Pediatrics Advanced life support in exam oriented pattern for emergency physician
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive data. Let me compile the full exam-oriented PALS guide:
Pediatric Advanced Life Support (PALS) - Exam-Oriented Review for Emergency Physicians
Sources: Rosen's Emergency Medicine (9e), Tintinalli's Emergency Medicine (9e)
1. EPIDEMIOLOGY & KEY CONCEPTS (High-Yield)
| Feature | Pediatric (vs Adult) |
|---|---|
| Arrest etiology | Respiratory predominates (hypoxia/asphyxia), NOT primary cardiac |
| VF/pVT incidence | ~10-15% (vs ~85% in adults) |
| Bystander CPR | Improves survival but underperformed |
| Survival (out-of-hospital) | ~10%; in-hospital ~30-40% |
| Primary goal | Oxygenation + ventilation FIRST, then perfusion |
Exam pearl: Because children arrest from respiratory causes, they benefit from conventional CPR (compressions + ventilations), unlike adults where compression-only CPR is acceptable. Compression-only CPR is inferior in pediatric arrests from asphyxia.
2. AGE DEFINITIONS (PALS)
| Term | Age Range |
|---|---|
| Neonate | Birth to 28 days |
| Infant | <1 year |
| Child | 1 year to puberty |
| Adult ACLS | Signs of puberty onward |
3. RECOGNIZING ARREST / PRE-ARREST
Pediatric Assessment Triangle (PAT)
- Appearance (TICLS: Tone, Interactiveness, Consolability, Look/Gaze, Speech/Cry)
- Work of Breathing
- Circulation to skin (color, mottling, pallor)
Normal Vital Signs by Age
| Age | HR (beats/min) | RR (breaths/min) | SBP (mmHg) |
|---|---|---|---|
| Newborn | 100-160 | 30-60 | 60-90 |
| Infant (1-12 mo) | 100-160 | 25-50 | 70-100 |
| Toddler (1-3 y) | 90-150 | 20-30 | 80-110 |
| Preschool (3-5 y) | 80-140 | 20-25 | 80-110 |
| School-age (6-12 y) | 70-120 | 15-20 | 90-120 |
| Adolescent | 60-100 | 12-20 | 100-120 |
Hypotension by age (PALS formula): Systolic BP < 70 + (2 × age in years) for ages 1-10
4. CPR - HIGH-QUALITY COMPRESSIONS
Key Parameters
| Parameter | Value |
|---|---|
| Rate | 100-120/min |
| Depth - Infants | 1.5 inches (≥1/3 AP diameter) |
| Depth - Children | 2 inches (≥1/3 AP diameter) |
| Recoil | Complete chest recoil |
| Interruptions | Minimize; switch compressor every 2 minutes |
| C:V ratio (no airway) | 15:2 (pediatric; 30:2 for adults) |
| C:V ratio (advanced airway) | Continuous compressions + 1 breath every 2-3 sec (20-30 breaths/min) |
Compression Technique by Age
| Age | Technique |
|---|---|
| Infant (1-rescuer) | 2-finger technique on sternum below nipple line |
| Infant (2-rescuer) | 2-thumb encircling technique - preferred (generates higher cardiac output) |
| Child 1-8 years | 1 or 2 hands, heel of hand on lower half sternum |
| Older child/adolescent | 2 hands, same as adult |
Exam pearl: For infants, the 2-thumb encircling technique generates greater cardiac output and coronary perfusion pressure than the 2-finger technique. Use it when a second rescuer is available.
ETCO₂ in CPR
- Target ETCO₂ >20 mmHg to indicate adequate compressions
- Sudden rise in ETCO₂ signals ROSC
- If ETCO₂ consistently <10 mmHg despite optimal CPR, prognosis is poor
5. AIRWAY & VENTILATION
BVM vs Endotracheal Intubation
- For pre-hospital arrest: 2019 PALS update recommends bag-mask ventilation - ETI does not improve survival and may worsen outcomes (delays compressions; OR 0.82 for survival, no benefit)
- For in-hospital arrest: insufficient evidence to mandate ETI over BVM
- If ETI performed: aim for 8-10 breaths/min without interrupting compressions
Airway Sizes (Exam Classics)
- ET tube size = (Age/4) + 4 (uncuffed) or (Age/4) + 3.5 (cuffed)
- Preferred: cuffed ETT in all ages (avoids multiple attempts)
- Verify placement with waveform capnography
Jaw Thrust vs Head-Tilt/Chin-Lift
- Jaw thrust preferred if cervical spine injury suspected
- Head-tilt/chin-lift is standard for non-trauma
6. VASCULAR ACCESS
Priority order:
- Peripheral IV (2 attempts max - 90 seconds)
- Intraosseous (IO) - if IV fails; should be obtained within 60-90 seconds of arrest
- Central venous access
IO sites:
- Proximal tibia (most common)
- Distal tibia
- Distal femur
- Humeral head (EZ-IO)
Exam pearl: IO is equivalent to IV for drug delivery in arrest. All resuscitation drugs can be given IO. If epinephrine is given via ETT: dose is 10× the IV dose (0.1 mg/kg of 1:1000).
7. PALS CARDIAC ARREST ALGORITHM (2020 AHA)
AHA 2020 Pediatric Cardiac Arrest Algorithm
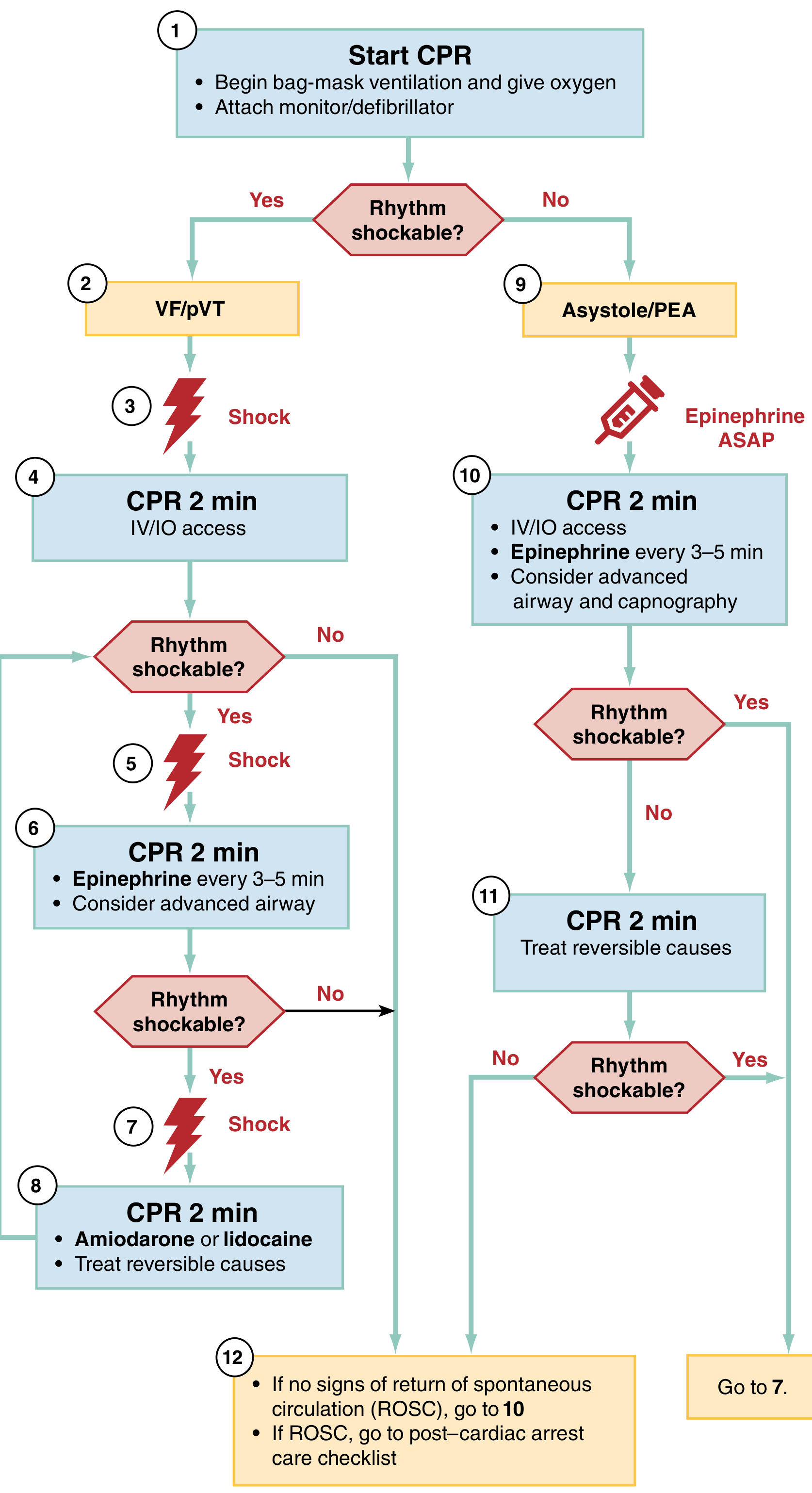
The algorithm splits into two arms based on rhythm:
Shockable (VF / pulseless VT)
- Start CPR + O₂ + attach monitor
- Shock: 2 J/kg
- CPR 2 min + IV/IO access
- Shock: 4 J/kg
- CPR 2 min + Epinephrine every 3-5 min
- Shock: ≥4 J/kg (max 10 J/kg or adult dose)
- CPR 2 min + Amiodarone or Lidocaine + treat reversible causes
- Continue loops; check rhythm every 2 min
Non-Shockable (Asystole / PEA)
- Start CPR + O₂
- CPR 2 min + IV/IO access + Epinephrine ASAP (repeat every 3-5 min)
- Consider advanced airway
- Treat reversible causes (H's and T's)
- Check rhythm every 2 min; if converts to shockable → go to shockable arm
8. DRUG THERAPY IN ARREST
Medications for Pediatric Cardiac Arrest
| Drug | Indication | IV/IO Dose | Key Notes |
|---|---|---|---|
| Epinephrine | All rhythms | 0.01 mg/kg (0.1 mL/kg of 0.1 mg/mL); max 1 mg | Repeat every 3-5 min; ET dose 0.1 mg/kg; HIGH doses (>0.01) do NOT improve survival |
| Amiodarone | VF/pVT, SVT | 5 mg/kg bolus; up to 3 doses for VF/pVT | May repeat x3 for refractory VF; infuse over 20-60 min for SVT |
| Lidocaine | VF/pVT | 1 mg/kg loading dose | Alternative to amiodarone; avoid in WPW |
| Atropine | Bradycardia (vagal/AV block) | 0.02 mg/kg; min 0.1 mg, max 0.5 mg/dose | NOT for routine use in PEA/asystole |
| Adenosine | SVT | 0.1 mg/kg (1st dose, max 6 mg); 0.2 mg/kg (2nd, max 12 mg) | 1st-line for stable SVT; rapid IV push + flush; avoid in WPW/wide QRS |
| Procainamide | SVT (WPW), stable VT | 10-15 mg/kg over 30-60 min | 1st line for SVT in WPW; do NOT combine with amiodarone |
| Calcium chloride | Hyperkalemia, hypocalcemia, CCB OD | 20 mg/kg | Not routine; central line preferred |
| Sodium bicarbonate | Hyperkalemia, TCA overdose | 1 mEq/kg | Not routine use |
| Magnesium sulfate | Torsades de pointes | Max single dose 2 g | Not routine |
| Dextrose | Hypoglycemia | 0.5-1 g/kg (max 25 g) | D10W: 5 mL/kg; D25W: 2 mL/kg; D50W: 1 mL/kg; Do NOT give empirically |
Exam pearl: Epinephrine dose via ETT is 10× IV dose = 0.1 mg/kg of 1 mg/mL (1:1000) concentration. IV/IO dose uses 0.1 mg/mL (1:10,000) concentration.
9. H's AND T's - REVERSIBLE CAUSES
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary) |
| Hypoglycemia | Thrombosis (coronary) |
| Hypothermia |
Pediatric-specific emphasis: Hypoxia and hypovolemia are the most common reversible causes in children.
10. PEDIATRIC BRADYCARDIA ALGORITHM
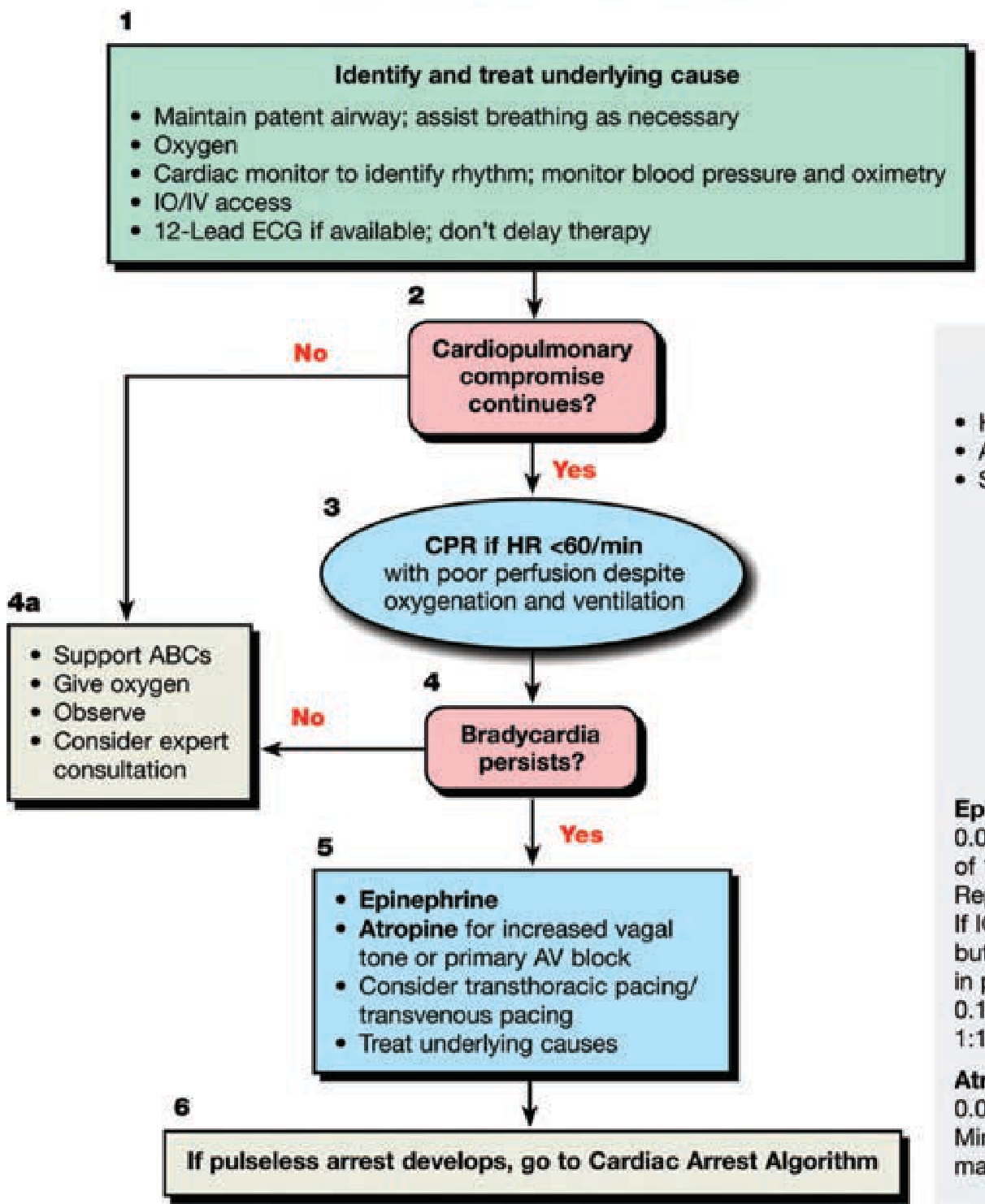
Key steps:
- Identify and treat underlying cause (O₂, airway, IO/IV access)
- Is there cardiopulmonary compromise? (hypotension, AMS, shock)
- No → support ABCs, observe
- Yes → If HR <60/min with poor perfusion despite O₂/ventilation → CPR
- If bradycardia persists:
- Epinephrine 0.01 mg/kg IV/IO (repeat every 3-5 min); or
- Atropine 0.02 mg/kg (for increased vagal tone or primary AV block); min 0.1 mg, max 0.5 mg
- Consider transcutaneous pacing
- If pulseless arrest develops → Cardiac Arrest Algorithm
Exam pearl: In pediatrics, bradycardia is most commonly due to hypoxia - treat the airway first. Atropine is for vagal causes/AV block, NOT hypoxic bradycardia.
11. PEDIATRIC TACHYCARDIA ALGORITHM
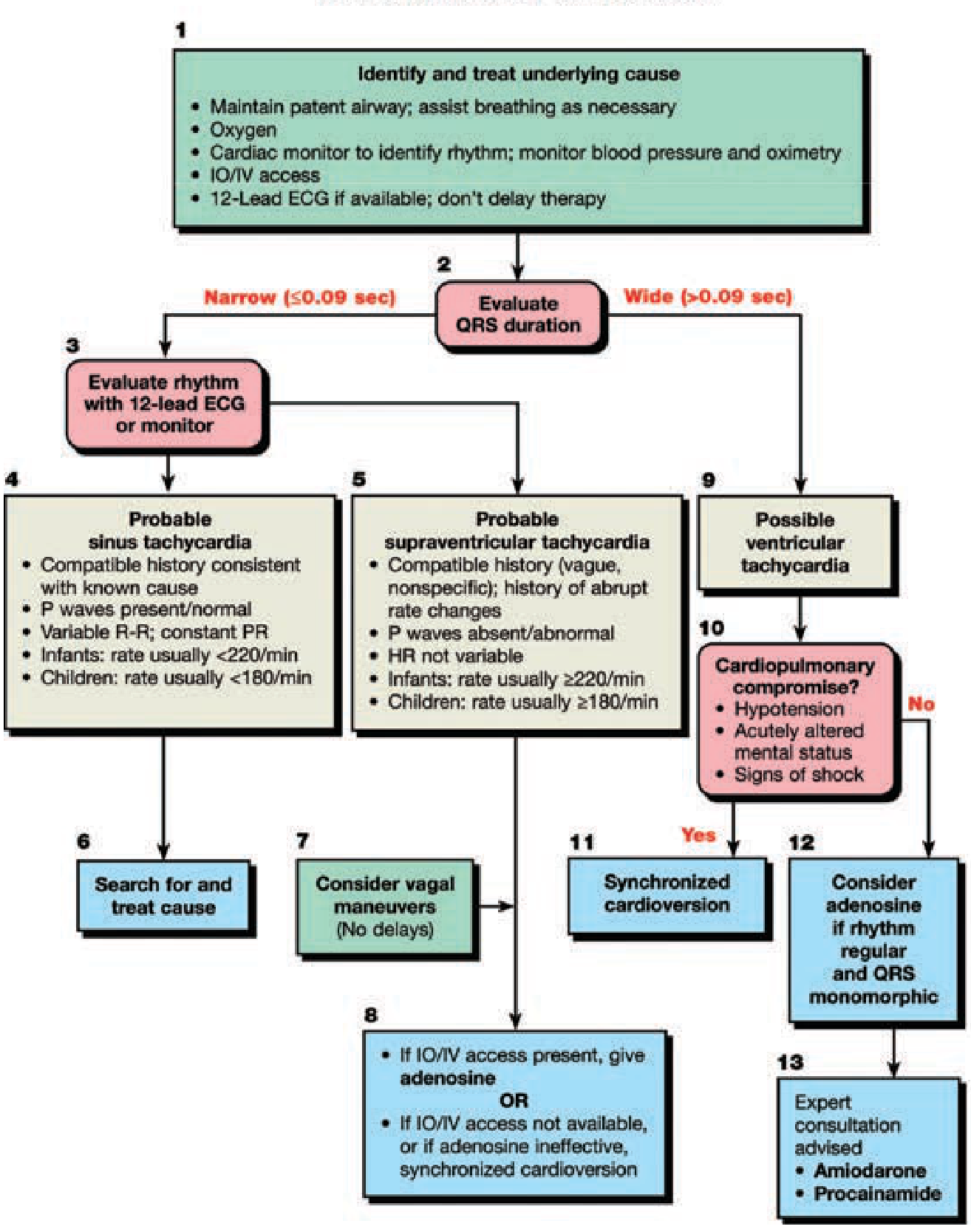
Step 1: Evaluate QRS Duration
- Narrow QRS (≤0.09 sec)
- Wide QRS (>0.09 sec)
Step 2: Sinus Tachycardia vs SVT (Narrow Complex)
| Feature | Sinus Tachycardia | SVT |
|---|---|---|
| History | Compatible with known cause (fever, pain, hypovolemia) | Vague, abrupt onset |
| P waves | Present/normal | Absent or abnormal |
| R-R interval | Variable | Fixed (non-variable HR) |
| Rate - Infants | Usually <220/min | Usually ≥220/min |
| Rate - Children | Usually <180/min | Usually ≥180/min |
| Treatment | Treat underlying cause | Vagal maneuvers → Adenosine → Cardioversion |
SVT Treatment (Narrow Complex)
- Vagal maneuvers (ice water to face in infants; Valsalva in older children) - first-line, no delays
- Adenosine 0.1 mg/kg rapid IV bolus (max 6 mg); if ineffective → 0.2 mg/kg (max 12 mg)
- Synchronized cardioversion 0.5-1 J/kg; if ineffective → 2 J/kg (sedate if possible, do NOT delay)
Wide Complex Tachycardia
- Possible VT - evaluate for cardiopulmonary compromise
- With compromise → Synchronized cardioversion
- Without compromise + regular + monomorphic QRS → consider adenosine; consult expert; consider amiodarone or procainamide
Exam pearl - WPW: Avoid adenosine, digoxin, beta-blockers, calcium channel blockers in WPW. Use procainamide (first-line for SVT in WPW) or cardioversion.
12. DEFIBRILLATION & CARDIOVERSION
| Intervention | Energy | Notes |
|---|---|---|
| Defibrillation (VF/pVT) | 1st: 2 J/kg; 2nd: 4 J/kg; subsequent: ≥4 J/kg (max 10 J/kg or adult dose) | Unsynchronized |
| Synchronized cardioversion (SVT/unstable VT) | 0.5-1 J/kg; repeat at 2 J/kg | Synchronize mode ON |
| AED for children <8 years / <25 kg | Prefer AED with pediatric dose attenuator | Use adult AED if no pediatric attenuator available |
| AED for children ≥8 years / >25 kg | Standard adult AED |
Pad/Paddle placement:
- One contact: right of sternum at 2nd intercostal space
- Other contact: left midclavicular line at xiphoid level
13. POST-CARDIAC ARREST CARE (ROSC)
| Goal | Target |
|---|---|
| Oxygenation | SpO₂ 94-99%; avoid hyperoxia (FiO₂ titration) |
| Ventilation | PaCO₂ 35-45 mmHg; avoid hypocapnia |
| Hemodynamics | MAP ≥5th percentile for age; treat hypotension aggressively |
| Glucose | Normoglycemia; treat hypo- AND hyperglycemia |
| Temperature | Targeted Temperature Management (TTM): 32-36°C; avoid fever |
| 12-lead ECG | Obtain immediately to identify ST-elevation MI or arrhythmia |
| Neurological monitoring | EEG (especially if unresponsive post-arrest) |
Exam pearl: Post-ROSC hypotension and hyperoxia are independently associated with worse neurological outcomes and mortality.
14. PEDIATRIC SEPTIC SHOCK
Recognition
- Tachycardia + signs of decreased perfusion (delayed cap refill >2s, mottling, altered mental status)
- Hypotension is a LATE sign in children (maintained by compensatory tachycardia/vasoconstriction)
- "Compensated shock" = shock WITHOUT hypotension - critical to recognize
Management (Golden Hour Bundle)
- 0-15 min: Obtain IV/IO access; labs (CBC, BMP, lactate, blood culture, glucose); IV/IO fluid bolus
- Fluid resuscitation: 10-20 mL/kg NS or LR bolus; titrate to signs of perfusion; reassess after each bolus
- Antibiotics: Broad-spectrum IV within 1 hour of recognition
- Vasopressors (if fluid-unresponsive): Norepinephrine or epinephrine for fluid-refractory shock
- Hydrocortisone: for catecholamine-refractory shock with suspected adrenal insufficiency
Exam pearl: The 2020 Surviving Sepsis Campaign moved AWAY from mandating aggressive fluid resuscitation (no longer 3×20 mL/kg). Reassess after each bolus and stop if signs of fluid overload (crackles, hepatomegaly, worsening O₂).
15. TERMINATION OF RESUSCITATION
- Pediatric CPA lasting >20 minutes without ROSC is associated with poor outcome
- Exception: Hypothermic arrest - continue until rewarmed ("not dead until warm and dead")
- If hypothermia is responsible and cardiac electrical activity is present, continue resuscitation
QUICK REFERENCE: PALS DOSE SUMMARY CARD
| Drug | Dose | Route | Max |
|---|---|---|---|
| Epinephrine (arrest) | 0.01 mg/kg | IV/IO q3-5 min | 1 mg |
| Epinephrine (ETT) | 0.1 mg/kg | ETT | - |
| Amiodarone (arrest) | 5 mg/kg bolus (×3) | IV/IO | - |
| Lidocaine | 1 mg/kg | IV/IO | - |
| Atropine | 0.02 mg/kg | IV/IO | 0.5 mg |
| Adenosine 1st | 0.1 mg/kg | IV rapid | 6 mg |
| Adenosine 2nd | 0.2 mg/kg | IV rapid | 12 mg |
| Cardioversion | 0.5-1 J/kg → 2 J/kg | Synchronized | - |
| Defibrillation | 2 → 4 → ≥4 J/kg | Unsynchronized | 10 J/kg |
| Glucose (D10W) | 5 mL/kg | IV/IO | 25 g |
| Ca chloride | 20 mg/kg | IV/IO | - |
| NaHCO₃ | 1 mEq/kg | IV/IO | - |
| MgSO₄ | 25-50 mg/kg | IV/IO | 2 g |
TOP 10 PALS EXAM TRAPS
- C:V ratio = 15:2 (pediatric single/2-rescuer without advanced airway) - NOT 30:2
- Minimum atropine dose = 0.1 mg - doses <0.1 mg can cause paradoxical bradycardia
- ETT epinephrine dose = 0.1 mg/kg (10× the IV dose)
- First defibrillation = 2 J/kg, not 1 or 3 J/kg
- Bradycardia + hypoxia in children - treat airway FIRST before medications
- CPR starts at HR <60/min with poor perfusion, not just HR <60
- Adenosine is ineffective or potentially harmful in WPW - use procainamide
- Compression-only CPR is inferior in pediatric asphyxial arrest
- Hypotension is a LATE sign of shock in children
- Hypothermia = continue resuscitation regardless of duration
Sources: Rosen's Emergency Medicine 9e, Ch. 158; Tintinalli's Emergency Medicine 9e, Ch. 109 - AHA 2020 PALS Guidelines
Stroke syndrome complete guide from Harrison, tintinaali and Rosen's emergency book
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here's a summary of what's covered in this complete guide:
What's Covered (18 Sections)
The guide integrates content from Rosen's Emergency Medicine 9e (Ch. 87), Tintinalli's Emergency Medicine 9e, and Harrison's Principles of Internal Medicine 22e, organized in exam-focused format:
- Epidemiology - stroke types and frequencies
- Pathophysiology - CBF thresholds, penumbra, ICH injury mechanisms
- Anatomy of stroke syndromes - anterior/posterior circulation, lacunar syndromes with full tables (including Wallenberg, locked-in, ACA/MCA/PCA territories)
- TIA - tissue-based definition, ABCD² score, risk stratification
- Hemorrhagic stroke - ICH sites and frequencies, clinical presentations, ICH Score
- Stroke recognition scales - FAST, LAPSS, Cincinnati, full NIHSS with scoring
- Imaging - CT findings (hyperdense MCA, insular ribbon, etc.), CT with actual case images, CTA, CTP, DWI-FLAIR mismatch
- Time goals - NINDS door-to-needle targets
- IV thrombolysis - alteplase vs tenecteplase, time windows, full inclusion/exclusion criteria, sICH management
- BP management - separate targets for ischemic/pre-tPA/post-tPA/ICH
- Mechanical thrombectomy - LVO criteria, DAWN/DEFUSE3 extended windows
- ICH management - anticoagulation reversal, surgical indications, ICP management
- SAH - Hunt-Hess grade, diagnosis, nimodipine
- Stroke mimics - 10+ conditions with differentiating features
- CT findings table
- Secondary prevention - antiplatelet, anticoagulation, statins, carotid surgery
- Drug doses quick reference card
- Top 12 exam traps
This is a shared conversation. Sign in to Orris to start your own chat.