Ecg
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive breakdown of Atrial Fibrillation (AF) and Atrial Flutter on ECG, sourced from Braunwald's Heart Disease, Tintinalli's Emergency Medicine, Guyton & Hall, Rosen's Emergency Medicine, and Goldman-Cecil Medicine.
Atrial Fibrillation (AF) on ECG
ECG Hallmarks
| Feature | Detail |
|---|---|
| P waves | Absent - replaced by chaotic, low-amplitude fibrillatory baseline (flat or undulating) |
| Fibrillatory waves | Best seen in inferior leads (II, III, aVF) and V1; can be coarse or fine |
| Ventricular rhythm | Irregularly irregular - the defining feature |
| QRS morphology | Narrow, unless preexisting bundle branch block or accessory pathway (WPW) |
| Atrial rate | >350-600 beats/min (chaotic, not countable) |
| Ventricular rate | Typically 120-170 beats/min with intact AV node; slower if on nodal-blocking agents |
Key rule: If the ventricular rate exceeds 200 beats/min, strongly suspect an accessory conduction pathway (WPW). This can present as wide, irregular QRS complexes and must not be mistaken for VT.
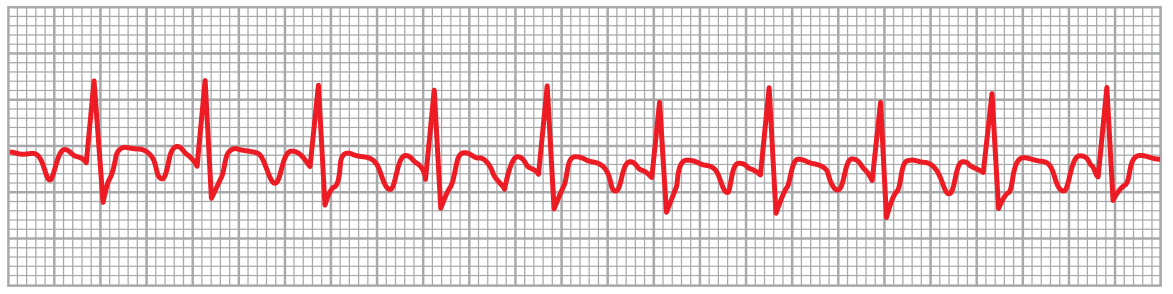
ECG Tracing - Atrial Fibrillation (lead II)
Guyton & Hall Textbook of Medical Physiology - Fig. 13.20:

Note the complete absence of P waves, low-amplitude undulating baseline, and the variable spacing of QRS complexes confirming irregularly irregular rhythm.
Three Clinical Examples of AF
Tintinalli's Emergency Medicine - Fig. 18-10:
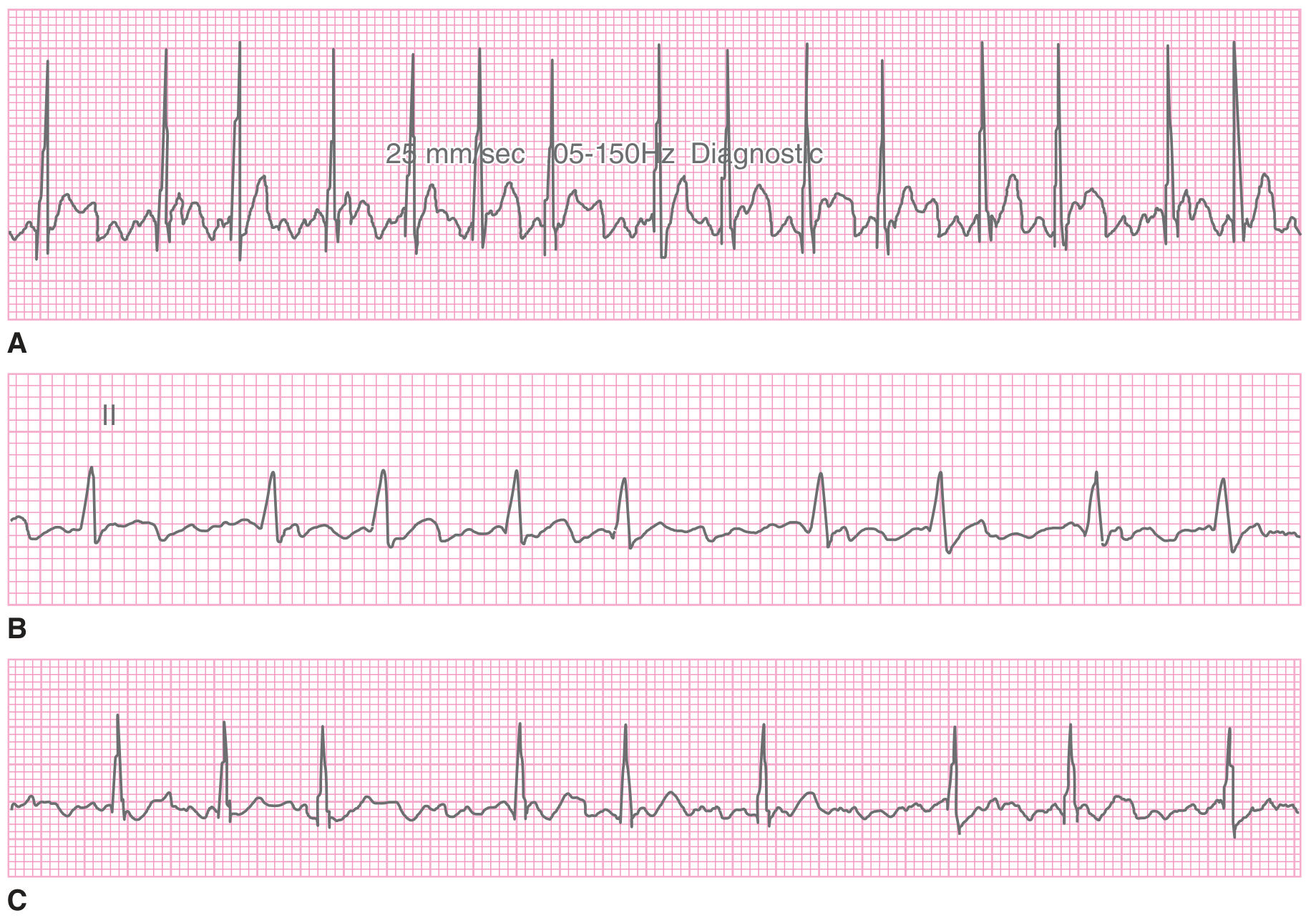
- A: Rapid ventricular response with chaotic baseline
- B: Controlled rate (Lead II) - no P waves, irregular QRS
- C: Slow ventricular response (possibly rate-controlled or on nodal agents)
Why the Rhythm is Irregular
Multiple small depolarization waves spread in all directions through the atria simultaneously. Atrial impulses bombard the AV node irregularly at rates >600/min. The AV node has a refractory period of ~0.35 sec, so impulses pass randomly - the interval between successive ventricular beats varies from ~0.35 to ~0.95 sec, producing the classic "irregularly irregular" pattern. (Guyton & Hall)
Ashman Phenomenon
In AF, an early impulse following a long R-R interval may conduct aberrantly due to differential refractoriness of the bundle branches. This produces a RBBB-pattern wide beat called an Ashman beat - easily confused with a PVC or run of VT. The key: look for the preceding long-short cycle and overall irregular rhythm context.
Atrial Flutter on ECG
ECG Hallmarks
| Feature | Detail |
|---|---|
| P waves | "Sawtooth" flutter waves - regular, uniform morphology |
| Flutter wave polarity | Counterclockwise (typical): Negative in II, III, aVF; positive in V1 |
| Flutter wave polarity | Clockwise: Positive in II, III, aVF; negative in V1 |
| Atrial rate | ~300 beats/min (range 250-350) |
| Ventricular rate | 150/min with 2:1 block (most common), 100/min with 3:1, etc. |
| Ventricular rhythm | Usually regular; may be irregular with variable AV block |
High-yield tip: A narrow-complex tachycardia at ~150 bpm (+/-5) should strongly suggest atrial flutter with 2:1 conduction until proven otherwise.
ECG Tracing - Atrial Flutter (lead II, 2:1 block)
Guyton & Hall - Fig. 13.21:
Classic sawtooth P waves at 250 beats/min with 2:1 AV block, giving a ventricular rate of 125 beats/min.
Flutter with Carotid Sinus Massage (CSM)
Tintinalli's Emergency Medicine - Fig. 18-11:
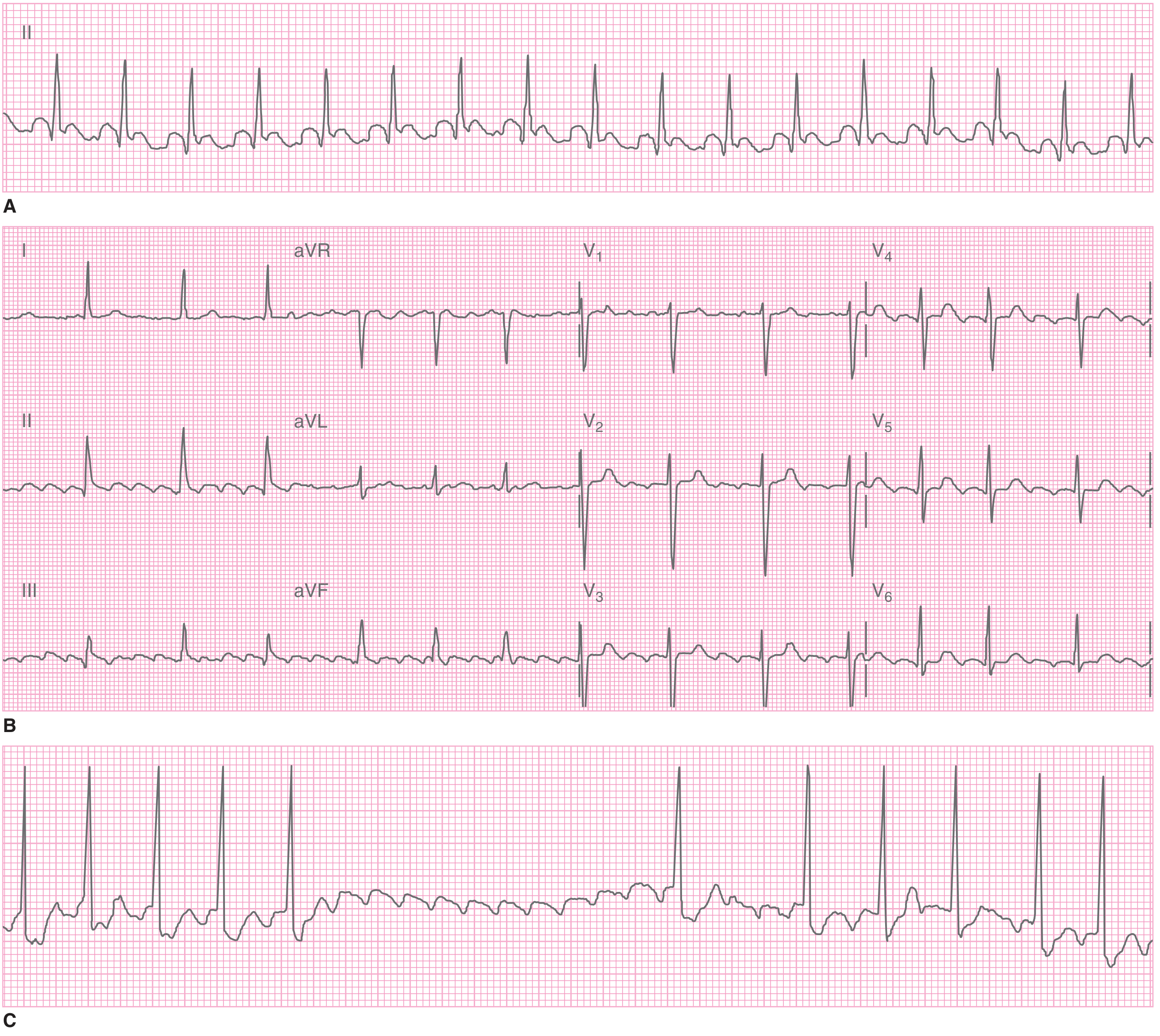
- A: Regular narrow-complex tachycardia at 155 bpm - suggestive of flutter with 2:1
- B: 12-lead showing sawtooth flutter waves best in leads II, III, aVF
- C: CSM induces transient AV block, unmasking the flutter waves clearly
Carotid sinus massage (or adenosine) is a useful bedside maneuver - it transiently increases AV nodal block, revealing underlying flutter waves that may be hidden in the QRS-T at fast rates.
AF vs. Atrial Flutter - Quick Comparison
| Feature | AF | Atrial Flutter |
|---|---|---|
| P waves | Absent (chaotic baseline) | Sawtooth flutter waves |
| Atrial rate | >350-600/min | ~300/min |
| Ventricular rhythm | Irregularly irregular | Usually regular |
| Ventricular rate | Variable, 120-170/min | Usually 150/min (2:1) |
| Best lead to see activity | V1, inferior leads | Inferior leads (II, III, aVF) |
| AV conduction | Variable, random | Fixed or variable ratio (2:1, 3:1) |
Clinical Classification of AF
- Paroxysmal - terminates spontaneously or with treatment within 7 days
- Persistent - lasts >7 days or requires cardioversion
- Long-standing persistent - continuous >1 year
- Permanent - decision made not to restore sinus rhythm
Common Causes of AF
- Hypertension (most common)
- Ischemic heart disease
- Valvular disease (especially mitral)
- Heart failure / cardiomyopathy
- Hyperthyroidism
- Alcohol binge ("holiday heart syndrome")
- Pericarditis, myocarditis
- Pulmonary embolism
- Sick sinus syndrome
- Post-cardiac surgery
- WPW / accessory pathway
- Idiopathic ("lone AF")
Key Complications & Scoring
- Stroke risk: AF carries a 5-fold increased stroke risk. Use CHA₂DS₂-VASc score to guide anticoagulation (score ≥2 in males, ≥3 in females = anticoagulate).
- Bleeding risk: HAS-BLED score helps estimate bleeding risk before starting anticoagulation.
- Rate vs. rhythm control: ED management involves rate control (beta-blockers, calcium channel blockers), rhythm conversion (cardioversion or pharmacologic), and anticoagulation.
- Thromboembolic risk with cardioversion: If AF duration >48 hours, risk of embolism increases - 3-4 weeks of anticoagulation or TOE to exclude left atrial thrombus is needed before cardioversion.
Sources: Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, Guyton & Hall Medical Physiology, Goldman-Cecil Medicine, Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.