

IMG_0674.jpg
IMG_0675.jpg
This is the history and admissions diagnosis our doc requested for plain chest ct scan may I know why and what’s the use of it
analyse_media
analyse_media
Reading File
Searching the Web
plain chest CT scan multiple rib fractures pulmonary contusion trauma indications
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a full, clear explanation based on this patient's specific case and backed by authoritative surgical and emergency medicine textbooks.
Why a Plain Chest CT Was Ordered for This Patient
The Patient's Situation
Patient: Bagube, San Jay - 34-year-old male
Mechanism: Motorcycle-vs-motorcycle collision (July 12, 2026 at 6:20 PM, Bolinao)
Admission Diagnosis: Multiple rib fractures (2nd, 3rd, 4th ribs) with pulmonary contusion, secondary to vehicular crash
Ward: Surgery
Why CT Chest Specifically?
1. Plain Chest X-ray Misses Pulmonary Contusion Early On
The biggest reason CT was ordered is that a plain chest X-ray (CXR) has low sensitivity for pulmonary contusion, especially in the first few hours after trauma.
"Radiographic evidence of pulmonary contusion can take 6 hours to be evident, and may not be present until 48 hours post-injury."
- Rockwood and Green's Fractures in Adults, 10th ed., p. 2085
"Chest CT scan is particularly valuable to identify a pulmonary contusion in the acute phase after injury because plain chest X-ray films have a low sensitivity."
- Rosen's Emergency Medicine, 9th ed.
CT detects at least twice as many pulmonary contusions as plain X-ray. In studies, isolated contusions seen only on CT (occult contusions) had a mortality of only 2.6% - meaning early detection changes management.
2. CT Accurately Identifies All Three Rib Fractures and Their Severity
This patient has fractures at the 2nd, 3rd, and 4th ribs - the upper thoracic cage. A plain CXR is often poor at counting fractures, detecting displacement, or showing whether the fracture ends are overlapping (which predicts malunion).
"A CT scan is not indicated to confirm suspected isolated rib fracture, but it will identify multiple-level fractures and associated pulmonary injury, such as pneumothorax or hemothorax, with much greater accuracy than additional chest X-ray views."
- Rosen's Emergency Medicine
3. Ruling Out Life-Threatening Associated Injuries
Multiple rib fractures from high-energy trauma (motorcycle crash) carry a risk of several hidden injuries that can be fatal if missed. Chest CT screens for all of these in a single scan:
| Injury to Rule Out | Why It Matters |
|---|---|
| Pneumothorax | Air in pleural space - can tension and cause cardiac arrest |
| Hemothorax | Blood in chest - can cause hemorrhagic shock |
| Aortic injury | Upper rib fractures are associated with great vessel trauma |
| Flail chest | 3 adjacent ribs fractured in 2 places = segment moves paradoxically |
| Tracheal/bronchial laceration | Rare but life-threatening |
| Diaphragm injury | Can be missed on CXR |
The CT imaging of blunt chest trauma reference classifies these as the core injuries detectable only on CT.
4. Grading Pulmonary Contusion Severity - Which Guides Treatment
CT allows the doctor to grade the contusion by how much lung volume is involved:
- Mild: less than 18% lung volume
- Moderate: 18-28%
- Severe: more than 28%
This directly determines whether the patient needs:
- Supplemental oxygen only
- Non-invasive ventilation (CPAP/BiPAP)
- Mechanical ventilation (intubation)
- Dual-lung ventilation in extreme cases
"CT scanning is very sensitive in identifying pulmonary contusions immediately and is often used in making this diagnosis."
- Rockwood and Green's, p. 2085
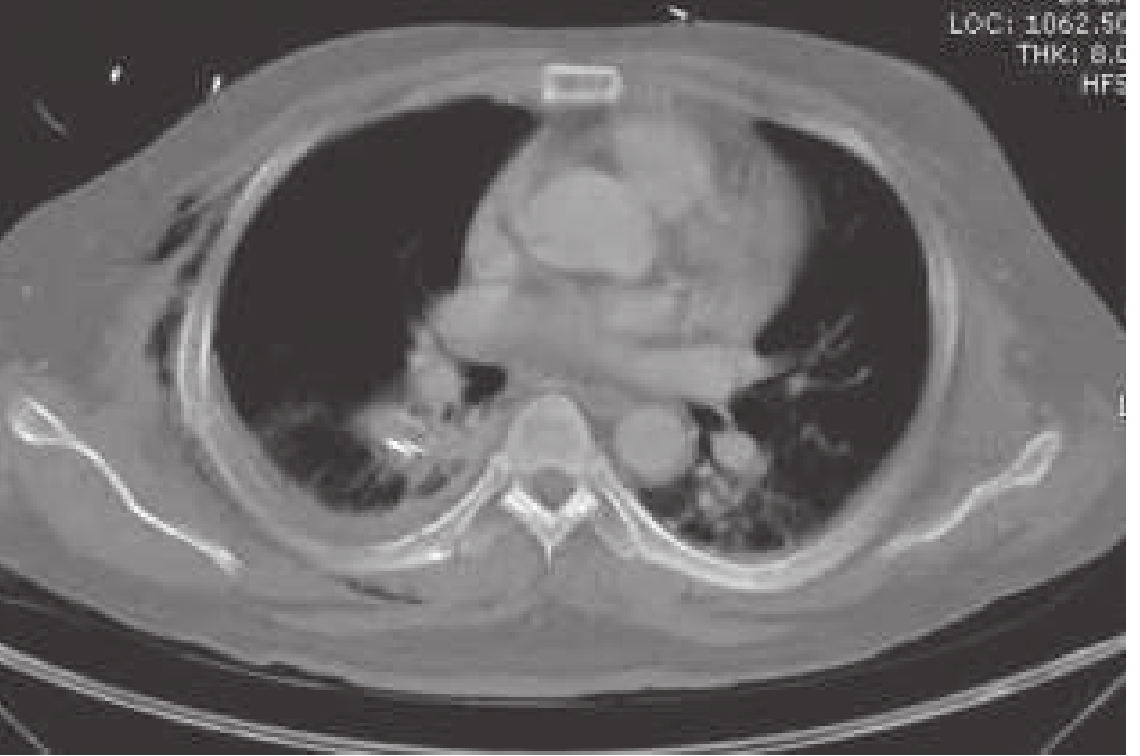
Here is what pulmonary contusion looks like on CT - the hazy/white opacification in the lung (left image shows bilateral contusions; right shows contusion with associated pneumothorax):

5. Why "Plain" (Non-Contrast) CT?
"Plain" means without IV contrast dye. For initial lung/rib assessment, a non-contrast CT is standard because:
- Lung windows do not require contrast to see contusion, pneumothorax, or rib fractures
- It avoids the risk of contrast reactions or kidney injury
- It is faster and appropriate for acute trauma triage
(If aortic injury was highly suspected, a contrast CT angiogram would be added instead.)
Summary Table
| CT Chest Purpose | Clinical Reason for This Patient |
|---|---|
| Detect pulmonary contusion | CXR may be normal in first 6-48 hrs; CT sees it immediately |
| Count and characterize rib fractures | Fractures 2nd-4th rib on the same side raise concern for flail segment |
| Rule out pneumothorax/hemothorax | High-energy blunt trauma has 60% rib fracture rate with associated lung injury |
| Rule out vascular injury | Upper rib fractures near great vessels |
| Grade severity for management decisions | Degree of contusion determines ventilation strategy |
In short, the plain chest CT is the gold standard imaging for this patient because the admission diagnosis of multiple rib fractures with pulmonary contusion after a motorcycle crash demands far more detail than a simple X-ray can provide - and the treatment plan, surgical considerations, and monitoring intensity all depend on what the CT shows.
Do we need labs for this
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
laboratory workup multiple rib fractures pulmonary contusion blunt chest trauma CBC ABG coagulation
Reading File
Reading Web Page
https://emedicine.medscape.com/article/428723-workup
Yes - labs are definitely needed for this patient. Here is a breakdown of exactly which tests, why each one is ordered, and what you are looking for.
Required Labs for Bagube, San Jay (Multiple Rib Fx + Pulmonary Contusion, MVA)
1. Complete Blood Count (CBC)
Why: Standard for all trauma patients. Rib fractures can cause internal bleeding (hemothorax, intercostal vessel laceration) that is not immediately obvious clinically.
- Hemoglobin/Hematocrit - gauges blood loss; a dropping Hgb over serial checks signals ongoing hemorrhage
- WBC - baseline; later elevations flag developing pneumonia or sepsis (common complications of pulmonary contusion)
- Platelets - needed before any surgical intervention
"A CBC is a routine laboratory test for most trauma patients. It helps gauge blood loss, though it is not entirely reliable for accurately determining acute blood loss. Other important information includes platelet and WBC counts."
- Blunt Chest Trauma Workup, Medscape/eMedicine
2. Arterial Blood Gas (ABG)
This is the most important lab specifically for pulmonary contusion.
Pulmonary contusion causes a ventilation-perfusion (V/Q) mismatch - blood passes through damaged, flooded alveoli without getting oxygenated. The ABG measures this directly.
- PaO2 and O2 saturation - detects hypoxemia (low oxygen)
- PaCO2 - detects hypoventilation (high CO2 means the patient is not breathing adequately)
- pH - identifies respiratory acidosis
- A-a gradient (alveolar-arterial O2 difference) - widening A-a gradient is one of the earliest and most accurate indicators of pulmonary contusion severity
"Arterial blood gas assessment is helpful in making the diagnosis, because a widening alveolar-arterial oxygen difference indicates a decreasing pulmonary diffusion capacity of the contused lung, and it is one of the earliest and most accurate means of assessing the current status, progress, and prognosis."
- Rosen's Emergency Medicine, 9th ed.
ABG results also directly guide the treatment decision:
- PaO2 > 80 mmHg on room air = supplemental O2 only
- PaO2 60-80 mmHg = non-invasive ventilation (CPAP/BiPAP)
- PaO2 < 60 mmHg or rising PaCO2 = intubation
3. Serum Lactate
A marker of tissue hypoperfusion and shock. In MVA trauma, a high lactate (> 2 mmol/L) means the body is not getting enough oxygen - this can be from hemorrhage, tension pneumothorax, or severe pulmonary contusion. Serial lactate levels track whether resuscitation is working.
4. Type and Crossmatch (Blood Typing)
Why: Hemothorax from rib fractures can cause significant hemorrhage requiring blood transfusion. This must be set up early - you do not want to be scrambling for compatible blood when the patient crashes.
"Type and crossmatch are among the most important blood tests in the evaluation and management of a seriously injured trauma patient, especially one predicted to require major operative intervention."
- Medscape Blunt Chest Trauma Workup
5. Coagulation Studies (PT, PTT, INR)
Trauma activates the clotting cascade and can cause coagulopathy - either a clotting problem or, in severe cases, Disseminated Intravascular Coagulation (DIC). This matters especially if surgery or chest tube insertion is needed.
6. Basic Metabolic Panel (BMP) / Electrolytes + Creatinine
- Creatinine/BUN - baseline kidney function (important before IV fluids and medications)
- Electrolytes (Na, K) - trauma and pain cause stress hormone surges that shift electrolytes
- Glucose - stress hyperglycemia is common after trauma
7. Cardiac Enzymes (Troponin I or T)
The 2nd, 3rd, and 4th ribs are directly over the heart. High-impact anterior chest trauma can cause myocardial contusion (bruising of the heart muscle). A raised troponin signals this.
"Elevated serum troponin I levels correlate with the presence of echocardiographic or ECG abnormalities in patients with significant blunt cardiac injuries."
- Medscape
Pair this with an ECG (not a lab, but ordered alongside) to look for arrhythmias from cardiac contusion.
8. Urinalysis (UA)
Blunt trauma from a motorcycle crash can also injure the kidneys. Hematuria (blood in urine) would prompt further imaging of the abdomen/kidneys.
Summary Table
| Lab | Purpose | Specific Finding You Are Watching For |
|---|---|---|
| CBC | Blood loss, infection baseline | Low Hgb, thrombocytopenia |
| ABG | Respiratory status, guide ventilation | Low PaO2, high PaCO2, wide A-a gradient |
| Lactate | Shock/hypoperfusion | > 2 mmol/L = tissue hypoxia |
| Type & Crossmatch | Prepare for possible transfusion/surgery | - |
| PT/PTT/INR | Coagulation status | Coagulopathy, DIC |
| BMP/Creatinine | Kidney function, electrolytes | Baseline before fluids/meds |
| Troponin | Cardiac contusion (ribs 2-4 are over the heart) | Elevated = myocardial injury |
| Urinalysis | Kidney/bladder injury | Hematuria |
Bottom line: Labs and the chest CT work together. The CT tells you the anatomy (where and how severe the injury is), while the labs - especially the ABG - tell you how badly the body is actually being affected by it, and guide the decisions on oxygen therapy, fluid management, and whether the patient needs mechanical ventilation.
What is contusion
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
What is a Contusion?
A contusion is a bruise - an area of bleeding into tissue caused by blunt force trauma, without breaking the skin open.
"A contusion, or bruise, is an area of hemorrhage into soft tissue due to rupture of blood vessels caused by blunt trauma."
- DiMaio's Forensic Pathology, 3rd ed.
The Basic Mechanism
When a blunt force hits the body (like hitting a motorcycle handlebar or the ground during a crash), it crushes and tears small blood vessels (capillaries, venules, small arteries) inside the tissue. Blood leaks out of those broken vessels and pools in the surrounding tissue. The skin stays intact - there is no open wound.
This leaked blood causes:
- Swelling (edema from the inflammatory response)
- Discoloration (red → purple → green → yellow as the blood breaks down over days)
- Pain and tenderness (from pressure on nerve endings)
Contusions Can Happen in Any Tissue
This is the key concept for this patient - contusions are not just skin-deep bruises you can see. They happen in internal organs too:
| Location | What It's Called | Example |
|---|---|---|
| Skin / muscle | Bruise / contusion | Purple mark after a fall |
| Lung | Pulmonary contusion | Blood floods the air sacs (alveoli) |
| Heart | Myocardial contusion | Heart muscle bruised from chest impact |
| Brain | Cerebral contusion | Brain tissue bruised after head trauma |
| Kidney | Renal contusion | Kidney bruised from flank impact |
Pulmonary Contusion Specifically (This Patient's Diagnosis)
When the impact from the motorcycle crash hit this patient's chest, the force was transmitted through the rib cage directly into the lung tissue. The lung is delicate and filled with tiny blood vessels and air sacs.
The blunt impact causes:
- Rupture of tiny capillaries inside the lung
- Blood floods into the alveoli (air sacs) and interstitial spaces (the walls between air sacs)
- The flooded alveoli cannot exchange oxygen anymore - they are full of blood instead of air
- This creates a physiologic shunt - blood passes through the lung without picking up oxygen
- Result: Hypoxemia (low blood oxygen) and potentially respiratory failure
"Pulmonary contusion results in tissue damage and hemorrhage into the alveolar and interstitial spaces. Mortality and morbidity are predominantly a result of respiratory failure from ARDS or pneumonia."
- Sabiston Textbook of Surgery
What It Looks Like
On the skin - this is what an external contusion (bruise) looks like:

On CT scan - the left lung (right side of the image, marked by the arrow) appears dense/white because it is filled with blood instead of air. Normal lung is black on CT because it is full of air:

Simple Analogy
Think of the lung like a sponge full of tiny holes (the air sacs). Normally those holes are filled with air. In a pulmonary contusion, the blunt impact bursts blood vessels inside the sponge, and the holes fill up with blood instead of air. The sponge can no longer do its job of absorbing oxygen.
How It Differs from a Laceration
| Contusion | Laceration | |
|---|---|---|
| Skin | Intact (no open wound) | Skin is cut/torn open |
| Mechanism | Blunt force | Sharp force or extreme tearing |
| Internal organ | Bruising + bleeding within tissue | Actual tearing/cutting of organ |
| Example | Pulmonary contusion | Lung laceration (tear in lung tissue) |
In this patient's case, the rib fractures from the motorcycle crash delivered enough blunt force to bruise the lung tissue directly underneath - that is the pulmonary contusion in his admission diagnosis.
What is the findings in xray for this contusion
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete breakdown of what pulmonary contusion looks like on chest X-ray, with real textbook images.
Chest X-Ray Findings in Pulmonary Contusion
The Key Findings
On a plain chest X-ray, pulmonary contusion appears as:
| Finding | What It Means |
|---|---|
| Patchy opacification / haziness | Blood and fluid filling the air sacs |
| Ground-glass opacity | Early/mild contusion - hazy whitening, lung structure still visible through it |
| Consolidation | More severe - dense white area where lung is solidly blood-filled |
| Non-segmental distribution | Does NOT follow lung segment boundaries (unlike pneumonia) |
| Crosses pleural fissures | Distinguishes contusion from atelectasis and pneumonia |
| Peripheral / subpleural location | Usually under the point of impact, near the chest wall |
"Chest radiograph and CT may show patchy, ground-glass opacities in mild or moderate contusion and widespread consolidation in severe contusion. Contusions are found in non-segmental areas of the lung and across pleural fissures."
- Tintinalli's Emergency Medicine
Real X-Ray Images
Image 1 - Before and After (Motor Vehicle Collision, left lung contusion):
- Panel A (left) = on arrival at ER: white hazy area on the left lung (arrow) = pulmonary contusion
- Panel B (right) = 24 hours later: significant improvement as blood is reabsorbed
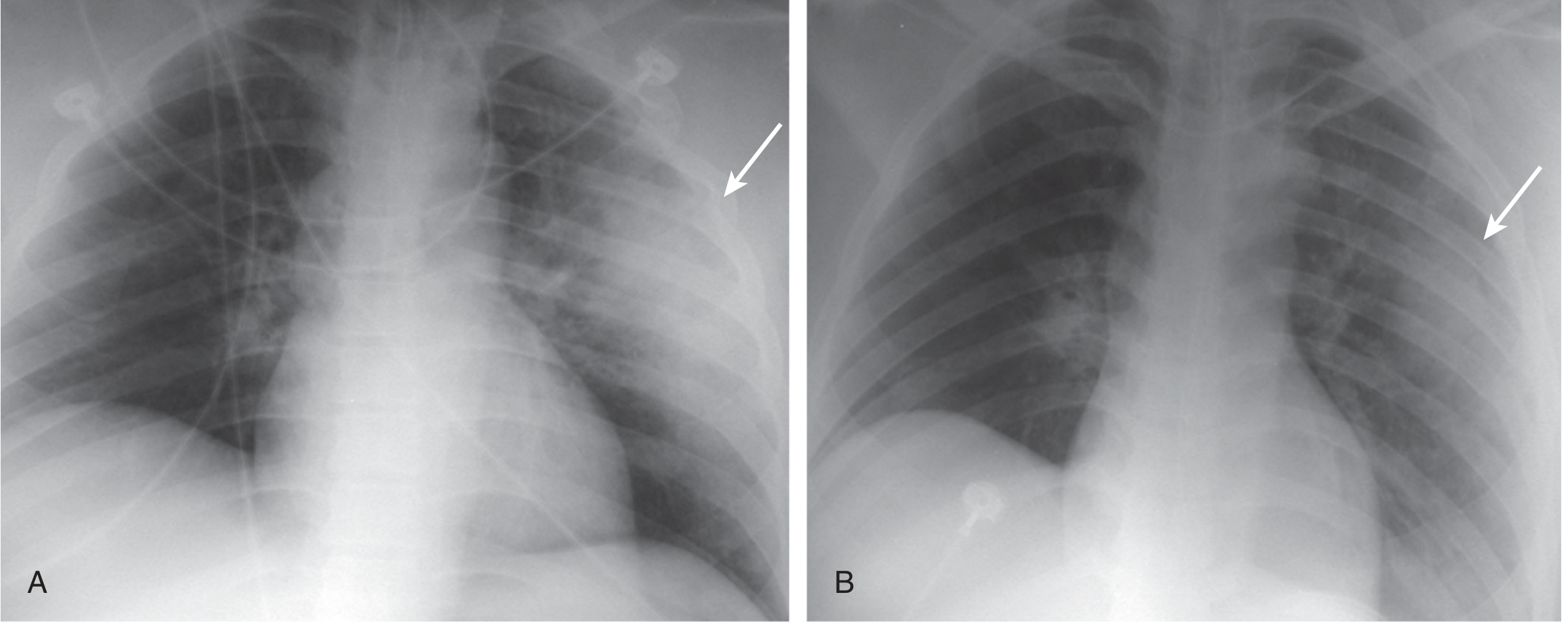
Image 2 - Severe bilateral pulmonary contusion (ICU patient):
Patchy, irregular white areas scattered through both lungs. This is a more advanced/severe case where both lungs are involved.
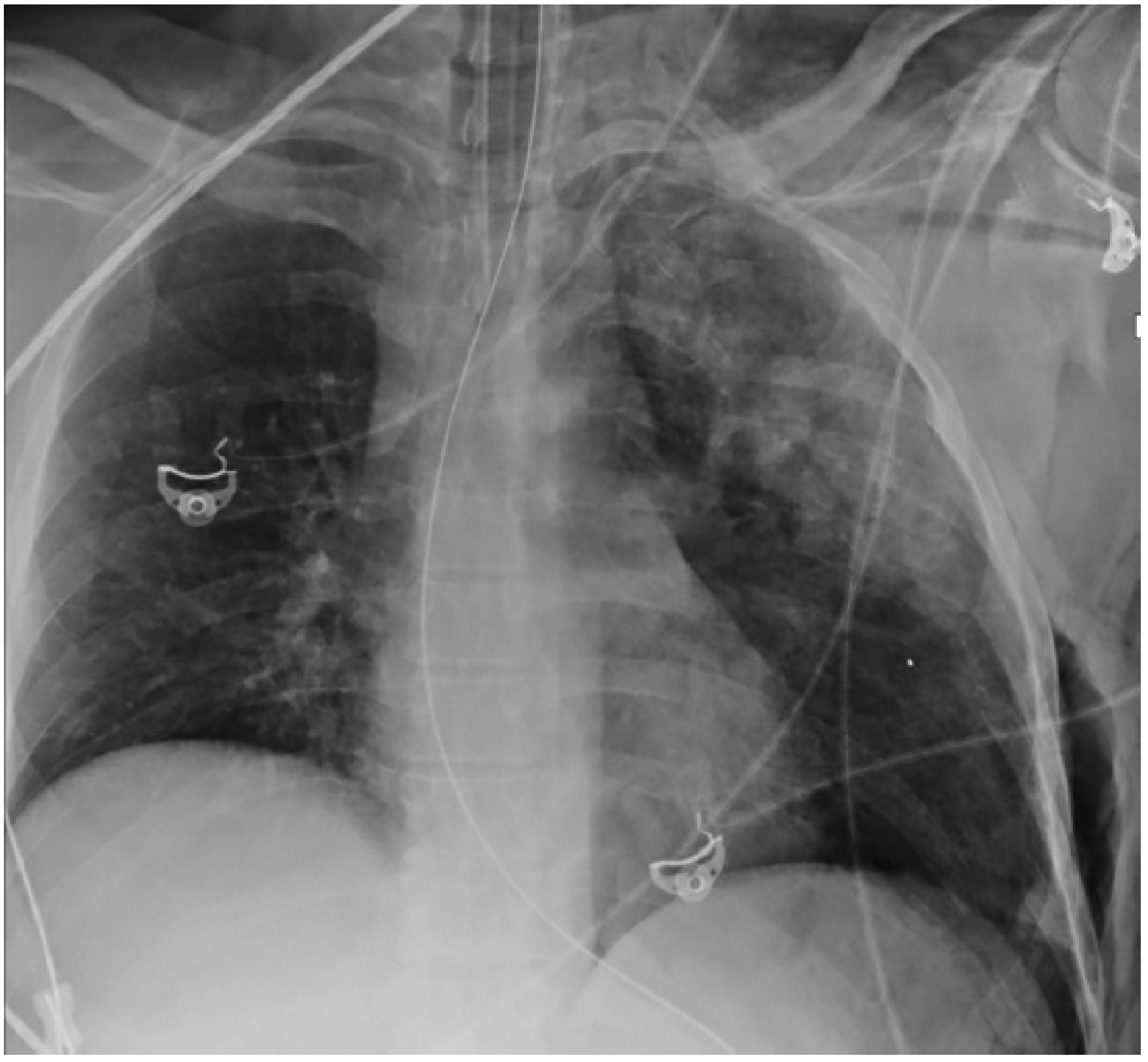
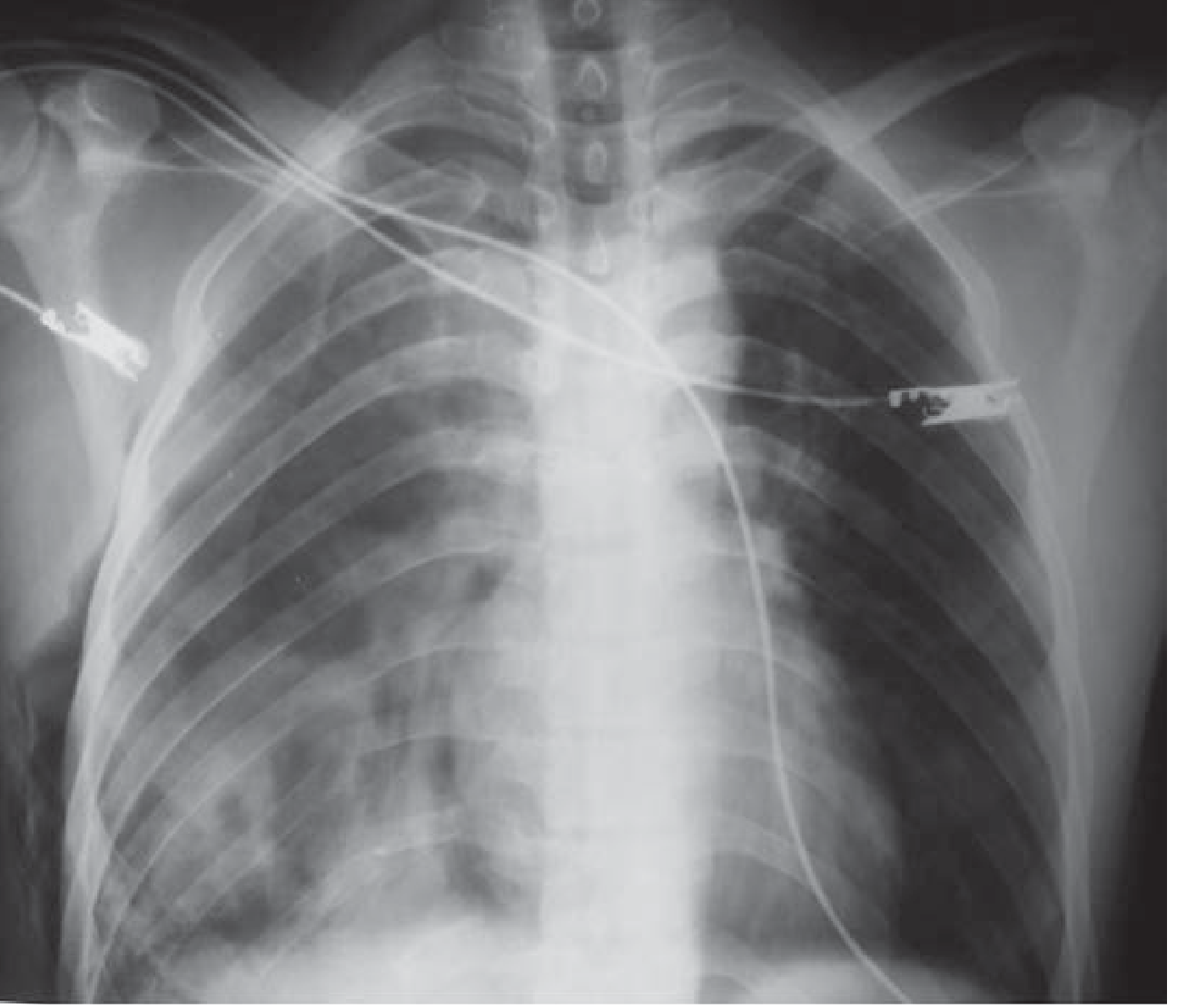
Image 3 - Pulmonary contusion with rib fractures (blunt chest trauma):
Right-sided opacification from a contusion after blunt trauma, with rib fractures visible.
Critical Timing Problem - Why X-ray Alone Is Not Enough
This is the most important clinical point for your patient:
"Radiographic evidence of pulmonary contusion can take 6 hours to be evident, and may not be present until 48 hours post-injury. As many as 70% of pulmonary contusions are NOT visible on the initial radiograph."
- Tintinalli's Emergency Medicine; Rockwood & Green's
Timeline of X-ray changes:
| Time After Injury | What X-ray Shows |
|---|---|
| 0-6 hours | Often NORMAL - even with significant contusion |
| 6-24 hours | Patchy haziness / ground-glass begins to appear |
| 24-48 hours | Findings peak - most obvious on X-ray |
| 48-72 hours | Begins to clear (if no complications) |
| 10 days | Usually resolved (unless pneumonia/ARDS develops) |
This is exactly why the doctor ordered a CT scan for this patient instead of relying on X-ray alone - the patient was admitted in the early hours (1:30 AM, just hours after the crash), and the X-ray could easily look almost normal while significant lung bruising is already present inside.
How to Tell Pulmonary Contusion Apart from Other White Areas on X-ray
| Condition | Timing | Distribution | Clue |
|---|---|---|---|
| Pulmonary contusion | Within minutes to 6 hrs | Non-segmental, crosses fissures, peripheral | Right after trauma |
| Pneumonia | 12-24+ hrs | Segmental (follows lobe/segment) | Fever, productive cough |
| Aspiration | 12-24 hrs | Dependent zones (lower lobes) | History of vomiting/unconsciousness |
| Fat embolism | 12-72 hrs | Bilateral, diffuse | Seen with long bone fractures |
| ARDS | 24-72 hrs | Bilateral, diffuse | After systemic insult |
"Areas of lung opacification on chest imaging within 6 hours of blunt trauma are usually considered diagnostic of pulmonary contusion."
- Tintinalli's Emergency Medicine

photo-1784209672363.jpg
This is the result of xray then why we requesting plain chest ct for this
analyse_media
This is a great clinical question - and the X-ray actually gives us the exact reasons why CT is still needed. Let me break it down clearly.
What the X-Ray Shows (Follow-up, Jul 16, 2026)
The radiology report tells us:
- Regression of pulmonary contusive changes in the right lung - the contusion is improving, but it was there
- No pneumothorax - good
- Heart and aorta normal
- Diaphragm and costophrenic sulci intact
- Fractures with NO significant interval change:
- Right 3rd, 4th, and 5th posterior rib fractures
- Complete oblique fracture in the distal 3rd segment of the right clavicle
- Comminuted fracture of the right scapula
So Why Is CT Still Being Requested?
Even with this X-ray in hand, CT is needed for 5 solid reasons:
1. The X-Ray Confirmed Contusion Was There - CT Tells How Much Lung Is Damaged
The X-ray says the contusion is "regressing" - but it does not tell the doctor:
- How much lung volume was/is involved (mild <18%? moderate 18-28%? severe >28%?)
- Whether there are deeper areas of contusion not visible on X-ray
- Whether the "regression" is real healing or just fluid redistributing
CT quantifies the injury. The treatment approach - oxygen only vs. BiPAP vs. intubation - depends on severity that only CT can measure accurately.
2. Comminuted Scapula Fracture = High-Energy Trauma Warning
A comminuted fracture (broken into multiple fragments) of the scapula is a red flag. The scapula is one of the hardest bones in the body to break because it is protected by surrounding muscles. A comminuted fracture means the impact force was extreme.
High-energy trauma sufficient to shatter the scapula can injure structures that X-ray cannot see:
- Brachial plexus (nerve bundle to the arm)
- Subclavian/axillary vessels (major blood vessels)
- Thoracic outlet structures
- Deeper lung injury not visible on X-ray
CT evaluates all of these in one scan.
3. Right Clavicle Complete Oblique Fracture - Vascular Risk
A complete oblique fracture of the clavicle carries risk of injuring the subclavian artery and vein running directly beneath it. A plain X-ray shows the bone but cannot show if the vessel is compressed, stretched, or torn.
CT (and if needed CT angiography) is the only way to rule this out safely.
4. Posterior Rib Fractures 3rd-5th - More Injuries May Be Hidden
The X-ray now shows fractures at the 3rd, 4th, and 5th posterior ribs - note the admission diagnosis said 2nd, 3rd, 4th. The X-ray has now found more fractures than were initially diagnosed. This is exactly the pattern textbooks warn about:
"A CT scan will identify multiple-level fractures and associated pulmonary injury, such as pneumothorax or hemothorax, with much greater accuracy than additional chest X-ray views."
- Rosen's Emergency Medicine
If 3 fractures showed up on follow-up X-ray that weren't fully counted initially, the question is: are there more? CT gives a definitive 3D picture of every rib, every fragment, and every associated injury.
5. X-Ray Cannot Exclude Hidden Hemothorax or Developing Complications
The X-ray says costophrenic sulci are intact (no obvious fluid pooling at the lung bases), but:
- A small to moderate hemothorax (blood in the chest cavity) can be missed on an AP sitting X-ray
- Early pneumonia developing inside a contused lung looks similar to residual contusion
- Pneumatocele (air-filled cavity forming inside a contused lung) is missed on X-ray
- Damage to the thoracic duct, esophagus, or diaphragm is invisible on X-ray
CT catches all of these.
Summary - X-Ray vs. CT for This Patient
| What X-Ray Told Us | What X-Ray CANNOT Tell Us |
|---|---|
| Contusion is regressing | How much lung is still damaged |
| No visible pneumothorax | Small/occult pneumothorax |
| 3 rib fractures, clavicle, scapula | Fragment displacement, nerve/vessel injury near fractures |
| No obvious pleural fluid | Small hemothorax hiding behind the ribs |
| Aorta looks normal | Subtle aortic/subclavian vessel injury |
The bottom line: The X-ray is a good screening tool and shows things are not getting dramatically worse - but it is like looking at an injury from a distance in poor lighting. The CT is like looking at it up close under full light. Given the severity of this patient's fractures (comminuted scapula + clavicle + 3 ribs), the doctor is right to get CT. The X-ray showing improvement is reassuring, but it does not replace the detailed assessment only CT provides.
This is a shared conversation. Sign in to Orris to start your own chat.