Breast abscess
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast abscess"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from four major surgical/emergency/gynecology textbooks. Here is the full, synthesized answer:
Breast Abscess
Definition
A breast abscess is a localized collection of pus within the breast tissue, representing the end stage of a continuum that begins with cellulitis and progresses through mastitis. It occurs in both lactating (14%) and non-lactating women (86%). - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Classification
1. Lactational (Puerperal) Abscess
- Occurs in breastfeeding women, most commonly in the first 6 weeks postpartum or during weaning
- Results from milk stasis combined with bacterial entry through cracked or abraded nipples
- Most common organism: Staphylococcus aureus (including MRSA) and streptococci from the nursing infant's mouth
2. Non-Lactational Abscess
- More common overall (86% of all cases)
- Associated with smoking, diabetes, and obesity
- Can also follow nipple piercing or breast implant complications
- Often caused by mixed flora (aerobic and anaerobic), especially in recurrent cases
- Organisms: S. aureus most common (51.3%); MRSA in up to 8.6-20% of cases; mixed anaerobes (13.7%); anaerobic cocci, Bacteroides, Corynebacterium, E. coli, P. mirabilis
3. Subareolar Abscess (Periductal Mastitis / Duct Ectasia)
- A relapsing form unique to non-lactating women
- Associated with squamous metaplasia of the lactiferous ducts, with obstruction by inspissated debris
- Strongly linked to smoking and diabetes
- Can lead to nipple retraction, subareolar masses, and lactiferous duct fistula (mammillary sinus) to periareolar skin
- Mixed aerobic and anaerobic flora typical
Risk Factors
- Lactation (especially first 6 weeks)
- Smoking (also increases recurrence risk)
- Diabetes
- Obesity
- African American race
- Nipple piercing or breast implants
- Poor hygiene during breastfeeding
Clinical Features
| Feature | Details |
|---|---|
| Pain | Localized, often severe |
| Erythema | Overlying skin redness |
| Swelling/Induration | Tender palpable mass |
| Fever, chills, malaise | Systemic signs of infection |
| Fluctuance | Indicates frank pus formation |
- Cellulitis phase: diffuse erythema, no discrete fluctuant mass; ultrasound shows thickened hyperechoic skin
- Abscess phase: localized fluctuant mass; ultrasound shows inhomogeneous, hyperechoic collection, often multiloculated
Important: Failure to improve with antibiotics requires urgent surgical consultation and possible biopsy to exclude inflammatory carcinoma. Inflammatory carcinoma can closely mimic a breast abscess. - Tintinalli's Emergency Medicine
Investigations
- Ultrasound (US): First-line imaging - confirms abscess vs. cellulitis, identifies loculations, guides aspiration. Appearance: inhomogeneous, hyperechoic mass with posterior acoustic enhancement
- Pus culture and sensitivity: Always send aspirated pus, including MRSA screening
- Milk culture: In lactating patients; if delivered in hospital, assume penicillin-resistant Staphylococcus
- Mammography: Recommended in women >30 years, performed after the acute phase resolves
- Biopsy: Required if erythema persists despite treatment to rule out inflammatory carcinoma
Management
Step 1 - Early/Cellulitis Stage (No Frank Abscess)
- Antibiotics alone may be curative
- Apply heat; encourage continued breast emptying (lactating)
Antibiotic selection:
| Setting | Drug of Choice |
|---|---|
| Non-severe, no MRSA risk | Dicloxacillin or cephalexin (oral) |
| Non-lactating, broader coverage needed | Amoxicillin-clavulanate, dicloxacillin |
| High community MRSA prevalence | TMP-SMX or clindamycin |
| Severe infection / inpatient | Vancomycin IV (± metronidazole for deeper/anaerobic coverage) |
| Non-lactating: anaerobic coverage needed | Clindamycin, amoxicillin-clavulanate, or metronidazole added |
| Beta-lactam allergy | Clindamycin |
Infections should respond within 48 hours. If not, escalate.
Step 2 - Frank Abscess: Needle Aspiration (First-Line)
- Ultrasound-guided needle aspiration is now the standard of care for most breast abscesses
- For abscesses <3 cm: single-needle aspiration
- For abscesses ≥3 cm: ultrasound-guided catheter drainage preferred
- Advantages over I&D: less scarring, does not interfere with breastfeeding, no procedural sedation required
- Mean of 3.5 aspirations required for complete resolution; repeat daily or every other day
- A single aspiration is sufficient in ~50% of non-lactational cases
Step 3 - Surgical Incision and Drainage (I&D)
Reserved for:
- Skin compromise (thinning, necrosis) overlying the abscess
- Failure to resolve after needle aspiration + antibiotics
- Multiloculated abscesses (usually require general anaesthesia)
Surgical technique (Pye's Surgical Handicraft):
- Radial incision near nipple/areola (to minimize duct damage); follow Langer's lines elsewhere
- Enter abscess cavity with scissors
- Send swab of pus for culture
- Digitally break down all loculi into one large cavity
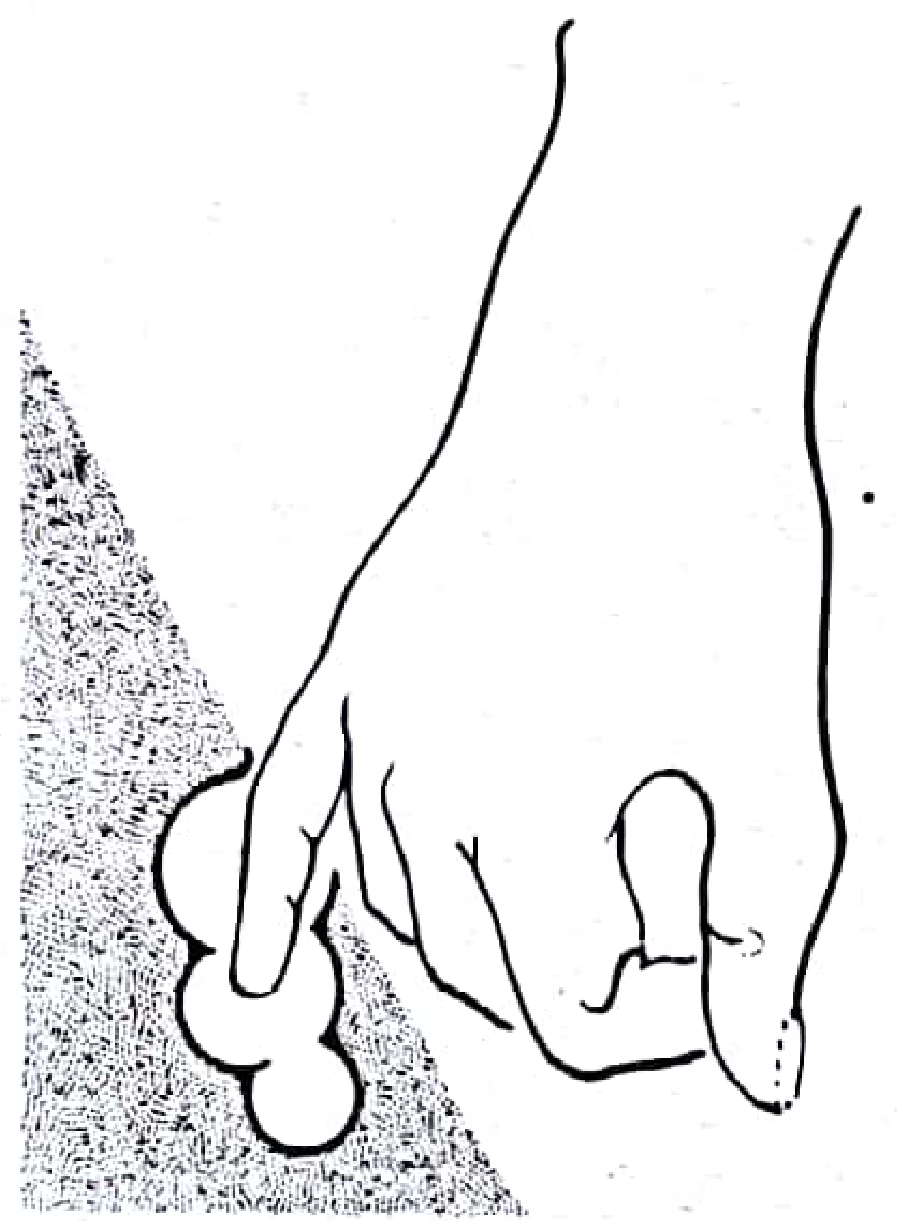
Digital breakdown of loculi in breast abscess - Pye's Surgical Handicraft
- Curettage or dissection of necrotic material, then dry gauze wipeout
- If drainage is difficult: counter-incision in the dependent (lower) part + soft rubber drain
- Dry dressings, wool padding, supporting bandage; continue antibiotics
Specific Situations
Lactating Women
- Do not stop breastfeeding from the affected breast in early mastitis; continue to empty the breast (reduces milk stasis)
- If abscess forms: percutaneous drainage + continue breastfeeding (non-infected side at minimum)
- Breastfeeding can usually be resumed from the affected side after drainage
Antibioma (Sterile Abscess)
- If antibiotics are continued without drainage, pus may be sterilized, forming a hard, palpable mass resembling carcinoma
- Diagnosed by aspirating pus that yields no bacterial growth
- Treated by aspiration or formal drainage
Subareolar / Recurrent Abscess
- Multiple aspirations often required
- Definitive treatment (after the acute infection resolves): excision of the entire subareolar duct complex
- I&D alone has a high recurrence rate
- Rarely, repeated infections require excision of the nipple and areola
- Lactiferous duct fistula (mammillary sinus) is confirmed as the cause of reinfection in virtually all recurrent cases
- Counsel patients on smoking cessation
Differential Diagnosis
- Cellulitis
- Mastitis
- Periductal mastitis / duct ectasia
- Ruptured breast cyst
- Inflammatory breast carcinoma (most important to exclude)
- Metastatic cancer
- Tuberculosis of the breast
- Paget's disease
- Idiopathic granulomatous mastitis
Key Points Summary
| Lactational | Non-Lactational | Subareolar | |
|---|---|---|---|
| Common organisms | S. aureus, Streptococcus | S. aureus, mixed flora | Aerobic + anaerobic mixed |
| Risk factors | Cracked nipple, milk stasis | Smoking, DM, obesity | Smoking, squamous metaplasia |
| First-line Rx | Antibiotics + breast emptying | US-guided aspiration + abx | Aspiration + abx |
| Definitive surgical Rx | I&D if aspiration fails | I&D if aspiration fails | Subareolar duct excision |
| Recurrence | Low | Low (higher in smokers 10%) | High without duct excision |
Sources: Sabiston Textbook of Surgery; Berek & Novak's Gynecology; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; Pye's Surgical Handicraft (22nd ed.)
Breast abscess
Finding Sources
Finding Sources
Searching PubMed
"breast abscess"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Breast Abscess
A breast abscess is a localized collection of pus within breast tissue. It represents the end of a continuum: cellulitis → mastitis → abscess. Overall, 86% occur in non-lactating women and only 14% in lactating women. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Classification
1. Lactational (Puerperal) Abscess
- Occurs during breastfeeding, most commonly in the first 6 weeks postpartum or during weaning
- Precipitated by milk stasis (missed feeds, weaning) + bacterial entry through cracked/abraded nipple
- Organism from the nursing infant's mouth: S. aureus (including MRSA), streptococci
- Mastitis incidence in lactating women: 2-33%
2. Non-Lactational Abscess
- The more common form (86%)
- Associated with smoking, diabetes, obesity
- Also linked to nipple piercing, breast implants
- More likely to be multiloculated and caused by mixed flora
3. Subareolar Abscess / Periductal Mastitis
- Relapsing chronic form in non-lactating women
- Caused by squamous metaplasia of the lactiferous ducts → obstruction by inspissated debris
- Strongly linked to smoking
- Leads to: nipple retraction/inversion, subareolar mass, and lactiferous duct fistula (mammillary sinus) to periareolar skin
- Mixed aerobic + anaerobic flora
Microbiology
| Organism | Frequency |
|---|---|
| Staphylococcus aureus | 51.3% (most common overall) |
| MRSA | 8.6-20% (rising) |
| Mixed anaerobes | 13.7% |
| Anaerobic cocci | 6.3% |
| Streptococcus pyogenes, E. coli, Bacteroides, Corynebacterium, Proteus mirabilis, P. aeruginosa | Less common |
Mixed flora are more common in recurrent abscesses. Hospital deliveries: assume penicillin-resistant Staphylococcus. - Berek & Novak's Gynecology; Pye's Surgical Handicraft
Risk Factors
- Lactation (especially cracked nipples)
- Smoking (increases incidence AND recurrence)
- Diabetes mellitus
- Obesity
- African American race
- Nipple piercing / breast implants
- Poor breastfeeding hygiene
Clinical Features
| Symptom/Sign | Notes |
|---|---|
| Breast pain | Localised, often severe |
| Erythema | Overlying skin redness and warmth |
| Swelling, induration | Tender mass |
| Fluctuance | Indicates frank pus - may be deep |
| Fever, chills, malaise | Systemic toxicity |
- Early stage (cellulitis predominates): diffuse, no discrete mass - diagnosis may be difficult
- Late stage: fluctuant, loculated mass; patient may appear toxic
Red flag: If erythema does not improve with antibiotics, inflammatory breast carcinoma must be excluded by biopsy. It can mimic infection exactly. - Tintinalli's Emergency Medicine
Investigations
- Breast ultrasound - first-line imaging
- Cellulitis: diffuse thickened, hyperechoic skin, increased echogenicity of subcutaneous tissue
- Abscess: inhomogeneous, hyperechoic mass; identifies loculations, confirms pus, guides aspiration
- Pus culture and sensitivity - always send aspirated material (MRSA screen)
- Milk culture - in lactating patients
- Mammography - recommended for women >30 years, done after acute phase resolves (not during)
- Core biopsy - if diagnosis uncertain, or erythema fails to resolve, to exclude carcinoma
Management
Step 1: Early Cellulitis / Mastitis (No Frank Abscess)
- Antibiotics alone may be curative - reassess at 48 hours
- Lactating: support breast with firm bandage; breastfeeding may be continued or discontinued (resumed later)
- Apply warmth; encourage continued breast emptying
Antibiotic Selection:
| Clinical Setting | Drug(s) of Choice |
|---|---|
| Non-severe, no MRSA risk | Dicloxacillin or cephalexin (oral) |
| Non-severe, broader coverage | Amoxicillin-clavulanate |
| High community MRSA prevalence | TMP-SMX or clindamycin |
| Non-lactating (anaerobic coverage needed) | Add metronidazole, or use amoxicillin-clavulanate |
| Severe infection / inpatient | Vancomycin IV ± metronidazole |
| Non-severe, severe infection (non-lactating) | 3rd-gen cephalosporin (ceftazidime), fluoroquinolone, or linezolid |
| Beta-lactam allergy | Clindamycin |
Outpatient management is appropriate without systemic toxicity. Patients with toxicity need admission.
Step 2: Frank Abscess - Ultrasound-Guided Needle Aspiration (First-Line)
US-guided needle aspiration is now the standard of care for most breast abscesses, replacing formal I&D as first-line treatment. - Roberts and Hedges'
- Abscess <3 cm: needle aspiration (repeat daily or every other day as needed)
- Abscess ≥3 cm: ultrasound-guided catheter drainage preferred
- Mean of 3.5 aspirations required for complete resolution
- A single aspiration is sufficient in ~50% of non-lactational cases
- Always send aspirated pus for culture
Advantages over I&D: less scarring, does not interfere with breastfeeding, no sedation required
Step 3: Surgical Incision and Drainage (I&D)
Reserved for:
- Compromise/thinning of overlying skin
- Failure to resolve after aspiration + antibiotics
- Multiloculated abscess not amenable to aspiration
Surgical technique:
- Incision: radial near nipple/areola (to protect ducts); follow Langer's lines elsewhere
- Enter abscess cavity with scissors; swab pus for culture
- Digitally break down all loculi into one large cavity
- Curette or dissect necrotic material; wipe out with dry gauze
- If drainage is difficult: counter-incision in dependent (lower) part of breast + soft rubber drain
- Dry dressings, wool padding, supporting bandage; continue antibiotics; dress frequently
Special Situations
Antibioma (Sterile Abscess)
- Occurs when antibiotics are continued without drainage - pus becomes sterilized
- Presents as a hard, discrete, palpable breast mass - closely resembles carcinoma
- Diagnosis: aspirate yields pus with no growth on culture
- Treatment: aspiration or formal drainage
Subareolar / Recurrent Abscess
- Acute phase: aspiration + antibiotics covering aerobic and anaerobic organisms; warm soaks
- Definitive treatment (after full resolution of acute infection): excision of the entire subareolar duct complex + IV antibiotic cover
- I&D alone has a high recurrence rate - lactiferous duct fistula is the cause of reinfection in virtually all recurrent cases
- Rarely: repeated infections require excision of the nipple and areola
- Always counsel on smoking cessation (major modifiable risk)
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Cellulitis | No discrete abscess on US; diffuse erythema |
| Mastitis | Diffuse, no fluctuance; may respond to antibiotics |
| Periductal mastitis | Non-lactating; subareolar; relapsing; nipple retraction |
| Ruptured breast cyst | History of cyst; US shows collapsed cyst |
| Inflammatory breast carcinoma | Fails antibiotics; peau d'orange; biopsy needed |
| Tuberculosis of the breast | Rare; chronic; AFB stain/culture |
| Idiopathic granulomatous mastitis | Biopsy: non-necrotizing granulomas; cultures negative |
| Hidradenitis suppurativa | Recurrent; affects inferior breast folds; sinus tracts; scarring |
Summary Table
| Lactational | Non-Lactational | Subareolar | |
|---|---|---|---|
| Common organisms | S. aureus, Streptococcus | S. aureus, mixed flora, MRSA | Aerobic + anaerobic mixed |
| Key risk factors | Cracked nipple, milk stasis | Smoking, DM, obesity | Smoking, squamous metaplasia |
| First-line Rx | Antibiotics + breast emptying | US-guided aspiration + antibiotics | Aspiration + antibiotics |
| Drainage threshold | Abscess formation | Abscess formation | Abscess formation |
| Definitive surgery | I&D if aspiration fails | I&D if aspiration fails | Subareolar duct excision |
| Recurrence rate | Low | ~10% (higher in smokers) | High without duct excision |
Sources: Sabiston Textbook of Surgery; Berek & Novak's Gynecology; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; Pye's Surgical Handicraft (22nd ed.)
And it's cauin short to make notes of breast abscess se
Here are concise notes on Breast Abscess for quick revision:
BREAST ABSCESS - Short Notes
Definition
Localized collection of pus in breast tissue. Part of a continuum: Cellulitis → Mastitis → Abscess
Types
| Type | Key Feature |
|---|---|
| Lactational | 1st 6 weeks postpartum / weaning |
| Non-lactational | Smokers, diabetics, obese (most common - 86%) |
| Subareolar | Duct ectasia, relapsing, smoking-related |
Causative Organisms
- #1: S. aureus (51%) - including MRSA (up to 20%)
- Streptococcus, mixed anaerobes, Bacteroides
- Subareolar: mixed aerobic + anaerobic flora
Risk Factors
- Lactation + cracked nipple
- Smoking (also causes recurrence)
- Diabetes, obesity
- Nipple piercing, breast implants
Clinical Features
- Pain, swelling, erythema, warmth
- Tender fluctuant mass
- Fever, chills, malaise
- Systemic toxicity in severe cases
Investigations
- Ultrasound - confirms abscess, guides aspiration
- Inhomogeneous hyperechoic mass
- Pus culture + sensitivity (always)
- Mammography (women >30 yrs, after acute phase)
- Biopsy - if no improvement → exclude inflammatory carcinoma
Treatment
Antibiotics
| Setting | Drug |
|---|---|
| Non-severe, no MRSA risk | Dicloxacillin / Cephalexin |
| MRSA risk | TMP-SMX or Clindamycin |
| Severe / IV | Vancomycin ± Metronidazole |
| Beta-lactam allergy | Clindamycin |
Drainage
| Abscess Size | Approach |
|---|---|
| <3 cm | US-guided needle aspiration (repeat daily/alternate day; mean 3.5 aspirations) |
| ≥3 cm | US-guided catheter drainage |
| Fails aspiration | Surgical I&D |
Surgical I&D Technique
- Radial incision near nipple (protect ducts) / Langer's lines elsewhere
- Enter with scissors → swab pus
- Digitally break down loculi into one cavity
- Curette necrotic tissue
- Counter-incision + rubber drain if drainage poor
- Dressings + antibiotics
Special Points
| Condition | Key Fact |
|---|---|
| Antibioma | Sterile abscess from antibiotics without drainage; mimics carcinoma; pus on aspiration but no growth |
| Subareolar/recurrent | Definitive Rx = excision of subareolar duct complex (not just I&D) |
| Lactating | Continue breastfeeding; empty breast; antibiotics first |
Differentials to Remember
- Inflammatory breast carcinoma ← most important (biopsy if no response to antibiotics)
- Mastitis, cellulitis, ruptured cyst
- Granulomatous mastitis, TB breast, hidradenitis suppurativa
High-Yield Points
- 86% non-lactating, 14% lactating
- US-guided aspiration = standard of care (not I&D first)
- Smoking → recurrence → excise subareolar ducts
- No response to antibiotics → biopsy to exclude carcinoma
- Antibioma = sterile abscess = mimics cancer
This is a shared conversation. Sign in to Orris to start your own chat.