Role of Diagnostic ultrasound in Neck pain
Reading File
Finding Sources
Finding Sources
Searching PubMed
ultrasound neck pain diagnosis
Reading File
Reading File
Finding Sources
Searching PubMed
"musculoskeletal ultrasound" AND "cervical spine" AND pain
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching PubMed
ultrasound guided injection cervicogenic headache neck pain
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
ultrasonography neck pain soft tissue muscle tendon evaluation
Loading Image
Loading Image
Searching the Web
diagnostic ultrasound neck pain clinical applications 2024 2025 musculoskeletal cervicogenic
I now have comprehensive material from multiple textbooks and recent literature. Let me compile a thorough, well-structured answer.
Diagnostic Ultrasound in Neck Pain
Diagnostic ultrasound has become one of the most versatile first-line imaging tools for neck pain evaluation. Its advantages - real-time imaging, no ionizing radiation, portability, low cost, and compatibility with guided interventions - make it uniquely suited to the superficial anatomy of the neck. Nearly all clinically relevant cervical structures lie within 5 cm of the skin surface, placing them well within the optimal resolution range of a high-frequency (7-15 MHz) linear transducer.
1. Physics and Technical Principles
The neck is imaged with high-frequency linear transducers (7-15 MHz), which provide excellent resolution of superficial structures. Higher frequencies give better spatial resolution but less depth penetration, while lower frequencies penetrate deeper with reduced resolution. B-mode (gray-scale) imaging defines structure, while color Doppler characterizes vascularity and differentiates solid from vascular lesions. The technique is highly operator-dependent, requiring familiarity with cervical anatomy and pathology.
Key terms:
- Hyperechoic: bright (e.g., bone cortex, fat, fibrous tissue)
- Hypoechoic: dark (e.g., muscle, fluid collections, many malignant nodes)
- Anechoic: completely dark with posterior acoustic enhancement (e.g., simple cysts)
(Cummings Otolaryngology Head and Neck Surgery, Ch. 114)
2. Thyroid Gland - the Dominant Cervical US Application
Thyroid pathology is among the most common causes of neck discomfort, fullness, and pain (including Hashimoto thyroiditis causing neck pain and globus sensation). Ultrasound is the gold standard modality for thyroid nodule evaluation.
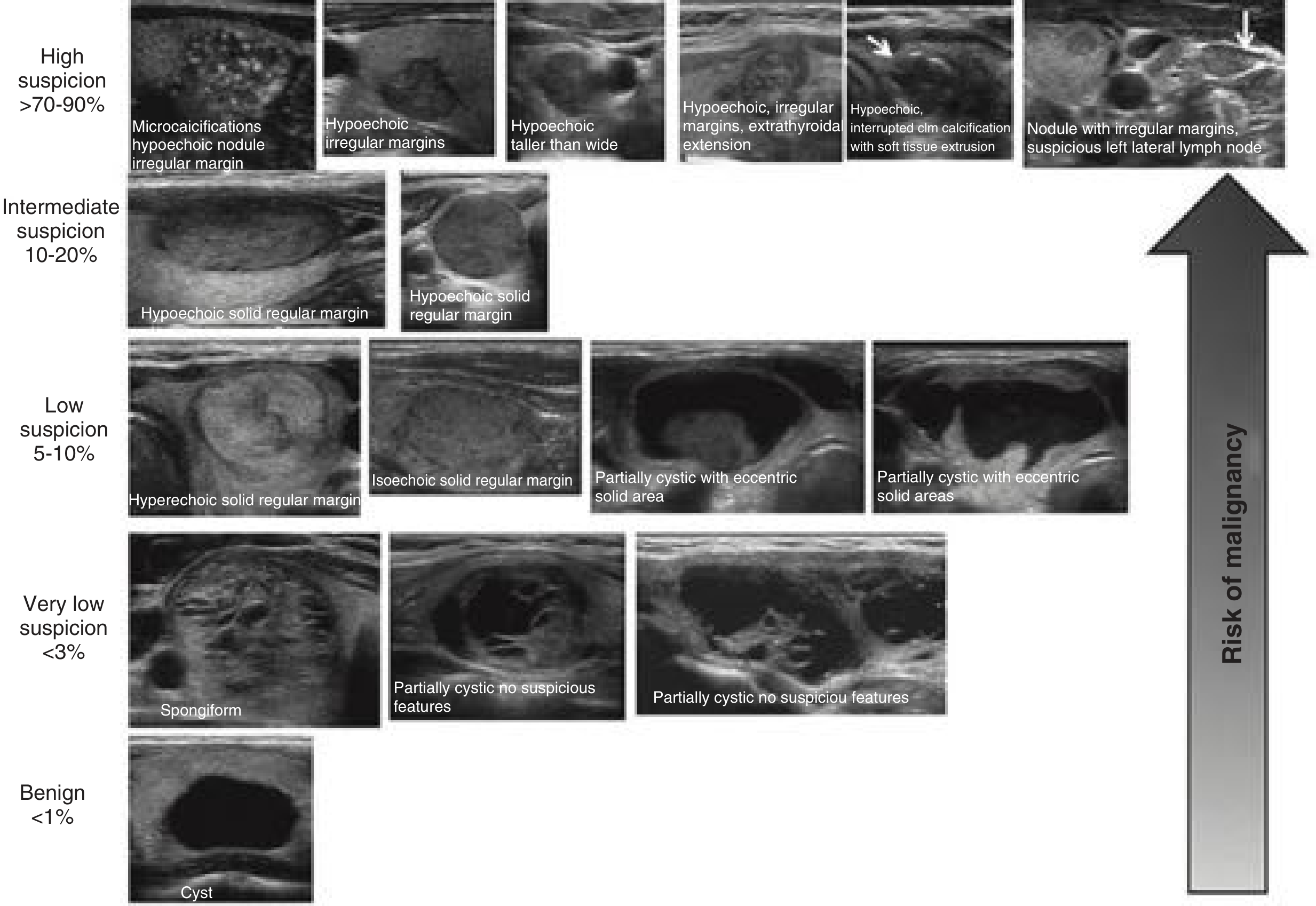
Sonographic Features Suggesting Malignancy
| Feature | Significance |
|---|---|
| Microcalcifications | High suspicion (>70-90% malignancy risk) |
| Hypoechogenicity with irregular margins | High suspicion |
| Taller-than-wide orientation | High suspicion - PTC |
| Extrathyroidal extension | High suspicion |
| Interrupted rim calcification with soft tissue extrusion | High suspicion |
| Hyperechoic, regular margin nodule | Low suspicion (5-10%) |
| Spongiform or purely cystic | Very low (<3%) or benign (<1%) |
ATA Thyroid Nodule Sonographic Patterns and Risk of Malignancy:
Risk-based management algorithm (ATA guidelines):
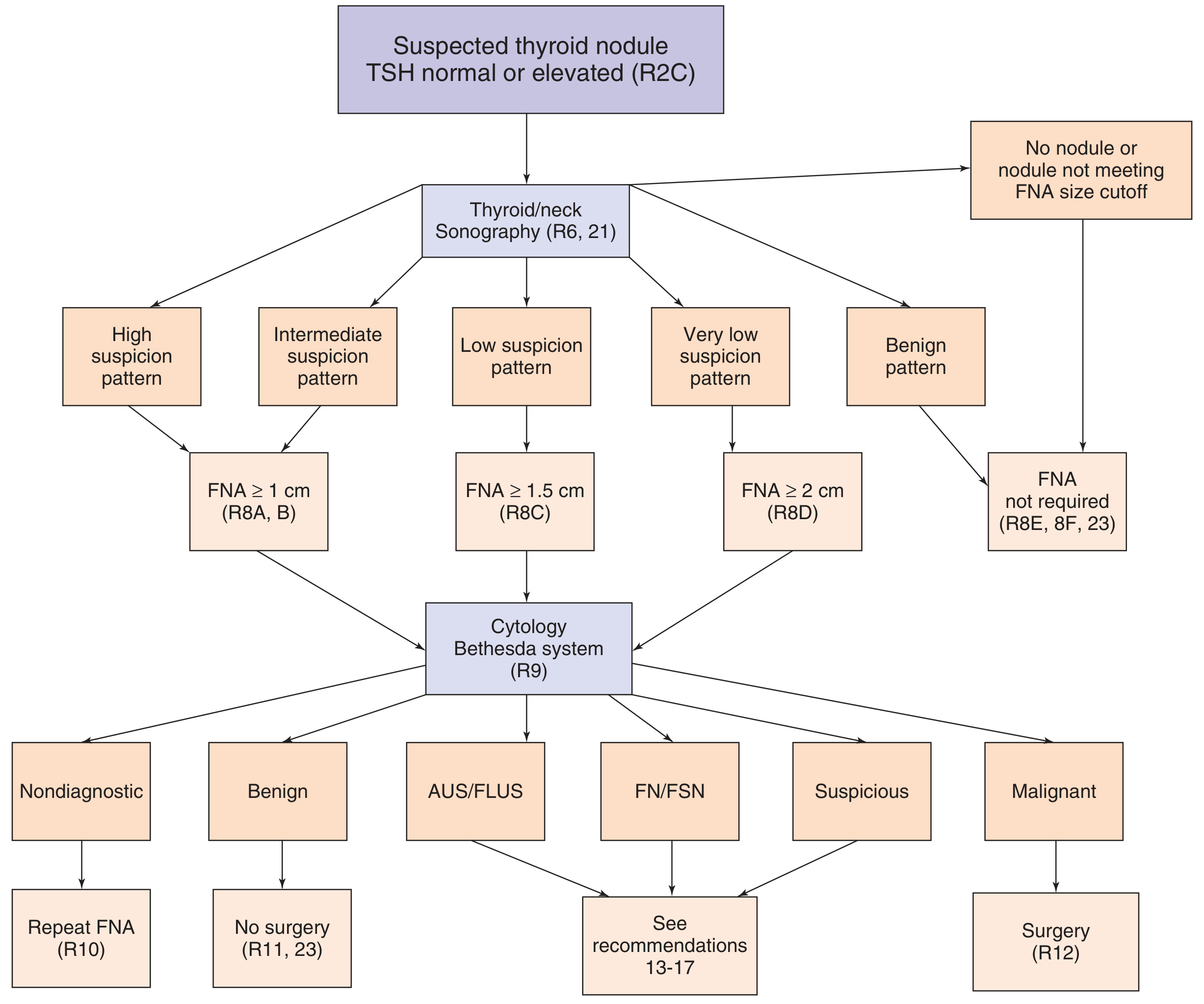
- FNA is indicated at ≥1 cm for high suspicion, ≥1.5 cm for intermediate, ≥2 cm for very low suspicion patterns
- US-guided FNA reduces nondiagnostic rates compared to palpation-guided biopsy
- For surveillance of thyroid carcinoma, neck US is considered the most sensitive tool for detecting recurrent/residual disease, especially when combined with serum thyroglobulin or calcitonin
(Cummings Otolaryngology, Ch. 114; Sabiston Surgery)
3. Parathyroid Localization
When neck pain accompanies hypercalcemia or hyperparathyroidism, US identifies hyperfunctioning parathyroid adenomas (responsible for 90-95% of primary hyperparathyroidism). Key sonographic features include:
- Oval, homogeneous, markedly hypoechoic lesion posterior and inferior to the thyroid lobe
- Peripheral "feeding vessel" blood supply on Doppler (distinguishes from reactive lymph nodes, which show hilar vascularity)
- Intrathyroidal adenomas can be confirmed with US-guided FNA + needle wash for intact PTH (values typically in the thousands mg/dL)
Limitations: posterior mediastinal adenomas cannot be visualized; chest CT/MRI/SPECT-CT is needed if deep mediastinal location is suspected.
(Cummings Otolaryngology, Ch. 114)
4. Cervical Lymphadenopathy
Lymph node assessment is a core part of neck US, especially when neck pain accompanies a palpable neck mass or in the context of head and neck malignancy.
Sonographic Features of Malignant Lymphadenopathy
- Loss of echogenic fatty hilum
- Round shape (loss of normal oval morphology)
- Hypoechoic or heterogeneous echotexture
- Microcalcifications (highly specific for papillary thyroid carcinoma metastases)
- Cystic component
- Peripheral rather than hilar vascularity on Doppler
- Irregular or ill-defined borders
- Extranodal extension
US combined with FNA is highly effective for evaluating metastatic lymph nodes in head and neck cancer. The upper third of the internal jugular chain, retropharyngeal, and tracheoesophageal groove nodes are poorly evaluated by US due to bony or airway obscuration.
(Cummings Otolaryngology, Ch. 114; Goldman-Cecil Medicine)
5. Salivary Gland Pathology
Salivary gland disorders (parotid and submandibular) frequently cause neck or facial pain. US applications include:
- Detection of salivary duct stones as small as 2 mm (appearing as hyperechoic foci with posterior acoustic shadowing)
- Dilated ducts seen as tubular anechoic structures
- Abscess detection and real-time guidance for drainage during acute sialadenitis
- Assessment of mass margins (well-defined = likely benign; infiltrative = suggests malignancy)
- Limitation: deep lobe of the parotid is obscured by mandible/mastoid - MRI/CECT preferred for deep extension
(Cummings Otolaryngology, Ch. 114; APPLICATIONS section)
6. Vascular Structures - Carotid and Vertebral Arteries
Neck pain can arise from vascular causes (carotid artery disease, vertebral artery dissection), and US is the first-line vascular screening tool:
- Duplex ultrasound (B-mode + Doppler) reliably identifies and quantifies internal carotid artery stenosis at its origin
- Color Doppler differentiates vascular from cystic/solid lesions
- Carotid body tumors, carotid tortuosity, and subclavian artery anomalies can mimic other neck masses
- Invasion of the carotid by tumor: loss of the echogenic fascial plane between vessel wall and tumor is a sonographic sign of carotid encasement
- Duplex ultrasound is listed among key diagnostic studies for neck mass evaluation including carotid-related causes
(Neuroanatomy through Clinical Cases, 3rd Ed.; Harrison's Principles of Internal Medicine 22E; Current Surgical Therapy 14e)
7. Musculoskeletal and Soft Tissue Applications
This is a growing area of neck US, particularly relevant to mechanical neck pain and cervical radiculopathy:
Muscles and Fascial Planes
- Evaluation of cervical paraspinal muscles, trapezius, sternocleidomastoid, scalene muscles
- Detection of myofascial trigger points (appearing as hypoechoic foci within muscle)
- Muscle tears, hematomas, and inflammatory changes post-whiplash
Cervical Spondylosis and Radiculopathy
- US-guided cervical nerve root blocks and pulsed radiofrequency for cervical radiculopathy are increasingly performed under real-time ultrasound guidance
- US-guided acupotomy for cervical spondylosis has been evaluated in systematic review (Frontiers in Pain Research, 2025), showing benefit for pain and function
- US-guided C2 transverse process injections with myofascial release have been described for cervicogenic headache (PMID 41245473, 2025)
Cervicogenic Headache
- Ultrasound-guided interfascial blocks of the trapezius muscle have been used for cervicogenic headache (Arıcı et al., Agri 2023, PMID 36625186)
- Emerging evidence supports ultrasound-guided interventional approaches targeting the greater occipital nerve, cervical facet joints (C2-C3), and perivertebral musculature (PMID 39828851, J Pak Med Assoc 2025)
Point-of-Care Applications
- Localization of the cricothyroid membrane using POCUS in difficult airway management with neck anatomy (Rosen's Emergency Medicine)
- Identification and drainage of neck abscesses (Harriet Lane Handbook; Rosen's)
- Rapid evaluation of neck swelling to differentiate hematoma, abscess, vascular injury, or lymphadenopathy at bedside
8. US-Guided Fine-Needle Aspiration Biopsy (FNAB)
US-guided FNAB is the gold standard technique for tissue sampling in the neck:
- Reduces sampling error compared to palpation-guided biopsy
- Decreases nondiagnostic rates (5-20% for thyroid FNAB overall, lower with US guidance)
- Applicable to thyroid nodules, cervical lymph nodes, salivary gland masses, and parathyroid adenomas
- On-site cytopathologist evaluation can further reduce nondiagnostic rates
- For intrathyroidal parathyroid adenomas: needle wash for intact PTH distinguishes parathyroid from thyroid tissue
(Cummings Otolaryngology, Ch. 114)
9. Limitations of Neck Ultrasound
| Limitation | Clinical Implication |
|---|---|
| Cannot penetrate bone/cartilage | Cannot assess vertebral bodies, foramina, spinal canal |
| Cannot reliably assess perineural spread | CT/MRI needed for nerve invasion |
| Cannot evaluate retropharyngeal or mediastinal nodes | CT/MRI needed for deep nodal stations |
| Cannot evaluate skull base | MRI preferred |
| Operator-dependent | Requires dedicated training |
| Large neck habitus | Increased attenuation reduces resolution |
10. Comparison with Other Modalities
| Modality | Advantage over US | When preferred |
|---|---|---|
| CT | Bony detail, deep spaces, airway | Trauma, deep neck space infection, staging |
| MRI | Perineural spread, marrow, disc disease | Cervical disc herniation, myelopathy, soft tissue detail |
| PET-CT | Metabolic activity, distant disease | Head and neck cancer staging/surveillance |
| Radionuclide (SPECT) | Ectopic parathyroid in mediastinum | Failed US parathyroid localization |
Summary
Diagnostic ultrasound is a first-line modality in neck pain for:
- Thyroid nodule risk stratification and FNA guidance
- Parathyroid adenoma localization
- Cervical lymph node characterization and staging
- Salivary gland pathology (calculi, abscess, neoplasm)
- Carotid and vascular duplex assessment
- Real-time guidance for cervical nerve blocks, facet injections, and musculoskeletal interventions
- Bedside POCUS for airway, abscess, and acute neck swelling
Its key strengths - real-time imaging, no radiation, portability, procedural guidance capability, and exquisite resolution for superficial structures - make it arguably the most clinically impactful imaging tool in the neck, with ongoing expansion into interventional pain management for cervicogenic and radiculopathic neck pain.
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Ch. 114 (Ultrasound Imaging of the Neck)
- Sabiston Textbook of Surgery, Thyroid/Parathyroid US sections
- Harrison's Principles of Internal Medicine, 22E - Carotid Doppler techniques
- Neuroanatomy through Clinical Cases, 3rd Ed. - Vascular Doppler
- Rosen's Emergency Medicine - POCUS neck applications
- Arıcı T et al., Agri 2023 (PMID 36625186) - Ultrasound-guided trapezius interfascial blocks for cervicogenic headache
- Razaq A et al., J Pak Med Assoc 2025 (PMID 39828851) - Ultrasound-guided interventional management in cervicogenic headache
- Hao L et al., J Pain Res 2025 (PMID 41245473) - US-guided C2 transverse process injection
This is a shared conversation. Sign in to Orris to start your own chat.