Give a photo of one page notes of amenorrhea for my final proff university exam
amenorrhea one page notes classification causes investigation management MBBS
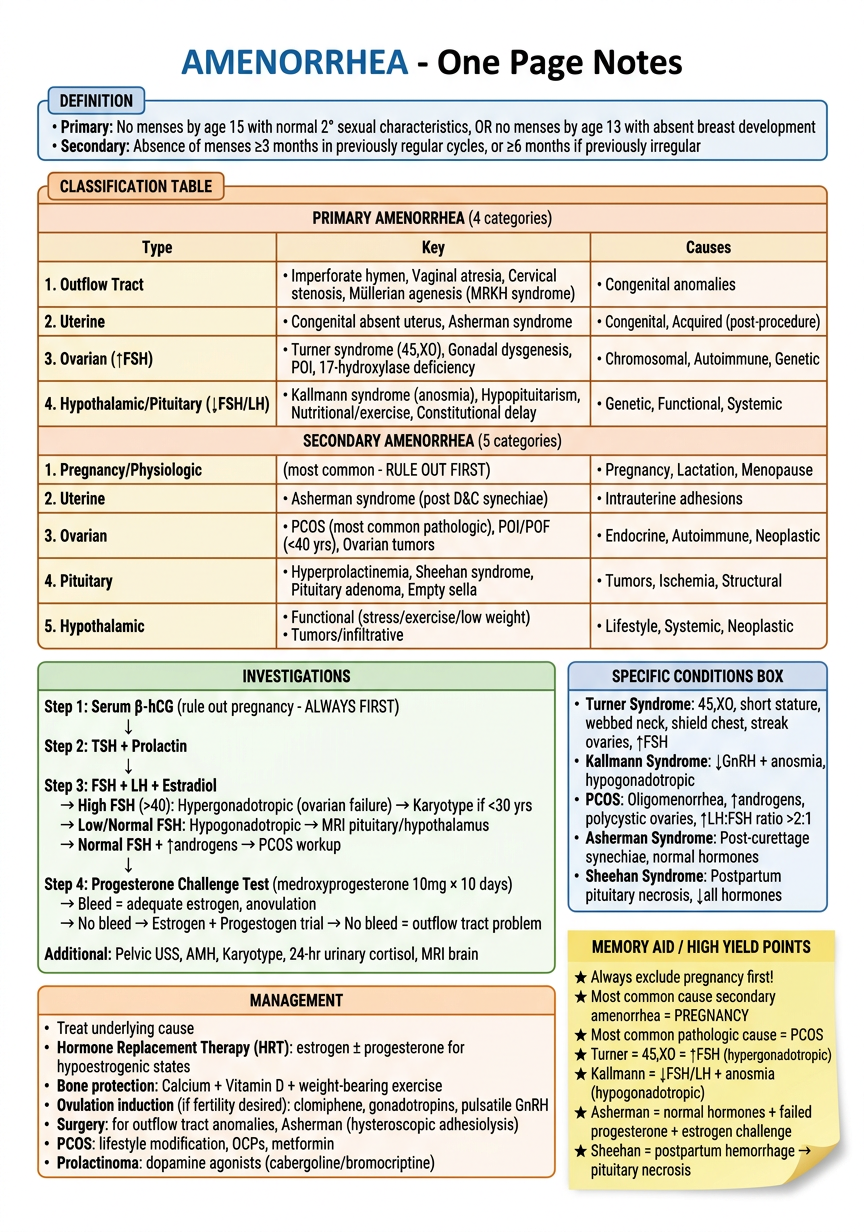
A detailed, clean, exam-ready one-page medical notes sheet titled "AMENORRHEA - One Page Notes" for a university final exam. The sheet is white/cream background with colored headings, organized in a structured layout with boxes, tables, and bullet points. Include the following sections: **DEFINITION (blue box):** - Primary: No menses by age 15 with normal 2° sexual characteristics, OR no menses by age 13 with absent breast development - Secondary: Absence of menses ≥3 months in previously regular cycles, or ≥6 months if previously irregular **CLASSIFICATION TABLE (organized grid):** | Type | Key | Causes | PRIMARY AMENORRHEA (4 categories): 1. Outflow Tract - Imperforate hymen, Vaginal atresia, Cervical stenosis, Müllerian agenesis (MRKH syndrome) 2. Uterine - Congenital absent uterus, Asherman syndrome 3. Ovarian (↑FSH) - Turner syndrome (45,XO), Gonadal dysgenesis, POI, 17-hydroxylase deficiency 4. Hypothalamic/Pituitary (↓FSH/LH) - Kallmann syndrome (anosmia), Hypopituitarism, Nutritional/exercise, Constitutional delay SECONDARY AMENORRHEA (5 categories): 1. Pregnancy/Physiologic (most common - RULE OUT FIRST) 2. Uterine - Asherman syndrome (post D&C synechiae) 3. Ovarian - PCOS (most common pathologic), POI/POF (<40 yrs), Ovarian tumors 4. Pituitary - Hyperprolactinemia, Sheehan syndrome, Pituitary adenoma, Empty sella 5. Hypothalamic - Functional (stress/exercise/low weight), Tumors/infiltrative **INVESTIGATIONS (green section):** Step 1: Serum β-hCG (rule out pregnancy - ALWAYS FIRST) Step 2: TSH + Prolactin Step 3: FSH + LH + Estradiol → High FSH (>40): Hypergonadotropic (ovarian failure) → Karyotype if <30 yrs → Low/Normal FSH: Hypogonadotropic → MRI pituitary/hypothalamus → Normal FSH + ↑androgens → PCOS workup Step 4: Progesterone Challenge Test (medroxyprogesterone 10mg × 10 days) → Bleed = adequate estrogen, anovulation → No bleed → Estrogen + Progestogen trial → No bleed = outflow tract problem Additional: Pelvic USS, AMH, Karyotype, 24-hr urinary cortisol, MRI brain **SPECIFIC CONDITIONS BOX:** Turner Syndrome: 45,XO, short stature, webbed neck, shield chest, streak ovaries, ↑FSH Kallmann Syndrome: ↓GnRH + anosmia, hypogonadotropic PCOS: Oligomenorrhea, ↑androgens, polycystic ovaries, ↑LH:FSH ratio >2:1 Asherman Syndrome: Post-curettage synechiae, normal hormones Sheehan Syndrome: Postpartum pituitary necrosis, ↓all hormones **MANAGEMENT (orange section):** • Treat underlying cause • Hormone Replacement Therapy (HRT): estrogen ± progesterone for hypoestrogenic states • Bone protection: Calcium + Vitamin D + weight-bearing exercise • Ovulation induction (if fertility desired): clomiphene, gonadotropins, pulsatile GnRH • Surgery: for outflow tract anomalies, Asherman (hysteroscopic adhesiolysis) • PCOS: lifestyle modification, OCPs, metformin • Prolactinoma: dopamine agonists (cabergoline/bromocriptine) **MEMORY AID / HIGH YIELD POINTS (yellow sticky note style):** ★ Always exclude pregnancy first! ★ Most common cause secondary amenorrhea = PREGNANCY ★ Most common pathologic cause = PCOS ★ Turner = 45,XO = ↑FSH (hypergonadotropic) ★ Kallmann = ↓FSH/LH + anosmia (hypogonadotropic) ★ Asherman = normal hormones + failed progesterone + estrogen challenge ★ Sheehan = postpartum hemorrhage → pituitary necrosis Use small neat fonts, colored borders for each section, arrows for diagnostic flowchart, very organized academic medical notes style suitable for printing on A4 paper
- Primary: No menses by age 15 (with normal development) OR age 13 (absent breast development)
- Secondary: ≥3 months absent in previously regular cycles; ≥6 months if previously irregular
- Rule out pregnancy (serum β-hCG) before anything else
- PCOS - most common pathologic cause of secondary amenorrhea; ↑LH:FSH ratio, ↑androgens
- Turner syndrome (45,XO) - primary amenorrhea, streak ovaries, ↑FSH (hypergonadotropic)
- Kallmann syndrome - ↓GnRH + anosmia (hypogonadotropic)
- Asherman syndrome - post-D&C synechiae; normal hormones, fails progesterone + estrogen challenge
- Sheehan syndrome - postpartum hemorrhage → pituitary necrosis → panhypopituitarism
- Hyperprolactinemia - check TSH + prolactin early; treat with cabergoline
- ↑FSH → ovarian failure → karyotype if <30 years
- ↓FSH/LH → hypothalamic/pituitary → MRI
- Normal + ↑androgens → PCOS workup
- Treat underlying cause
- HRT for hypoestrogenic states + bone protection (Ca²⁺ + Vit D)
- Ovulation induction if fertility desired
- Surgery for structural anomalies
Give a phot of one page notes on fever for opd treatment of patients
fever OPD outpatient treatment guidelines antipyretics when to refer 2024
A clean, professional, detailed one-page clinical quick-reference notes sheet titled "FEVER - OPD Management Guide" for outpatient/clinic use. White background with colored section boxes, tables, flowcharts, and bullet points. Well-organized, easy to read at a glance. Include all the following sections: **TOP HEADER - DEFINITION & NORMAL VALUES (blue box):** Fever = Core body temp ≥38.0°C (100.4°F) | Normal = 36.5–37.5°C • Low-grade: 37.5–38.0°C | Fever: 38.0–40.0°C | Hyperpyrexia: >40°C Measure: Oral / Axillary (subtract 0.5°C) / Rectal (most accurate, add 0.5°C) / Tympanic **SECTION 1 - INITIAL OPD ASSESSMENT (green box):** HISTORY: Duration | Pattern (continuous/remittent/intermittent/hectic) | Associated symptoms (cough, dysuria, rash, diarrhea, rigors) | Travel history | Medications | Immunization status | Sick contacts | Comorbidities EXAMINATION: Vitals (temp, HR, BP, RR, SpO2) | Hydration status | Skin (rash, petechiae, jaundice) | Lymph nodes | Throat | Ears | Chest | Abdomen | Neuro (neck stiffness, altered sensorium) **RED FLAGS - REFER/ADMIT (red box with warning symbol):** ⚠ Temp >40°C or <36°C (sepsis) | ⚠ Altered consciousness/neck stiffness | ⚠ Petechial/purpuric rash | ⚠ SpO2 <94% | ⚠ Hypotension (SBP <90 mmHg) | ⚠ HR >120 or RR >30 | ⚠ Immunocompromised/elderly/infant <3 months | ⚠ No oral intake / severe dehydration | ⚠ Fever >7 days without diagnosis | ⚠ Febrile neutropenia **SECTION 2 - FEVER PATTERN DIAGNOSIS CLUES (yellow table):** Pattern → Likely Cause Continuous (sustaining) → Typhoid, Lobar pneumonia, UTI Remittent (fluctuates, not to normal) → Typhoid, Infective endocarditis, Abscesses Intermittent (returns to normal) → Malaria (quotidian/tertian/quartan), Septicemia Hectic/Spiking (swinging) → Pyemia, Abscess, TB Pel-Ebstein (cyclic) → Lymphoma (Hodgkin's) Saddle-back (biphasic) → Dengue, Leptospirosis Fever + rash → Dengue, Measles, Meningococcemia, Drug fever Fever + rigors → Malaria, Pyelonephritis, Septicemia **SECTION 3 - BASIC OPD INVESTIGATIONS (orange box):** Routine (all febrile patients >3 days): CBC with differential | CRP | Blood culture (before antibiotics if sepsis suspected) | Urine R/M + culture | Peripheral blood smear (if malaria suspected) | CXR (if respiratory symptoms) Targeted: Dengue NS1/IgM/IgG | Widal test (typhoid, >5 days) | LFT, RFT | Malarial antigen (RDT) | Blood sugar | HIV if risk factors **SECTION 4 - ANTIPYRETIC TREATMENT (purple box, most prominent):** PHARMACOLOGICAL: 1. PARACETAMOL (first choice): 500–1000 mg oral q4–6h (max 4g/day adults) | Children: 10–15 mg/kg/dose q4–6h | Safe in pregnancy | Avoid in liver disease 2. IBUPROFEN: 200–400 mg oral q6–8h with food | Children: 5–10 mg/kg/dose | Avoid: renal disease, peptic ulcer, dengue, pregnancy (3rd trimester), <6 months 3. DICLOFENAC / MEFENAMIC ACID: second-line NSAIDs for adults 4. ASPIRIN: AVOID in children <12 yrs (Reye's syndrome risk) | Adults 300–600 mg q4–6h Combination: Paracetamol + Ibuprofen alternating every 3h for high/refractory fever NON-PHARMACOLOGICAL (tepid sponging, light clothing, adequate hydration, fan): • Tepid sponge bath (lukewarm water, NOT cold/ice) • Oral rehydration: 2–3 L/day fluids • Light loose clothing, rest • DO NOT use alcohol rubs **SECTION 5 - SPECIFIC COMMON CAUSES & OPD TREATMENT (teal box):** VIRAL FEVER (URTI/Flu): Paracetamol + rest + ORS + Vitamin C | No antibiotics needed | Antihistamine for cold symptoms DENGUE: Paracetamol ONLY (avoid NSAIDs/aspirin) | Daily CBC | Platelet monitoring | Admit if platelets <100,000 or bleeding MALARIA: Confirm with smear/RDT → Chloroquine (P.vivax) or Artemisinin combo therapy ACT (P.falciparum) → refer/admit if severe TYPHOID: Azithromycin 1g/day × 7 days (first-line OPD) OR Cefixime 400mg BD × 7–14 days | Avoid quinolones if resistance high | Admit if complications UTI: Nitrofurantoin / Trimethoprim / Cephalexin × 5–7 days (uncomplicated) | Urine C&S first PHARYNGITIS/TONSILLITIS: Amoxicillin 500mg TID × 7 days if Strep suspected | Benzathine Penicillin IM single dose if compliance concern **SECTION 6 - WHEN TO REVIEW (grey box):** Review in 48–72 hours if: No improvement | New symptoms develop | Fever increases | Investigations pending Advise patient: Return IMMEDIATELY if red flag signs appear **BOTTOM MEMORY BOX (sticky note style, yellow):** ★ Always take blood cultures BEFORE starting antibiotics ★ Dengue = Paracetamol ONLY — NO ibuprofen/aspirin (bleeding risk) ★ Children <3 months with fever = ADMIT (no exceptions) ★ Malaria smear x3 (on different days) to exclude ★ Fever >3 weeks without diagnosis = Fever of Unknown Origin (FUO) → full workup ★ ORS/hydration is as important as antipyretics Neat, clinical, color-coded, practical A4 layout, small readable fonts, suitable for printing and posting in an OPD clinic room
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.