Explain plasma cell neoplasms
Reading File
Finding Sources
Finding Sources
Searching PubMed
"plasma cell neoplasms" OR "multiple myeloma"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have extensive content from Robbins Pathology, Goldman-Cecil Medicine, and Harrison's. Let me compile a comprehensive, well-structured answer.
Plasma Cell Neoplasms
Plasma cell neoplasms are a group of clonal disorders arising from terminally differentiated B lymphocytes (plasma cells) that secrete a monoclonal immunoglobulin protein, called the M protein (or paraprotein). They span a spectrum from premalignant to overtly malignant conditions, with multiple myeloma being the most common and clinically significant.
Classification and Spectrum
The major entities, arranged from least to most aggressive, are:
| Entity | Key Feature |
|---|---|
| MGUS | M protein <3 g/dL, <10% marrow plasma cells, no end-organ damage |
| Smoldering Multiple Myeloma | M protein ≥3 g/dL or 10-60% marrow plasma cells, no end-organ damage |
| Multiple Myeloma | ≥10% clonal plasma cells + myeloma-defining events |
| Solitary Plasmacytoma | Single mass of clonal plasma cells (bone or extramedullary) |
| Plasma Cell Leukemia | Circulating plasma cells; terminal / aggressive variant |
| Lymphoplasmacytic Lymphoma / Waldenstrom's | B-cell neoplasm with plasmacytic differentiation; monoclonal IgM |
1. Monoclonal Gammopathy of Undetermined Significance (MGUS)
Definition
MGUS is a premalignant clonal plasma cell disorder defined by:
- Serum M protein <3 g/dL
- <10% clonal plasma cells in bone marrow
- No myeloma-defining events (no anemia, renal failure, hypercalcemia, lytic bone lesions)
Epidemiology
- Prevalence increases with age: ~1% in persons aged 50-60; >5% in those over 70 years
- More common in males; prevalence in Black Americans is twice that in Whites
- Familial clustering is recognized
Pathogenesis
- About 40% of MGUS shows IgH translocations involving chromosome 14q32 (partners include CCND1 at 11q13, FGFR3/MMSET at 4p16.3, and others)
- Another ~40% show hyperdiploid trisomies of odd-numbered chromosomes
- Normal plasma cells coexist with the clonal cells on flow cytometry
Risk of Progression
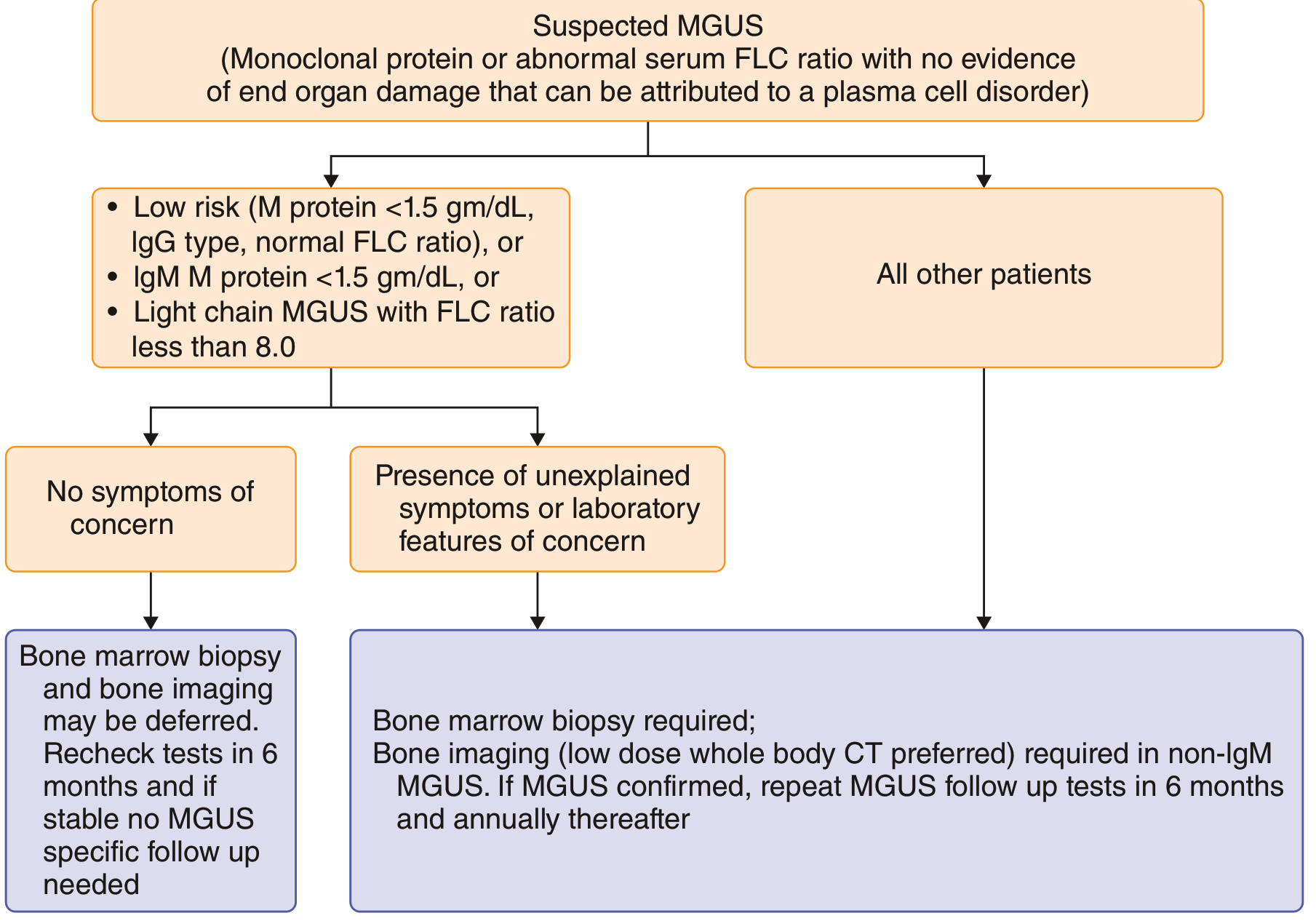
MGUS progresses to myeloma or a related disorder at a fixed rate of ~1% per year. Risk stratification uses three factors: M protein level, Ig subtype, and free light chain (FLC) ratio:
| Risk Group | 20-Year Absolute Progression Risk |
|---|---|
| Low (M protein <1.5 g/dL, IgG, normal FLC ratio) | ~5% |
| Low-intermediate (1 factor abnormal) | ~21% |
| High-intermediate (2 factors abnormal) | ~37% |
| High (all 3 factors abnormal) | ~58% |
- IgM MGUS tends to progress to Waldenstrom macroglobulinemia
- Non-IgM and light chain MGUS tend to progress to multiple myeloma
- All forms carry risk of progression to AL amyloidosis
Diagnostic Approach
2. Multiple Myeloma
Definition
Multiple myeloma is a malignancy of plasma cells defined by:
- ≥10% clonal plasma cells on bone marrow biopsy
- M protein in serum or urine (except in nonsecretory myeloma)
- At least one myeloma-defining event (CRAB criteria or specific biomarkers)
CRAB Criteria (myeloma-defining events):
- C - Hypercalcemia (>11 mg/dL)
- R - Renal insufficiency (creatinine >2 mg/dL or CrCl <40 mL/min)
- A - Anemia (Hb <10 g/dL or >2 g/dL below normal)
- B - Bone lesions (≥1 lytic lesion on imaging)
Additional biomarkers that define myeloma even without CRAB: >60% clonal plasma cells, serum FLC ratio ≥100, or >1 focal lesion on MRI.
Epidemiology
- ~1% of all malignancies; ~10% of hematologic malignancies in the US
- ~30,000 new cases/year in the US; incidence ~4 per 100,000
- Median age at diagnosis: 65-70 years; only 2% are under 40
- Males slightly more affected; incidence in Black Americans ~twice that in Whites
Pathogenesis
Genetic events:
- Virtually all cases evolve from a preceding MGUS phase
- Primary events: IgH translocations (40%) at chromosome 14q32 involving partners such as CCND1 (11q13), FGFR3/MMSET (4p16.3), c-MAF (16q23); or trisomies (hyperdiploid, 40%)
- Disease progression involves secondary events: RAS mutations, MYC abnormalities, deletion 17p, deletion 1p, and amplification 1q
Bone destruction mechanism:
- Myeloma cells upregulate RANKL expression on stromal cells and decrease osteoprotegerin (OPG)
- The elevated RANKL/OPG ratio activates osteoclasts - pure osteolytic disease
- Additional osteoclast activators: MIP-1α, IL-3, IL-1β, IL-6
- Osteoblast suppression by IL-3, IL-7, and DKK1
- Net result: pathologic fractures, hypercalcemia
IL-6 is the dominant plasma cell growth factor, produced by marrow stromal cells; it supports myeloma cell proliferation and survival.
M Protein Types
- IgG: 52-60% (most common)
- IgA: 20-25%
- Light chain only (Bence Jones protein): 16-20%
- IgD: 2%
- Biclonal: 2%
- Nonsecretory: ~1-3%
Morphology
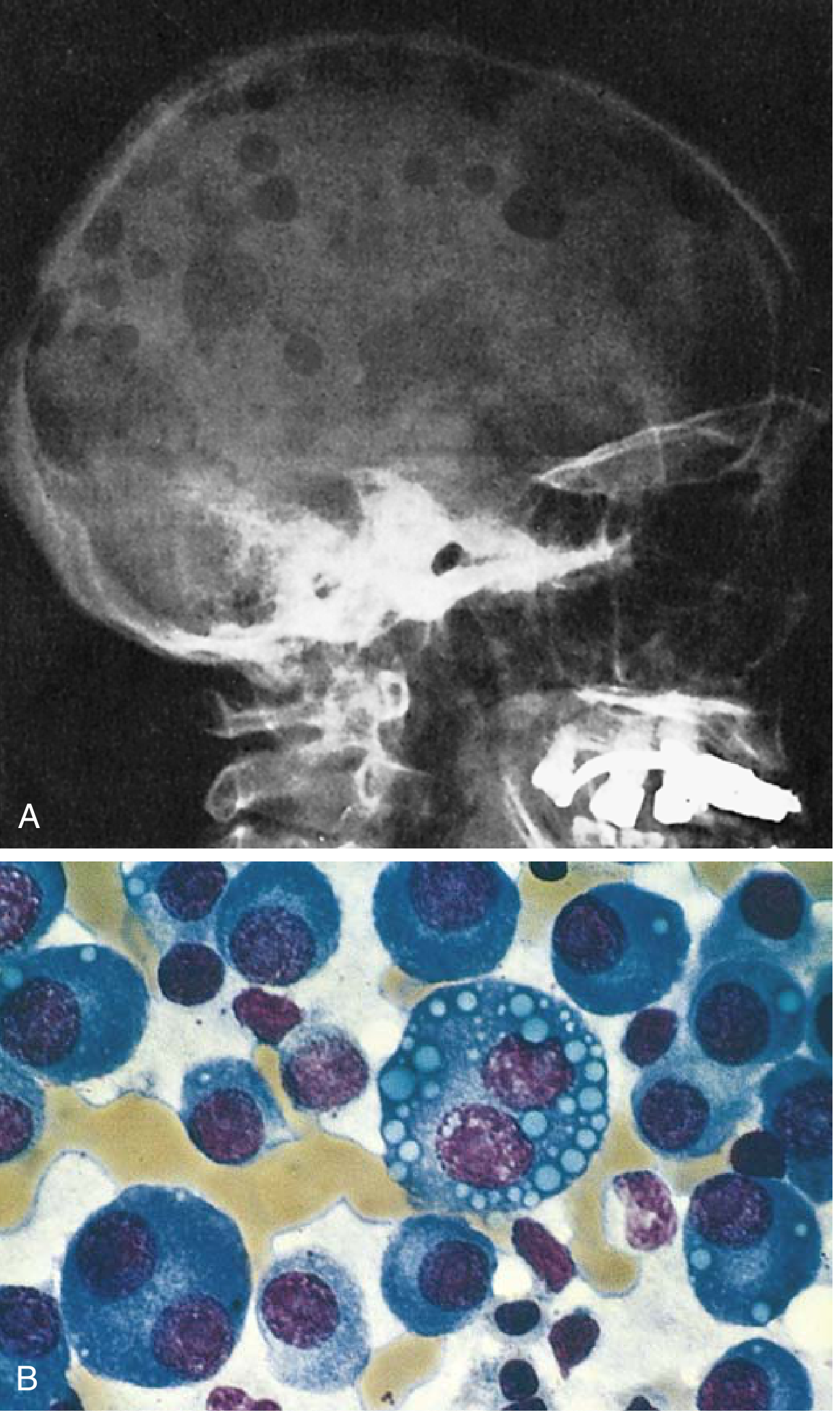
- Bone lesions: multifocal, typically in vertebral column, ribs, skull, pelvis, femur
- Marrow: plasma cells >30% of cellularity; abnormal features include prominent nucleoli, Russell bodies, multinucleation
- Myeloma kidney: proteinaceous casts of Bence Jones protein in distal tubules and collecting ducts, surrounded by multinucleate giant cells; tubular epithelial necrosis
Clinical Manifestations
Skeletal: Bone pain (especially back/chest) in >67% at diagnosis; vertebral collapse with height loss; pathologic fractures
Anemia: Normocytic/normochromic anemia in ~75% at diagnosis (marrow replacement, renal failure, inflammation)
Renal dysfunction: Occurs in up to 50% of patients - from:
- Cast nephropathy (Bence Jones proteins blocking tubules)
- Light chain deposition (glomerular or interstitial)
- AL amyloidosis
- Hypercalcemia (dehydration, nephrocalcinosis)
- Recurrent pyelonephritis (from hypogammaglobulinemia)
Infections: Increased risk of bacterial infections from suppressed normal immunoglobulin production (despite elevated total immunoglobulin from M protein) and neutropenia
Hypercalcemia: Confusion, weakness, lethargy, polyuria, constipation
Hyperviscosity (less common than in Waldenstrom's): Visual disturbances, headache
Amyloidosis (AL type): From light chain deposition - can cause cardiomyopathy, macroglossia, peripheral neuropathy, nephrotic syndrome
Thrombosis: Deep vein thrombosis - risk heightened by both disease and some treatments (e.g., lenalidomide)
Laboratory Findings
- Serum protein electrophoresis (SPEP): M protein spike in 80%; with serum immunofixation, detected in 93%
- Urine protein electrophoresis: Free light chains (Bence Jones protein); combined serum + urine detects M protein in 97%
- Serum free light chain assay: Can replace urine studies; key for monitoring
- β2-microglobulin and albumin: Used in staging
- LDH: Elevated in high-risk disease
- CBC: Normocytic anemia; sometimes leukopenia and thrombocytopenia
- Bone marrow biopsy: ≥10% clonal plasma cells required for diagnosis
- Imaging: Whole-body low-dose CT (preferred); MRI for spinal cord compression; PET-CT for staging
Staging (Revised ISS)
| Stage | Criteria | Median OS |
|---|---|---|
| I | Albumin ≥3.5 g/dL, β2-microglobulin <3.5 mg/L, no high-risk cytogenetics, normal LDH | ~62 months |
| II | Neither Stage I nor III | ~44 months |
| III | β2-microglobulin >5.5 mg/L + either high-risk cytogenetics OR elevated LDH | ~29 months |
High-risk cytogenetics: t(4;14), t(14;16), t(14;20), del(17p), amp(1q), p53 mutation
Standard-risk: t(11;14), t(6;14), trisomies
Treatment
Transplant-eligible patients:
- Induction therapy: triplet regimen (e.g., bortezomib + lenalidomide + dexamethasone, "VRd")
- Followed by autologous hematopoietic stem cell transplantation (ASCT) - remains standard of care
- Maintenance therapy: lenalidomide post-transplant prolongs progression-free survival
Transplant-ineligible patients:
- VRd or daratumumab-based regimens (Dara-VRd or Dara-Rd)
- Continuous therapy until progression
Mechanism targets:
- Proteasome inhibitors (bortezomib, carfilzomib, ixazomib): Myeloma cells accumulate misfolded immunoglobulin chains and are uniquely sensitive to proteasome blockade
- Immunomodulatory drugs (IMiDs) (thalidomide, lenalidomide, pomalidomide): Anti-angiogenic, immunostimulatory, direct anti-tumor effects
- Anti-CD38 monoclonal antibodies (daratumumab, isatuximab): Target CD38 expressed on plasma cells
- Anti-BCMA therapies: CAR-T cells (idecabtagene vicleucel, ciltacabtagene autoleucel) and bispecific antibodies for relapsed/refractory disease
Supportive care:
- Bisphosphonates (zoledronic acid) or denosumab for bone disease
- Plasmapheresis for hyperviscosity
- IVIG for recurrent infections
- Prophylactic anticoagulation with IMiD-based regimens
- Erythropoiesis-stimulating agents for anemia
Prognosis: Median survival approximately 5 years overall; has improved substantially with modern regimens. Smoldering myeloma may not require treatment for years.
3. Solitary Plasmacytoma
- A single mass of clonal plasma cells, either in bone (osseous plasmacytoma) or soft tissue (extramedullary plasmacytoma)
- No marrow infiltration elsewhere and no CRAB criteria
- Treatment: local radiotherapy
- ~50-70% of osseous plasmacytomas progress to multiple myeloma within 10 years; extramedullary has a lower progression rate
4. Lymphoplasmacytic Lymphoma / Waldenstrom Macroglobulinemia
Definition
A B-cell neoplasm of older adults where tumor cells undergo partial plasmacytic differentiation, secreting monoclonal IgM. When IgM is present in amounts sufficient to cause hyperviscosity, the clinical syndrome is called Waldenstrom macroglobulinemia.
Pathogenesis
- Virtually all cases carry a MYD88 L265P activating mutation, which drives NF-κB signaling - a key diagnostic and therapeutic target
- Unlike myeloma: no bone destruction, free light chain complications (renal failure, amyloidosis) are rare
Morphology and Immunophenotype
- Marrow infiltrate of lymphocytes, plasma cells, and plasmacytoid lymphocytes + mast cell hyperplasia
- Russell bodies (cytoplasmic) and Dutcher bodies (nuclear) containing Ig
- Spreads to lymph nodes, spleen, liver; rarely, nerve roots/meninges
- CD20+ B-cell markers + monoclonal surface IgM
Clinical Features
- Nonspecific: weakness, fatigue, weight loss
- ~50%: lymphadenopathy, hepatosplenomegaly
- Anemia from marrow infiltration
- ~10%: cold agglutinin-mediated autoimmune hemolysis (IgM antibodies active at <37°C)
Hyperviscosity syndrome (from high-concentration IgM):
- Visual impairment: tortuous/dilated retinal veins, retinal hemorrhages
- Neurologic: headaches, dizziness, deafness, stupor
- Bleeding: complexes between macroglobulins and clotting factors; platelet coating
- Raynaud phenomenon and cold urticaria from cryoglobulins
Treatment
- Rituximab-based regimens (anti-CD20)
- Ibrutinib (BTK inhibitor) - particularly effective given MYD88 pathway dependence
- Bendamustine + rituximab
- Plasmapheresis for acute hyperviscosity
5. Key Comparisons at a Glance
| Feature | Multiple Myeloma | Waldenstrom's | MGUS |
|---|---|---|---|
| Cell type | Plasma cells | Lymphocytes + plasma cells | Clonal plasma cells |
| M protein | IgG/IgA/light chain | IgM | Any, low level |
| Bone lesions | Yes (lytic) | No | No |
| Hyperviscosity | Rare | Common | No |
| Renal failure | Common | Rare | No |
| Bone marrow | ≥10% plasma cells | Mixed infiltrate | <10% plasma cells |
| Key mutation | IgH translocations, RAS, MYC | MYD88 L265P | IgH translocations or trisomies |
Recent Evidence (PubMed)
Recent meta-analyses (2024-2025) have focused on novel immunotherapies in relapsed/refractory myeloma:
- A 2024 meta-analysis (PMID 39551604) compared CAR T-cell therapy vs. bispecific antibodies as third-line or later treatment, showing both modalities produce deep responses
- Systematic reviews on CAR T-cell safety identified non-relapse mortality risks (PMID 38977912) and secondary malignancy rates (PMID 39256908)
These findings do not contradict established pathophysiology or first-line treatment approaches, but underscore a shift toward immunotherapy-based salvage in relapsed disease.
Sources: Robbins & Kumar Basic Pathology, p. 421-423 | Goldman-Cecil Medicine, Ch. 173 | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.