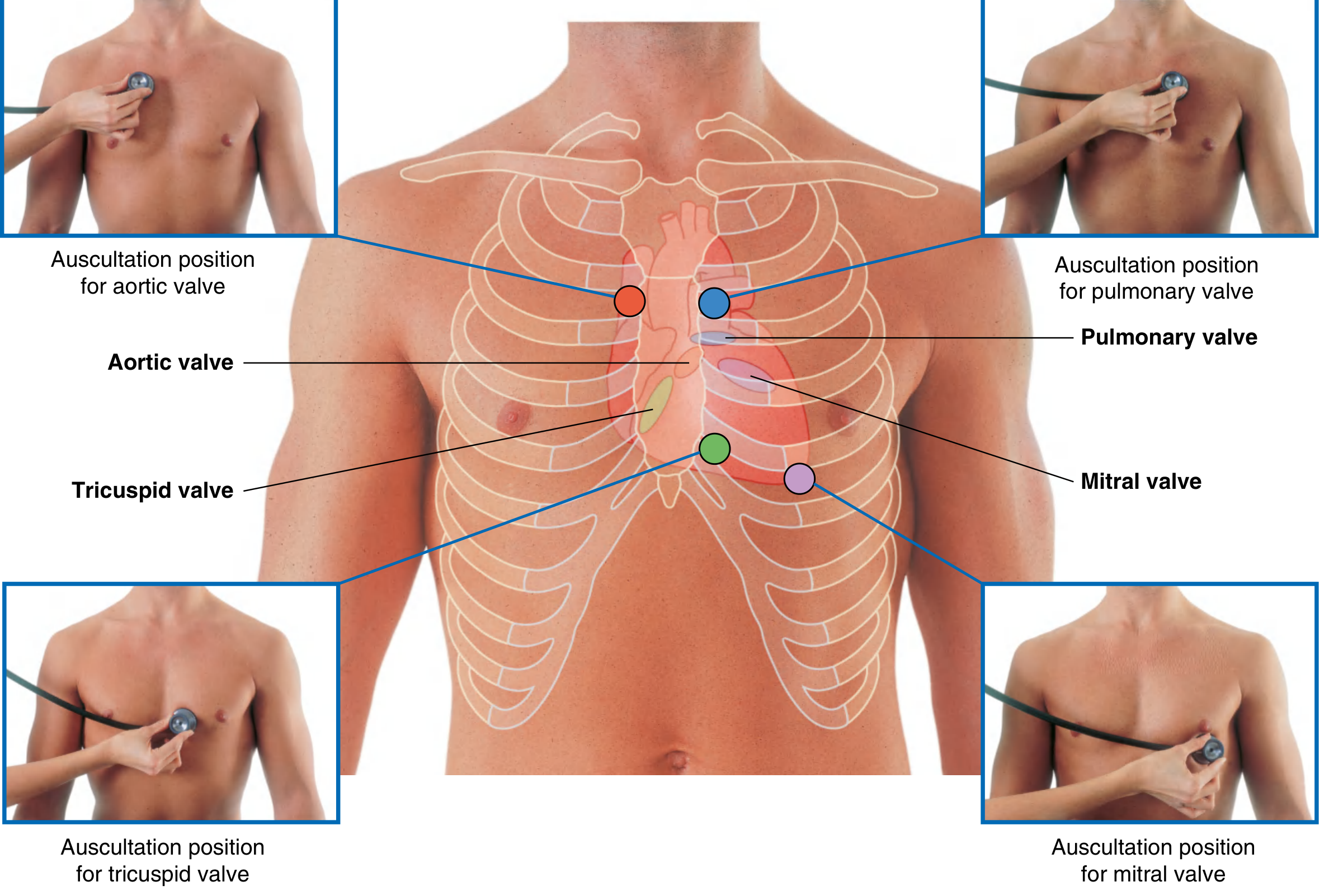
Figure: Valve locations and corresponding auscultation positions. - Gray's Anatomy for Students
| Valve | Auscultation Area |
|---|---|
| Aortic | Right 2nd intercostal space (ICS), medial end - sounds transmitted up the aorta |
| Pulmonary | Left 2nd ICS, medial end - sounds transmitted up the pulmonary artery |
| Tricuspid | Left lower sternal border, ~5th ICS - over the right ventricle |
| Mitral | Apex, left 5th ICS at the midclavicular line - over the apex of the left ventricle |
The cardiologist identifies individual valve sounds by moving the stethoscope systematically and using elimination - noting relative loudness in each area to isolate each valve's contribution. - Guyton and Hall Textbook of Medical Physiology
3. Additional Sounds
Ejection Click
- Heard with stenosis of semilunar valves, dilated great arteries, pulmonary/systemic hypertension, TOF, persistent truncus arteriosus
- Occurs early in systole
Midsystolic Click
- Heard at the apex in mitral valve prolapse (MVP)
Opening Snap
- A diastolic sound heard in mitral stenosis (or tricuspid stenosis) - rare in children
- Caused by the sudden tensing of fused mitral leaflets as they open under atrial pressure
4. Heart Murmurs
Murmurs are caused by turbulent blood flow, usually due to valve abnormalities, septal defects, or high-output states.
Grading (Levine Scale, I-VI)
| Grade | Description |
|---|---|
| I | Barely audible |
| II | Softer than heart sounds, but audible |
| III | Moderately loud; as loud as heart sounds; no thrill |
| IV | Louder than heart sounds; associated with a thrill |
| V | Audible with stethoscope barely on the chest |
| VI | Audible with stethoscope lifted off the chest |
- Harriet Lane Handbook
Phonocardiogram Patterns
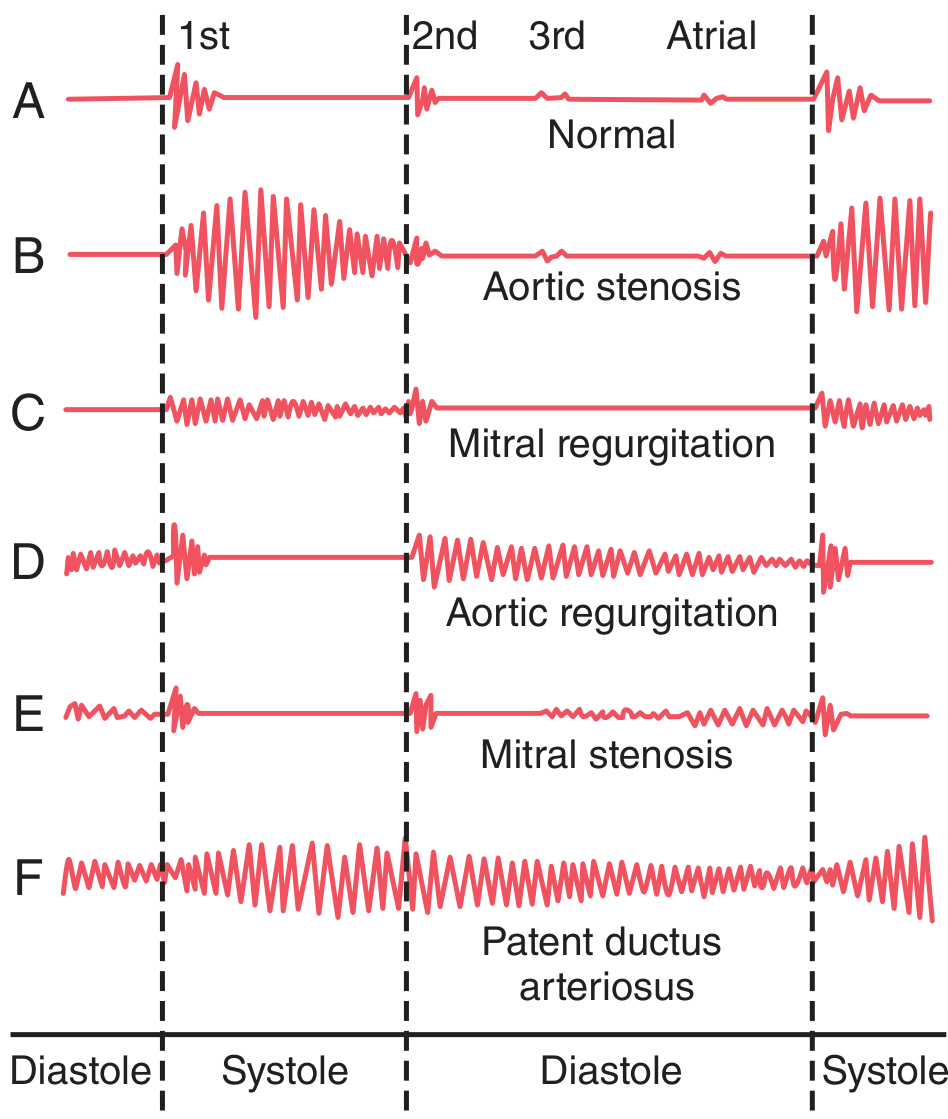
Figure: Phonocardiograms from normal and abnormal hearts - (A) Normal, (B) Aortic stenosis - systolic ejection murmur, (C) Mitral regurgitation - holosystolic murmur, (D) Aortic regurgitation - diastolic murmur, (E) Mitral stenosis - diastolic rumble, (F) PDA - continuous machinery murmur. - Guyton and Hall Textbook of Medical Physiology
Common Murmurs by Valve Lesion
| Condition | Timing | Character | Location |
|---|---|---|---|
| Aortic stenosis | Systolic (ejection) | Harsh, crescendo-decrescendo | Aortic area, radiates to neck |
| Aortic regurgitation | Diastolic (early) | High-pitched, blowing, decrescendo | Left sternal border |
| Mitral regurgitation | Holosystolic | Blowing | Apex, radiates to axilla |
| Mitral stenosis | Diastolic (mid-late) | Low-pitched rumble | Apex |
| VSD | Holosystolic | Harsh | LLSB |
| PDA | Continuous ("machinery") | Crescendo-decrescendo | Pulmonic area |
Clinical Approach to a Murmur
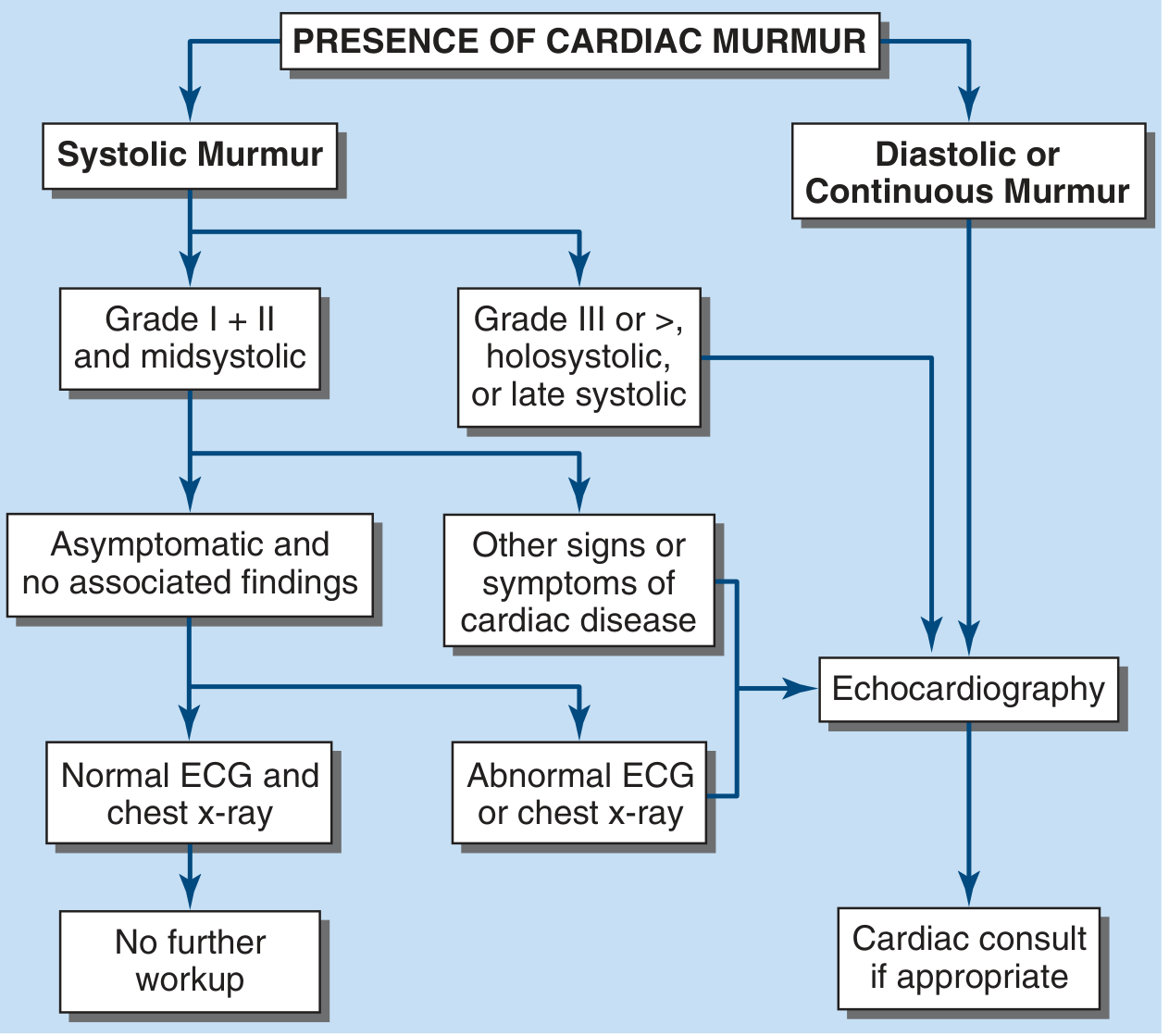
Figure: Approach to evaluation of a heart murmur. - Harrison's Principles of Internal Medicine, 22nd Ed.
Key clinical decision points:
- Grade I-II midsystolic murmur in an asymptomatic young person with no other findings → likely innocent/benign, no echocardiography needed
- Grade ≥III, holosystolic, or late systolic → echocardiography indicated
- Any diastolic or continuous murmur → always pathologic, warrants echocardiography
5. Innocent (Benign) Murmurs
Present in >80% of children at some point during childhood. Features:
-
Grade 1-3/6
-
Normal ECG and chest radiograph
-
Accentuated in high-output states (fever, anemia, anxiety, exercise)
-
Examples: Still's vibratory murmur (ages 3-6), pulmonary ejection murmur (ages 8-14)
-
Harriet Lane Handbook
Summary Mnemonic for Auscultation Areas
All Physicians Take Money:
- Aortic - Right 2nd ICS
- Pulmonary - Left 2nd ICS
- Tricuspid - Left lower sternal border
- Mitral - Apex (5th ICS, midclavicular line)
This is a shared conversation. Sign in to Orris to start your own chat.