31 yr old male with central chest pain felt like heaviness, occured twice today, last for few seconds, yesterday did high intensity cardio, no palpitations, no breathlessness, no radiation of pain, no sweating, no nausea or vomiting. He said the paon went away when he massaged
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a structured clinical analysis of this presentation:
Clinical Assessment: 31-year-old Male with Central Chest Heaviness
Presenting Features - Summary
| Feature | Detail |
|---|---|
| Age/Sex | 31-year-old male |
| Pain character | Heaviness, central chest |
| Duration | Few seconds each episode |
| Frequency | Twice today |
| Preceding event | High-intensity cardio yesterday |
| Relieving factor | Massage |
| Associated symptoms | None - no palpitations, no breathlessness, no radiation, no diaphoresis, no nausea/vomiting |
Differential Diagnosis
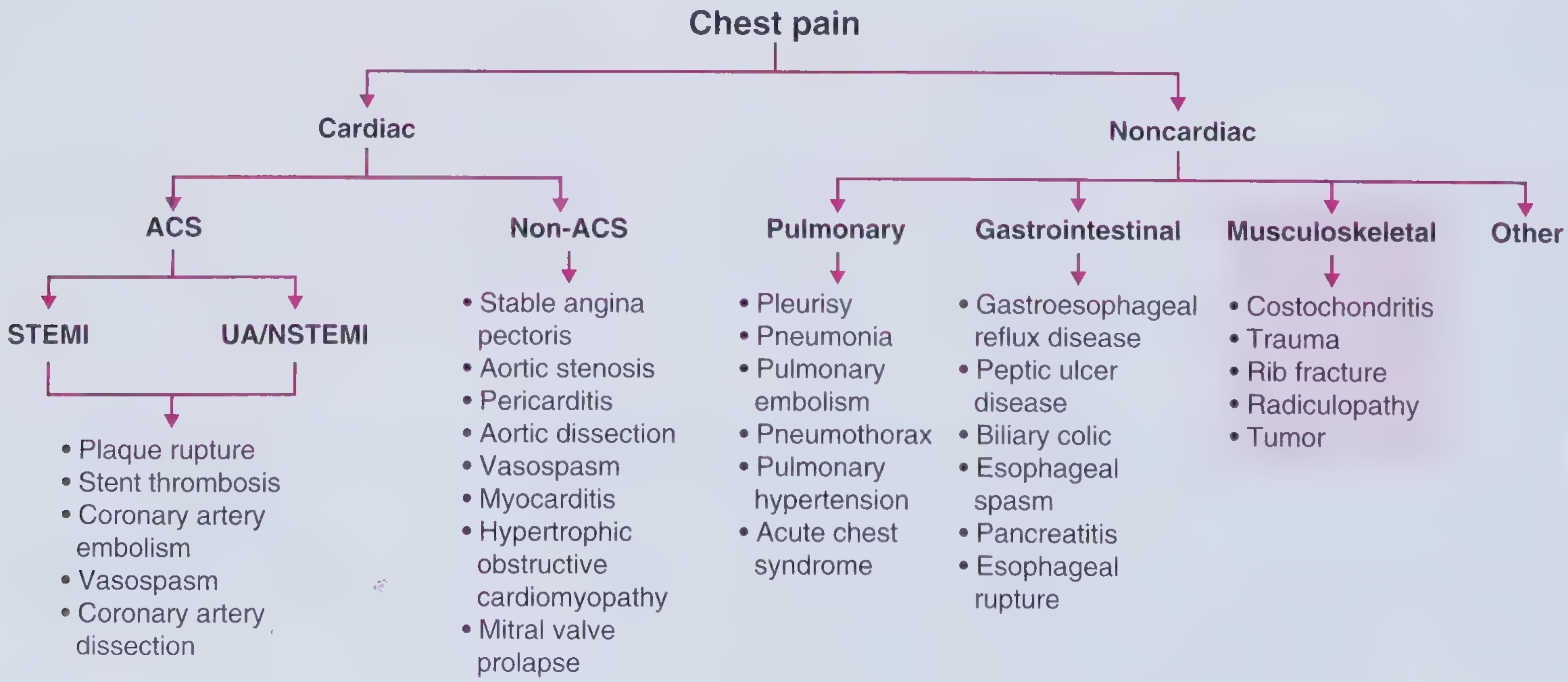
- Frameworks for Internal Medicine
1. Most Likely: Musculoskeletal Chest Pain (Costochondritis / Chest Wall Strain)
This is the most probable diagnosis given:
- Prior high-intensity cardio - exercise is a recognized precipitant of chest wall pain. Murray & Nadel's notes: "pain related to breathing may be experienced along the costal margins after vigorous exercise"
- Relief with massage - this is the key distinguishing feature. Pain that responds to massage/palpation points strongly toward a musculoskeletal rather than cardiac origin
- Tenderness to palpation is a hallmark of costochondritis and chest wall strain, helping differentiate these from angina
- Very brief duration (seconds) - cardiac ischemic pain typically lasts minutes, not seconds
- No autonomic features - complete absence of diaphoresis, nausea, or radiation argues against ischemia
With costochondritis, pain arises from costochondral cartilaginous junctions and is described as "dull with a gnawing, aching quality." The most common sites are the 2nd, 3rd, and 4th costal cartilages. - Murray & Nadel's Textbook of Respiratory Medicine
Chest wall muscle strain from intense cardio (particularly exercises involving chest/pec muscles - push-ups, bench press, rowing) can produce very similar localized chest wall pain.
2. Must Exclude: Cardiac Causes (Low Probability Here, but Important)
Even though this presentation is not typical for ischemia, cardiac causes must be considered because the symptom is central chest heaviness. In a 31-year-old male:
| Cardiac Cause | Why Less Likely in This Case |
|---|---|
| Stable angina / NSTE-ACS | No risk factors mentioned; pain lasts seconds (not 5-30 min); no radiation, no diaphoresis, no dyspnea; relieves with massage |
| Hypertrophic obstructive cardiomyopathy (HOCM) | Should be considered in young athletes with exertional symptoms - does not fully explain relief with massage |
| Myocarditis | Can follow vigorous exercise; typically more persistent pain + systemic features |
| Pericarditis | Usually sharp, pleuritic, positional - not relieved by massage |
| Coronary artery spasm (Prinzmetal) | Possible; typically nocturnal; no palpitations |
The absence of all anginal equivalents (no radiation to arm/jaw, no diaphoresis, no nausea, no breathlessness, no palpitations) and relief specifically with massage significantly lower the pre-test probability of a cardiac cause.
3. Other Causes to Consider
- Intercostal neuritis / radiculopathy - brief electric/lancinating pain in the chest wall; may be precipitated by unusual postures during exercise
- GERD / esophageal spasm - can mimic cardiac heaviness; however, massage relief is not typical; look for heartburn or food-related triggers
- Anxiety / panic - brief episodes of chest tightness are possible, though these tend to be associated with palpitations or breathlessness
Red Flags to Rule Out (Ask/Examine For)
These features should be actively sought to avoid missing a serious cause:
- Any family history of sudden cardiac death or premature CAD?
- Any syncope or near-syncope during or after exercise?
- Is the pain reproducible on pressing the chest wall? (if YES - strongly supports musculoskeletal)
- Any systolic murmur (HOCM)?
- Any fever, viral illness preceding this? (myocarditis)
- ECG changes?
Recommended Workup
Minimum:
- ECG - to exclude ischemia, HOCM pattern, arrhythmia
- Chest wall palpation - if pain is reproduced by pressing specific costochondral junctions, this confirms musculoskeletal origin
- Troponin - if any doubt remains about cardiac cause (likely to be normal here)
Additional if clinically indicated:
- Echocardiogram - if HOCM suspected (young athlete, exertional symptoms)
- Exercise stress test - only if ischemia is a genuine concern after initial workup
Clinical Bottom Line
This presentation is most consistent with musculoskeletal chest wall pain (costochondritis or chest wall muscle strain) following high-intensity cardio. The single most important feature is that massage relieved the pain - this is not a feature of any cardiac or visceral cause of chest pain. Chest wall tenderness on palpation at the costochondral junctions would confirm this.
Cardiac causes are low probability in a 31-year-old with no risk factors, no associated symptoms, and pain lasting only seconds - but an ECG is still warranted as a baseline safety net given the central location and description of "heaviness."
Management if musculoskeletal confirmed: NSAIDs (e.g., ibuprofen), rest from intense chest-loading exercise for 1-2 weeks, local heat/massage. - Frameworks for Internal Medicine
Note: This is a clinical analysis for educational/decision-support purposes. Full history, physical examination, and clinical judgment by the treating clinician remain essential.
He is going to do a cardiac stress test and echo today , taken via a package..... Consultation will be after doing the tests with the results
That's a good approach - getting objective data before the consultation is smart, especially since the echo will help rule out structural causes like HOCM, and the stress test will assess for inducible ischemia.
Here's what to look for when the results come in:
What to Expect & Interpret from the Tests
Echocardiogram - Key Things to Assess
| Finding | Significance |
|---|---|
| Normal wall motion, normal EF | Reassuring - no structural/ischemic cause |
| Asymmetric septal hypertrophy (ASH), SAM of mitral valve | Suggests HOCM - important in young athlete with exertional symptoms |
| Pericardial effusion | Points toward pericarditis/myocarditis |
| Mitral valve prolapse | Can cause atypical chest pain in young adults |
| Dilated chambers, reduced EF | Would suggest myocarditis or DCM |
| Regional wall motion abnormality | Suggests ischemia - though very unlikely at 31 with no risk factors |
Cardiac Stress Test - Key Things to Assess
| Finding | Significance |
|---|---|
| Normal - no ST changes, good exercise capacity, no symptoms reproduced | Strongly reassures against ischemia or HOCM obstruction |
| ST depression ≥1mm, horizontal/downsloping | Inducible ischemia - warrants further workup |
| Chest pain reproduced during test | Important - note at what stage (rest, low/high workload) |
| Significant BP drop during exercise | Suggests LVOTO (HOCM) or severe ischemia |
| Arrhythmia provoked (VT, SVT) | Would need urgent cardiology review |
| Chronotropic incompetence | Suggests conduction/autonomic issue |
Most Likely Scenario Given This Presentation
Given the clinical picture (31yo, symptoms lasting seconds, relief with massage, post-exercise muscle strain context), the most expected results are:
- Echo: Normal (normal LV size, normal EF, no LVOTO, no effusion)
- Stress test: Negative (no inducible ischemia, good heart rate response, no arrhythmias, no ST changes)
A normal echo + negative stress test in this context would confidently confirm a non-cardiac cause - pointing back to musculoskeletal chest wall strain as the diagnosis.
For the Consultation - Suggested Talking Points
Once results are available, the clinician should:
- If both tests normal - reassure the patient, explain musculoskeletal etiology, advise NSAIDs + rest from heavy chest workouts for 1-2 weeks, and advise return if pain recurs/worsens
- If echo shows any structural abnormality - refer to cardiologist before resuming high-intensity exercise
- If stress test is positive - urgent cardiology referral regardless of age
Feel free to share the results here once they're available and I can help interpret them in context of the full clinical picture.
Is it safe to do these tests without prior cardiology consultation
A reasonable question. Here's a direct, evidence-based answer:
Is it Safe to Proceed Without Prior Cardiology Consultation?
Short Answer: Yes, in this case - with one important caveat about the stress test
Echocardiogram - Completely Safe
An echo is a non-invasive, zero-risk imaging test. There is no scenario where doing an echo without prior cardiology review causes harm. It only provides information. Safe to proceed without any preconditions.
Cardiac Stress Test - Generally Safe, But Needs Pre-Test Screening
The stress test carries very small but real risks, including:
- Provoked arrhythmia
- Myocardial infarction (rare)
- Cardiac arrest (1 in ~10,000 tests)
However, these risks apply mainly when the test is done in high-risk or unstable patients. The standard safety screening before a stress test asks:
| Question | This Patient |
|---|---|
| Acute MI in last 2 days? | No |
| Unstable angina (ongoing rest pain)? | No - pain was brief, self-limiting |
| Uncontrolled arrhythmia? | No palpitations reported |
| Severe symptomatic aortic stenosis? | No |
| Active heart failure? | No dyspnea |
| Acute myocarditis/pericarditis? | No fever, no systemic features |
This patient has none of the absolute contraindications to exercise stress testing. A baseline ECG should be done first - which any stress test facility will do as standard protocol before starting the test.
What Makes This Acceptable Without Prior Cardiology Review
- Symptoms are not ongoing or at rest - pain was brief, episodic, now resolved
- No hemodynamic instability - no syncope, no breathlessness, no sustained symptoms
- Both tests are being done together - if the echo is done first and reveals something like severe HOCM or severe AS, the stress test can be cancelled before it starts
- Qualified technician + crash cart - any accredited facility running stress tests will have resuscitation equipment and a physician on-site
The One Precaution Worth Noting
Ideally, the echo should be reviewed before the treadmill starts. Many packages do the echo and stress test sequentially on the same day. If the echo shows:
- Severe LVOTO (HOCM)
- Severe aortic stenosis
- Severely reduced EF
...the stress test should be deferred. A competent cardiologist or physician supervising the tests on-site should make that call in real time - which is standard practice.
Bottom Line
For a 31-year-old male with brief, self-resolving chest pain, no ongoing symptoms, and no red flags, proceeding with a package echo + stress test without a prior dedicated cardiology consultation is safe and actually good practice. Having objective data in hand before the consultation makes that consultation far more productive.
The consultation after the tests - with results - is the right sequence here.
This is a shared conversation. Sign in to Orris to start your own chat.