Classify Hodgkin's Lymphoma**, Mixed Cellularity type - two important features; Classify Lymphoma, Types of Hodgkin's Lymphoma - describe in short; Describe a Reed Sternberg Cell and its variants; Gross, Microscopic Features (Pg. 348) 2. Splenomegaly* - list associated diseases; Classification (Pg. 367) 3. Classify Non-Hodgkin's Lymphoma refer robbins answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs exam Add histo pathology diagram and gross as well for exam easy to draw diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the needed material. Let me compile the comprehensive MUHS exam-oriented answer.
PATHOLOGY NOTES - MUHS 2nd MBBS
Based on Robbins & Kumar Basic Pathology + Harshmohan
1. HODGKIN'S LYMPHOMA (HL)
Classification - Five Subtypes (WHO)
HL is classified as:
A. Classic Hodgkin Lymphoma (4 subtypes) - all express CD15 + CD30:
| Subtype | Frequency | Age/Sex | Key Features |
|---|---|---|---|
| 1. Nodular Sclerosis | Most common (~65%) | Young adults, F=M | Lacunar cells + collagen bands; mediastinal involvement |
| 2. Mixed Cellularity | ~25% | >50 yrs, M>F | Abundant classic RS cells; EBV in 70% |
| 3. Lymphocyte Rich | Uncommon | - | Many lymphocytes, few RS cells |
| 4. Lymphocyte Depleted | Rare | Elderly/HIV | Many RS cells, few lymphocytes; worst prognosis |
B. Nodular Lymphocyte Predominant HL (~5%) - SEPARATE entity; L&H "popcorn cells"; expresses CD20, NOT CD15/CD30.
MIXED CELLULARITY HL - Two Important Features (★★ Exam Favorite)
- Abundant classic Reed-Sternberg cells - Binucleate/multinucleate RS cells are plentiful in a heterogeneous inflammatory background of lymphocytes, eosinophils, plasma cells, and macrophages
- Strong EBV association - EBV is demonstrable in RS cells in up to 70% of cases (highest of all HL subtypes); the integration site is identical in all RS cells, confirming EBV infection precedes clonal transformation
Additional notable features:
- Most common subtype in patients >50 years, with male predominance
- More likely to be disseminated and associated with systemic "B symptoms" compared to nodular sclerosis
- EBV likely contributes to transformation via oncogenic LMP1 protein
REED-STERNBERG (RS) CELL - Description
Classic RS Cell (Diagnostic / "Owl-Eye" Cell)
- Size: Large, 15-45 µm in diameter
- Nucleus: Enormous multilobate nucleus (typically binucleate or bilobed)
- Nucleolus: Exceptionally prominent, large, inclusion-like, acidophilic nucleolus surrounded by a clear halo - classically two nucleoli in mirror-image lobes giving the "owl-eye" appearance
- Cytoplasm: Abundant, slightly eosinophilic
- Immunophenotype: CD15(+), CD30(+), CD45(-), B-cell and T-cell markers (-)
- Origin: Derived from germinal center B cells (proven by identical Ig gene rearrangements in single microdissected RS cells)
Histology - Classic RS cell (Robbins Fig 10.23):
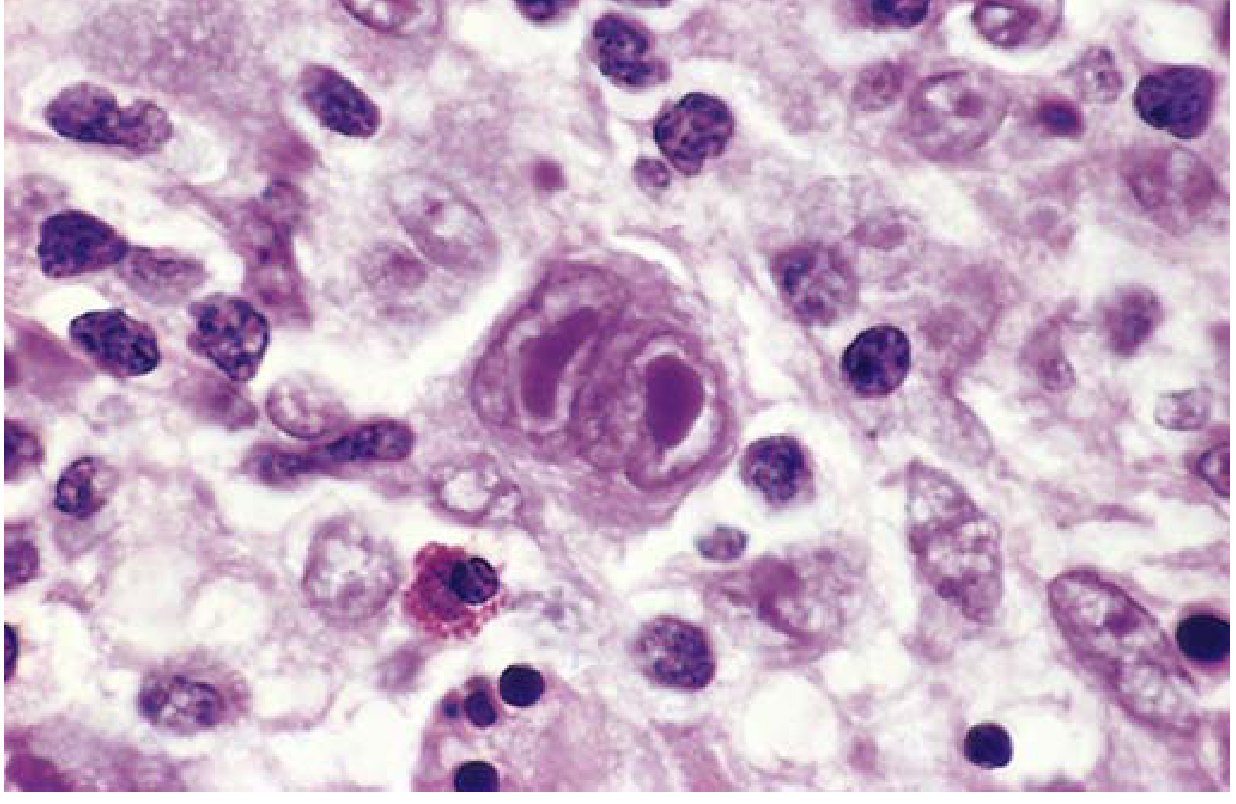
Classic RS cell - binucleate, large inclusion-like nucleoli, "owl-eye" appearance
RS Cell Variants (★★ Must Know for Exam)
| Variant | Subtype found in | Features |
|---|---|---|
| Lacunar cell | Nodular Sclerosis | Single multilobate nucleus, multiple small nucleoli, pale cytoplasm retracts in formalin leaving nucleus in empty "lacune" |
| L&H cell ("Popcorn cell") | Nodular Lymphocyte Predominant | Delicate multilobed nucleus resembling popcorn; expresses CD20, NOT CD15/CD30 |
| Mononuclear variant (Hodgkin cell) | All classic subtypes | Single large nucleus with prominent nucleolus; considered a forme fruste of RS cell |
| Reticular/pleomorphic variant | Lymphocyte Depleted | Bizarre anaplastic multinucleated giant cells |
GROSS AND MICROSCOPIC FEATURES (Pg. 348 reference = Harshmohan equivalent)
Gross Features
- Affected lymph nodes are enlarged, rubbery, matted, and discrete
- In Nodular Sclerosis type: the lymph node is firm due to fibrous bands and may show a white-glistening cut surface
- Involved nodes may coalesce into large masses, particularly in the mediastinum
- Spleen, liver, bone marrow involvement shows irregular nodules of RS cells mixed with reactive cells
Microscopic Features
Key principle: The diagnosis rests on identification of RS cells or variants in the appropriate reactive background.
Nodular Sclerosis (Histology):
- Lacunar cells in cellular nodules
- Collagen bands divide tissue into circumscribed nodules
- Background: lymphocytes, eosinophils, plasma cells
Histology - Nodular Sclerosis, low power (collagen bands dividing tumor into nodules):
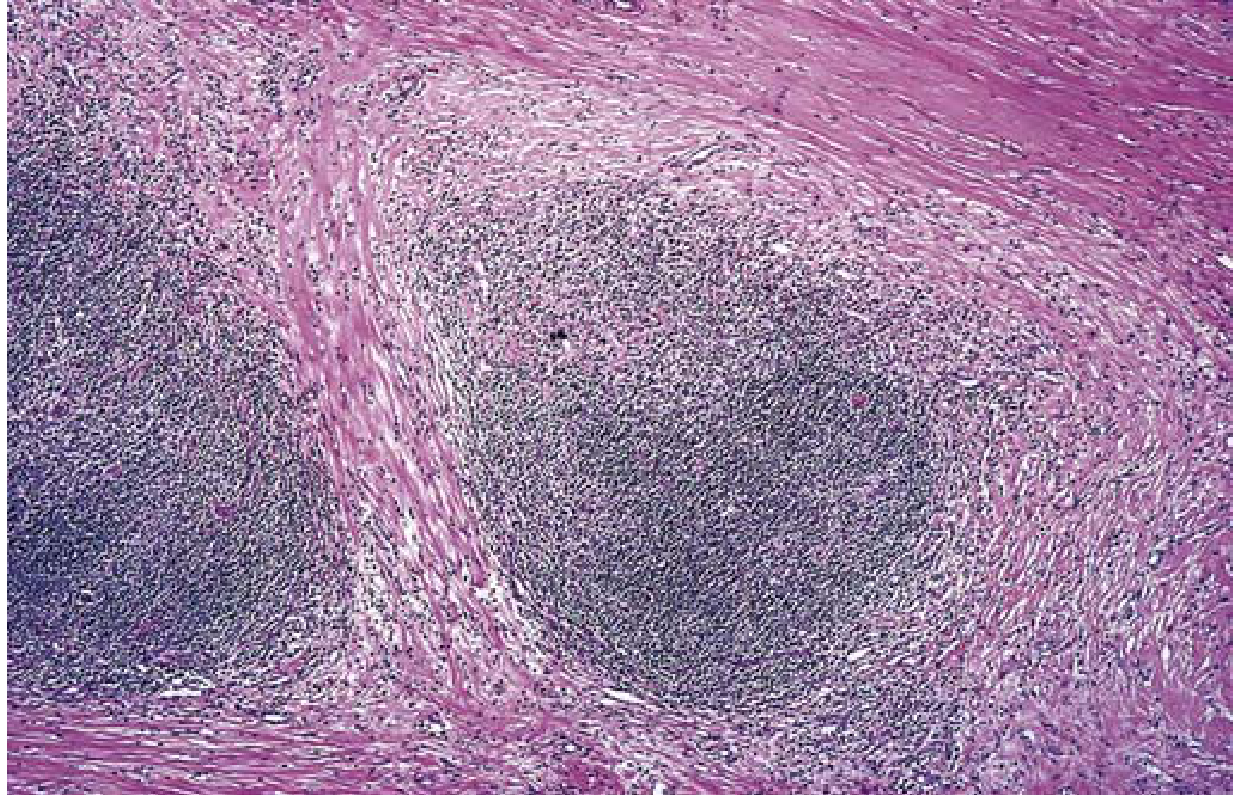
Nodular Sclerosis HL: Pink collagen bands encircling cellular nodules (low power, H&E)
Mixed Cellularity (Histology):
- Classic RS cells plentiful
- Heterogeneous infiltrate: lymphocytes, eosinophils, plasma cells, macrophages
- No collagen bands
Histology - Mixed Cellularity (Robbins Fig 10.26):

Mixed Cellularity HL: Diagnostic binucleate RS cell surrounded by eosinophils, lymphocytes, and histiocytes
Nodular Lymphocyte-Predominant:
- "Popcorn cells" within large nodules of small B cells + macrophages
- Eosinophils scanty/absent; classic RS cells rare
Histology - Nodular LP type:
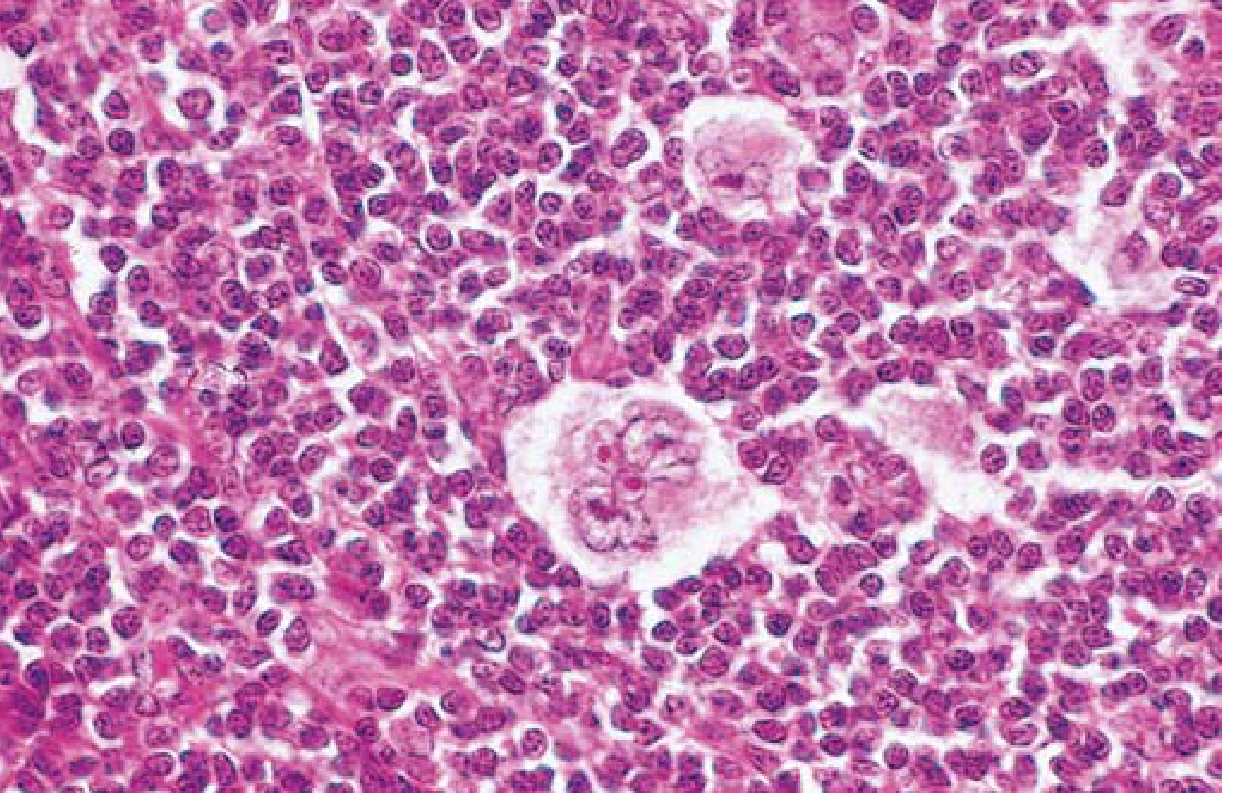
Nodular LP HL: Numerous lymphocytes with scattered large pale "popcorn cells" (L&H variant RS cells)
Pathogenesis (Quick Points)
- RS cells derive from germinal center B cells (proven by identical Ig gene rearrangements)
- EBV encodes LMP1 (a functional mimic of CD40) - most important in mixed cellularity
- RS cells secrete: IL-5 (eosinophil recruitment), TGF-β (fibrosis), IL-13 (autocrine growth)
- RS cells overexpress PD-L1 and PD-L2 → suppress host T-cell response (explains response to anti-PD-1 therapy)
Clinical Features and Staging
Clinical Features:
- Painless lymphadenopathy (most common presentation)
- B symptoms: fever, night sweats, >10% weight loss
- Pruritus
- Spreads in a stepwise/contiguous fashion (unlike NHL)
- Rarely involves mesenteric nodes or Waldeyer's ring
Ann Arbor Staging:
| Stage | Definition |
|---|---|
| I | Single lymph node region |
| II | ≥2 node regions, same side of diaphragm |
| III | Both sides of diaphragm |
| IV | Disseminated - multiple extralymphatic organs |
Add "A" = no B symptoms; "B" = fever, night sweats, weight loss
Prognosis: Overall excellent; 5-year survival ~90% with current chemotherapy (ABVD regimen).
2. SPLENOMEGALY - Classification and Associated Diseases
Definition
The spleen responds to most systemic diseases by enlarging. Splenomegaly produces: discomfort/dragging pain, hypersplenism (anemia, leukopenia, thrombocytopenia - especially thrombocytopenia due to platelet sequestration in red pulp).
Classification with Associated Diseases (Table 10.12, Robbins)
I. INFECTIONS
- Nonspecific splenitis (blood-borne infections, especially infective endocarditis)
- Infectious mononucleosis (EBV) - risk of splenic rupture
- Tuberculosis
- Typhoid fever
- Brucellosis
- Cytomegalovirus (CMV)
- Syphilis
- Malaria (massive splenomegaly/"Tropical splenomegaly")
- Histoplasmosis
- Toxoplasmosis
- Trypanosomiasis
- Schistosomiasis
- Leishmaniasis (kala-azar - massive splenomegaly)
- Echinococcosis
II. CONGESTIVE STATES (related to Portal Hypertension)
- Cirrhosis of the liver (most common cause of massive congestive splenomegaly)
- Portal vein thrombosis
- Splenic vein thrombosis
- Cardiac failure (congestive heart failure)
III. LYMPHOHEMATOGENOUS DISORDERS
- Hodgkin lymphoma
- Non-Hodgkin lymphomas and lymphocytic leukemias
- Myeloproliferative neoplasms (CML, polycythemia vera, primary myelofibrosis - massive splenomegaly)
- Hemolytic anemias (hereditary spherocytosis, thalassemia, sickle cell)
IV. IMMUNOLOGIC / INFLAMMATORY CONDITIONS
- Rheumatoid arthritis (Felty's syndrome: RA + splenomegaly + neutropenia)
- Systemic Lupus Erythematosus (SLE)
V. STORAGE / CONGENITAL (Lipid Storage Diseases)
- Gaucher disease (most common - massive splenomegaly)
- Niemann-Pick disease
- Mucopolysaccharidoses
VI. MISCELLANEOUS
- Amyloidosis
- Primary neoplasms and cysts (hemangioma - most common benign tumor)
- Secondary (metastatic) neoplasms
Quick Memory Aid for Splenomegaly Causes:
"I CAN LIST"
I - Infections (malaria, TB, EBV)
C - Congestive (portal HTN, cirrhosis)
A - Autoimmune (SLE, RA)
N - Neoplasms (lymphomas, leukemias)
L - Lipid storage (Gaucher, NPC)
I - Inflammatory
S - Storage disorders
T - Thalassemia/hemolytic anemias
3. NON-HODGKIN'S LYMPHOMA (NHL) - Detailed
Definition
NHL is a heterogeneous group of malignant lymphomas arising from lymphoid cells at various stages of differentiation (B cells - majority; T cells; rarely NK cells). Unlike HL, they are generally disseminated at diagnosis and spread non-contiguously.
Classification - By Cell of Origin + Grade
WHO Classification Principles:
- Based on cell of origin (B cell vs T cell vs NK cell)
- Stage of differentiation (precursor vs mature/peripheral)
- Growth pattern (follicular vs diffuse)
- Grade (indolent/low grade vs aggressive/high grade)
B-CELL NHLs (most common - ~85% of all NHL)
1. Small Lymphocytic Lymphoma / Chronic Lymphocytic Leukemia (SLL/CLL)
- Most common adult leukemia (CLL)
- Cell type: Mature CD5+ B cells
- Histology: Diffuse effacement of lymph node architecture with proliferation centers (pseudofollicles containing larger prolymphocytes) - pathognomonic
- High BCL2 expression (antiapoptotic)
- Indolent course; immune abnormalities (autoimmune hemolytic anemia, hypogammaglobulinemia)
- ~10% transform to aggressive DLBCL (Richter transformation)
- Key exam: CD5(+), CD23(+), CD20(dim+)
2. Follicular Lymphoma
- Most common indolent lymphoma (~20% of all NHL in adults)
- Cell type: Germinal center B cells
- Key genetic lesion: t(14;18) - juxtaposes BCL2 gene with IgH locus → BCL2 overexpression → blocked apoptosis
- Histology: Back-to-back follicles recapitulating germinal center B-cell growth; follicles are uniform, closely packed, lack polarization; mantle zones thin/absent
- Indolent but incurable with standard therapy
- 30-40% transform to aggressive DLBCL
- Key exam: CD10(+), BCL2(+), BCL6(+)
3. Mantle Cell Lymphoma
- Cell type: Mature CD5+ B cells (like CLL but different)
- Key genetic lesion: t(11;14) → Cyclin D1 overexpression (diagnostic marker)
- Moderately aggressive; poor prognosis
- Involves mantle zone of lymphoid follicles
- Key exam: CD5(+), CD23(-), Cyclin D1(+)
4. Extranodal Marginal Zone Lymphoma (MALT lymphoma)
- Arises at extranodal sites with chronic inflammation: stomach (H. pylori), salivary glands (Sjögren's), thyroid (Hashimoto's), lung
- Mature B cells; expresses CD20 and surface IgM
- Forms lymphoepithelial lesions (tumor cells infiltrate epithelium)
- Eradication of H. pylori causes regression of gastric MALT lymphoma (important exam point)
- Localized, indolent; often cured by excision + radiotherapy
5. Diffuse Large B-Cell Lymphoma (DLBCL)
- Most common type of lymphoma in adults (~35% of adult NHL)
- Aggressive; heterogeneous group
- Key genetic lesions:
- BCL6 rearrangements (3q27) - ~1/3 of cases
- t(14;18) with BCL2 - ~30% (may be "transformed" follicular lymphoma)
- MYC translocations
- Histology: Large cells (3-4x resting lymphocyte), round/oval nuclei, dispersed chromatin, distinct nucleoli, pale cytoplasm; diffuse growth pattern; architectural effacement
- Immunophenotype: CD20(+), CD45(+)
- ~50% cured with aggressive chemotherapy (R-CHOP)
- "Double-hit" lymphoma (BCL2 + MYC rearrangements) = very aggressive
6. Burkitt Lymphoma
- Very aggressive B-cell tumor
- Mostly extranodal (jaw in endemic African form; abdominal in sporadic form)
- Key genetic lesion: t(8;14) - MYC translocation (also t(2;8) or t(8;22)) → MYC overexpression
- EBV strongly associated with endemic (African) form; less so in sporadic
- Histology: "Starry-sky" pattern - sheets of medium-sized uniform blastic cells with numerous mitotic figures + scattered pale macrophages (tangible-body macrophages) giving a starry-sky appearance
- Immunophenotype: CD20(+), CD10(+), BCL6(+), BCL2(-), Ki-67 ~100%
- Potentially curable with intensive chemotherapy
7. Hairy Cell Leukemia (HCL)
- Rare indolent B-cell tumor
- Cells have characteristic "hairy" cytoplasmic extensions
- Massive splenomegaly + cytopenias (characteristic clinical triad)
- BRAF mutation (V600E) - diagnostic; excellent response to BRAF inhibitors and cladribine
- Tartrate-resistant acid phosphatase (TRAP) positive
T-CELL NHLs (~15% of all NHL)
8. Mycosis Fungoides (MF) / Sézary Syndrome (SS)
- Tumor of CD4+ skin-homing T cells
- MF: Indolent, localized skin involvement; responds well to topical therapy
- Histology: Pautrier microabscesses (clusters of atypical T cells in epidermis)
- SS: Leukemic variant with diffuse erythroderma and circulating tumor cells; aggressive
- Key exam: CD4(+), CD7(-) (aberrant T-cell phenotype)
9. Adult T-Cell Leukemia/Lymphoma (ATLL)
- Caused by HTLV-1 retrovirus (only human cancer caused by a retrovirus - ★exam)
- CD4(+) T cells expressing high levels of CD25 (IL-2 receptor α chain)
- Clinical: Skin lesions, lymphadenopathy, hepatosplenomegaly, hypercalcemia (osteoclast activating factors)
- Peripheral blood: cells with markedly irregular nuclear contours ("flower cells")
- Aggressive; median survival ~8 months
10. Peripheral T-Cell Lymphoma (PTCL, NOS)
- Heterogeneous group (~10% adult NHL)
- Lack defining features; "not otherwise specified"
- Aggressive; respond poorly to therapy
- Produce cytokines causing systemic symptoms even at low tumor burden
KEY DIFFERENCES: HL vs NHL (★★ Must Know)
| Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
| Node involvement | Single axial group (cervical, mediastinal, paraaortic) | Multiple node groups |
| Spread | Orderly, contiguous | Non-contiguous |
| Mesenteric nodes | Rarely involved | Commonly involved |
| Waldeyer's ring | Rarely involved | Commonly involved |
| Extranodal involvement | Uncommon | Common |
| Staging at diagnosis | Often early stage | Often disseminated |
| Diagnosis | Requires tissue biopsy (RS cells) | Various subtypes by biopsy + immunophenotype |
| Prognosis | Generally excellent | Varies widely by subtype |
QUICK EXAM SUMMARY TABLE: NHL subtypes
| Lymphoma | Key Marker | Key Genetic Lesion | Grade |
|---|---|---|---|
| CLL/SLL | CD5+, CD23+ | - | Indolent |
| Follicular | CD10+, BCL2+ | t(14;18) | Indolent |
| Mantle cell | CD5+, Cyclin D1+ | t(11;14) | Moderate |
| MALT | CD20+ | H. pylori assoc. | Indolent |
| DLBCL | CD20+ | BCL6, BCL2, MYC | Aggressive |
| Burkitt | CD10+, Ki-67~100% | t(8;14) MYC | Very aggressive |
| Hairy cell | TRAP+, BRAF V600E | BRAF | Indolent |
| ATLL | CD25+ CD4+ | HTLV-1 retrovirus | Aggressive |
| Mycosis fungoides | CD4+, CD7- | - | Indolent |
Easy Diagrams to Draw in Exam
1. Reed-Sternberg Cell (draw this for any HL question)
___________
/ \
| O[nucleolus]| <-- Nucleus 1 with large eosinophilic nucleolus
| (halo) | surrounded by clear halo
\___________/
|
| "Owl-eye"
_____|_____
/ \
| O[nucleolus]| <-- Mirror-image Nucleus 2
| (halo) |
\___________/
Abundant eosinophilic cytoplasm all around
Background: lymphocytes + eosinophils + plasma cells
2. Nodular Sclerosis HL (draw for microscopy question)
|===Collagen band===|===Collagen band===|===Collagen band===|
| | | |
| [Lacunar cell] | [Lacunar cell] | [Lacunar cell] |
| lymphocytes | lymphocytes | lymphocytes |
| eosinophils | eosinophils | eosinophils |
| Nodule 1 | Nodule 2 | Nodule 3 |
|___________________|___________________|___________________|
3. Burkitt "Starry-Sky" Pattern (draw for NHL question)
●●●●●●●●●●●●●●●●●●●● (dark tumor cells = the "night sky")
●●● ☆ ●●●●●●● ☆ ●●● (pale macrophages = "stars")
●●●●●●●● ☆ ●●●●●●●●
●● ☆ ●●●●●●●●● ☆ ●●
●●●●●●●●●●●●●●●●●●●●
Pathogenesis Summary - B-cell NHL oncogene table
| Lymphoma | Translocation | Activated gene | Mechanism |
|---|---|---|---|
| Follicular | t(14;18) | BCL2 | Anti-apoptosis |
| Mantle cell | t(11;14) | Cyclin D1 | Promotes cell cycle |
| Burkitt | t(8;14) | MYC | Transcription factor, proliferation |
| DLBCL | t(3;27) | BCL6 | Transcriptional repressor |
Sources: Robbins & Kumar Basic Pathology (10th ed.), Robbins Cotran Pathologic Basis of Disease; correlation with Harshmohan Textbook of Pathology topics for MUHS 2nd MBBS exam.
This is a shared conversation. Sign in to Orris to start your own chat.