Teach me carprazine as a whole..like yiu taught lithium previously
Reading File
Finding Sources
Finding Sources
Searching the Web
cariprazine pharmacology mechanism clinical uses 2024 2025
Searching PubMed
cariprazine pharmacology clinical review
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
cariprazine receptor binding pharmacology D3 D2
Reading File
Loading Image
I now have everything I need. Let me compile the comprehensive cariprazine teaching note.
Cariprazine (Vraylar) — Complete Pharmacology Teaching
1. Identity & Classification
| Feature | Detail |
|---|---|
| Trade name | Vraylar (USA) |
| Drug class | Atypical antipsychotic / dopamine–serotonin partial agonist |
| NbN classification | Pharmacologic domain: Dopamine + Serotonin; Mechanism: Receptor partial agonist (D2, D3, 5-HT1A) + antagonist (5-HT2B) |
| Developer | Gedeon Richter (Budapest); licensed to Allergan/AbbVie for USA & Canada |
| FDA approvals | Schizophrenia (2015) → Bipolar I mania (2015) → Bipolar I depression (2019) → Adjunctive MDD (2022) |
2. Mechanism of Action — The Star Feature: D3 >> D2
This is what sets cariprazine apart from every other antipsychotic.
Receptor Profile
| Receptor | Action | Affinity |
|---|---|---|
| D3 | Partial agonist | Ki = 0.09 nM — 3 orders of magnitude higher than dopamine itself |
| D2 | Partial agonist | Ki ~0.49 nM |
| 5-HT1A | Partial agonist | Moderate |
| 5-HT2B | Antagonist | High |
| 5-HT2A | Antagonist | Moderate |
| H1, α1, α2 | Antagonist | Weaker |
Critical concept: Dopamine's own Ki for D3 is ~60 nM. Cariprazine's Ki is 0.09 nM — ~667× more potent than dopamine at D3. In contrast, aripiprazole (Ki ~17.7 nM) and risperidone (Ki ~8 nM) cannot successfully compete with dopamine for the D3 receptor at clinical doses. Cariprazine and blonanserin are the only clinically available agents that reliably block D3 in vivo.
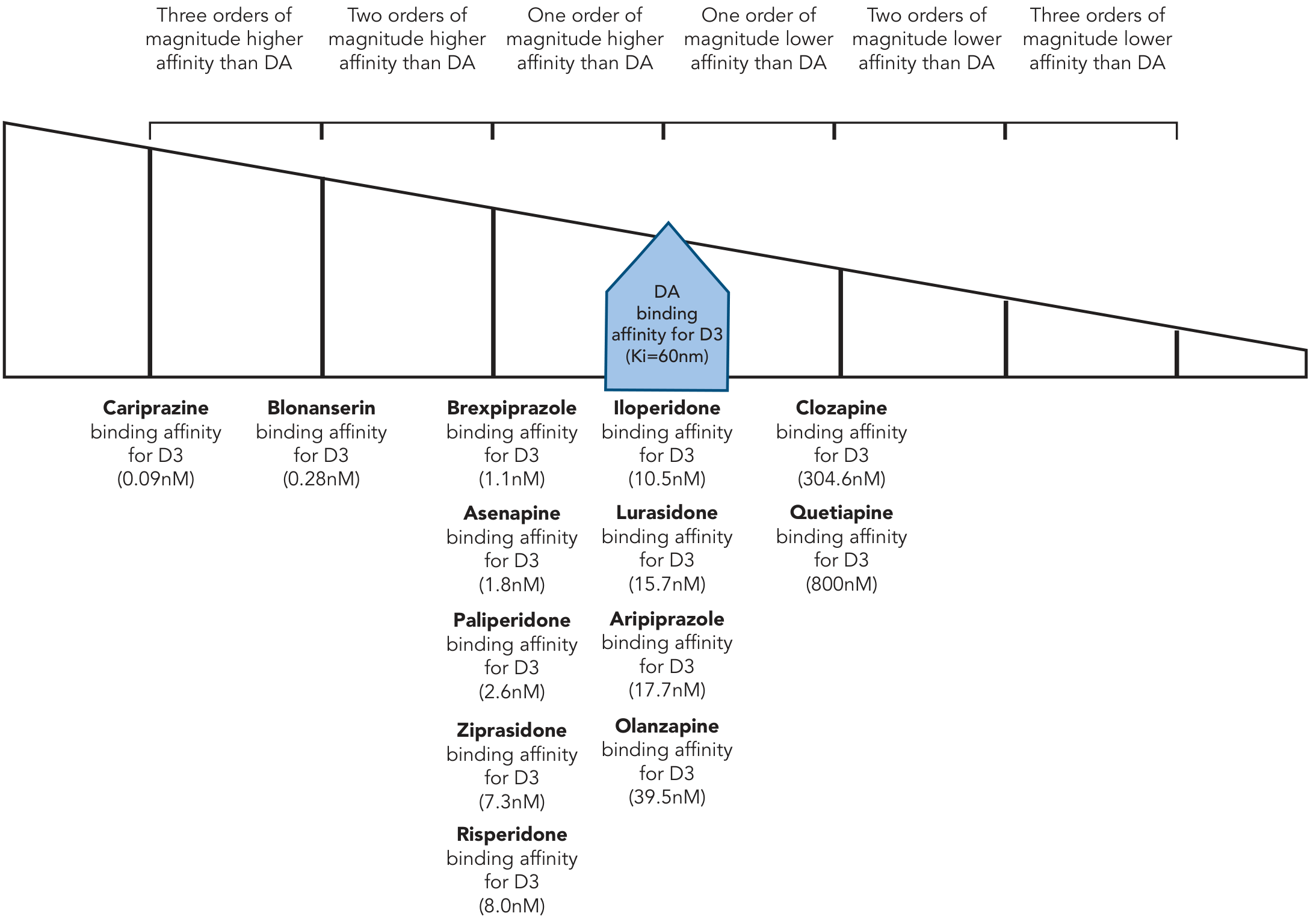
From Stahl's Essential Psychopharmacology — cariprazine sits three orders of magnitude to the left of dopamine's own affinity
PET Evidence
At just 1 mg/day, PET studies show cariprazine achieves 76% D3 occupancy vs 45% D2 occupancy — confirming true D3 selectivity over D2 at clinical doses.
3. Why Does D3 Partial Agonism Matter?
This is the mechanistic backbone explaining cariprazine's unique clinical benefits:
Presynaptic D3 in the VTA → More Dopamine in PFC
- D3 receptors sit as somatodendritic autoreceptors on mesocortical dopamine cell bodies in the VTA
- Normally: dopamine activates these D3 autoreceptors → inhibits further dopamine release → reduced cortical dopamine → depression, negative symptoms, cognitive deficits
- Cariprazine blocks these VTA D3 autoreceptors → disinhibits the mesocortical neurons → increased dopamine release onto D1 receptors in the prefrontal cortex
- Downstream effect: improved motivation, energy, cognition, negative symptoms — the "brightening" effect
Postsynaptic D3 in Limbic Regions → Antipsychotic
- Blockade of postsynaptic D3 in limbic emotional striatum reduces dopamine overactivity → antipsychotic and mood-stabilizing effects
This dual D3 action explains why cariprazine is one of the few drugs proven to improve negative symptoms of schizophrenia more than other antipsychotics.
4. Pharmacokinetics
Absorption
- Oral, well absorbed; Tmax: 3–6 hours
- Food does not significantly affect absorption
Metabolism — The "Three Active Moieties" Concept
This is a key pharmacokinetic distinction:
| Moiety | Half-life | Notes |
|---|---|---|
| Cariprazine (parent) | 2–5 days | Active |
| Desmethyl-cariprazine (DCAR) | Similar to parent | Active, equipotent |
| Didesmethyl-cariprazine (DDCAR) | 1–3 weeks | Active, equipotent — the dominant species at steady state |
- All three moieties are equipotent at therapeutic receptors
- Metabolized by CYP3A4 (primary) and CYP2D6
- Steady state: cariprazine + DCAR reach it in 1–2 weeks; DDCAR takes 4–8 weeks
- Elimination: ~21% excreted in urine
Clinical Implications of the Long Half-Life
- Slow accumulation — patients starting cariprazine see a gradual rise in active drug over weeks (set expectations)
- Long washout — when stopped, the active moiety persists in plasma for weeks (important for drug interactions and switching)
- Potential "oral depot" — Stahl's notes cariprazine's metabolite kinetics make it theoretically suitable for development as a weekly/biweekly oral depot formulation
- CYP3A4 interactions — if co-prescribed with a strong CYP3A4 inhibitor (e.g., ketoconazole, clarithromycin), reduce the cariprazine dose; strong inducers would reduce efficacy
5. FDA-Approved Indications & Dosing
| Indication | Dose Range | Starting Dose |
|---|---|---|
| Schizophrenia | 1.5–6 mg/day | 1.5 mg/day |
| Bipolar I — Acute Mania/Mixed | 3–6 mg/day | 1.5 mg/day |
| Bipolar I — Depression | 1.5–3 mg/day | 1.5 mg/day |
| Adjunctive MDD | 1.5–3 mg/day | 1.5 mg/day |
Key dosing principles:
- Lower doses (1.5–3 mg) favor D3 selectivity and antidepressant effects
- Higher doses (3–6 mg) engage more D2 and are needed for schizophrenia/mania
- Slow titration reduces akathisia
- No dose adjustment needed for mild-moderate hepatic or renal impairment
6. Clinical Trial Evidence
Schizophrenia (3 positive trials)
- Phase II: cariprazine 1.5–4.5 mg vs risperidone 4 mg vs placebo → cariprazine significantly improved total PANSS
- Trial 2: 3 mg and 6 mg superior to placebo (aripiprazole 10 mg as active reference)
- Trial 3: 3–6 mg and 6–9 mg both superior to placebo
Landmark negative symptoms trial:
26-week double-blind RCT, cariprazine (mean 4.2 mg) vs risperidone (mean 3.8 mg) in patients with predominantly negative symptoms → cariprazine showed significantly greater improvement in PANSS negative factor score. This is exceptional — most antipsychotics don't separate from each other on negative symptoms.
Bipolar Mania (3 positive trials)
- Two flexible-dose studies (3–12 mg/day) → cariprazine > placebo on YMRS
- Third trial: 3–6 mg and 6–12 mg both beat placebo; no efficacy advantage for higher dose range
Bipolar I Depression (key trial)
- Cariprazine 0.75, 1.5, or 3.0 mg/day vs placebo
- 1.5 mg and 3 mg significantly improved MADRS; 0.75 mg did not separate from placebo
- Low metabolic burden compared to quetiapine makes this a preferred option
Adjunctive MDD
- 8-week trial: adjunctive cariprazine 1–2 mg/day, 2–4.5 mg/day, or placebo added to antidepressant
- 2–4.5 mg/day group showed significantly greater improvement on MADRS
- FDA approved in 2022 for this indication
7. Adverse Effects
Most Common
| Side Effect | Comment |
|---|---|
| Akathisia | Most important; dose-related; slow titration helps greatly |
| EPS / Drug-induced parkinsonism | Lower incidence than older antipsychotics due to strong 5-HT1A partial agonism |
| Nausea, vomiting | Especially early in treatment |
| Somnolence/sedation | Less than quetiapine or olanzapine |
| Constipation | Moderate |
Metabolic Profile — A Major Advantage
- Very low propensity for weight gain
- Minimal metabolic disturbance (minimal glucose and lipid effects)
- Comparable to lurasidone in this regard — both are preferred when metabolic side effects are a concern
Black Box Warnings
- Increased mortality in elderly patients with dementia-related psychosis (class warning for all antipsychotics — not specifically proven worse for cariprazine)
- Neonatal EPS/withdrawal — neonates exposed in the third trimester are at risk for EPS and withdrawal symptoms after delivery
Pregnancy Considerations
- Dopamine-modulating drugs as a class: neonatal EPS/withdrawal risk in 3rd trimester exposure
8. Comparison with Aripiprazole (its closest "cousin")
Both are D2/D3/5-HT1A partial agonists, but:
| Feature | Cariprazine | Aripiprazole |
|---|---|---|
| D3 affinity | 0.09 nM (3 orders above DA) | 17.7 nM (lower than DA) |
| D3 receptor occupancy in vivo | Substantial at clinical doses | Minimal |
| Negative symptoms | Superior (head-to-head vs risperidone) | Not demonstrated |
| Bipolar depression | FDA approved | Not approved |
| Active metabolites | 2 long-acting (DDCAR: 1–3 weeks) | 1 long-acting (dehydro-aripiprazole) |
| Metabolic effects | Very low | Very low |
| Akathisia | Can occur; slow titration helps | Can occur |
9. Place in Therapy — Where to Use Cariprazine
| Clinical Scenario | Why Cariprazine? |
|---|---|
| Schizophrenia with predominant negative symptoms | Only antipsychotic with head-to-head superiority data over risperidone for negatives |
| Bipolar depression | FDA approved; low metabolic burden; D3-mediated antidepressant mechanism |
| Mixed features (mania + depression together) | Post-hoc analyses show efficacy across the full mixed spectrum |
| Bipolar I full spectrum coverage | Only drug with robust evidence across mania, mixed, and depression |
| Patient with metabolic concerns | Minimal weight gain, minimal glucose/lipid effects |
| Adjunctive MDD when antidepressant alone is insufficient | 2022 FDA approval; 2–4.5 mg as add-on |
10. Drug Interactions
| Interactant | Effect | Action |
|---|---|---|
| Strong CYP3A4 inhibitors (ketoconazole, clarithromycin, ritonavir) | ↑ cariprazine/DDCAR levels | Reduce cariprazine dose |
| Strong CYP3A4 inducers (rifampin, carbamazepine) | ↓ levels | Avoid or increase dose with caution |
| CYP2D6 inhibitors | Minor additional effect | Monitor |
11. Summary: The "CARIP" Mnemonic
| Letter | Key Point |
|---|---|
| C | CYP3A4 metabolized → watch inhibitors/inducers |
| A | Akathisia is the main side effect; titrate slowly |
| R | Robusto D3 receptor affinity — unique across all antipsychotics |
| I | Indications: Schizophrenia, Bipolar mania, Bipolar depression, MDD adjunct |
| P | Perfect metabolic profile — minimal weight gain, no significant metabolic disruption |
12. Key Exam Points
- Cariprazine has higher affinity for D3 than dopamine itself (Ki 0.09 nM vs dopamine's 60 nM) — this is unique
- It is the only antipsychotic with head-to-head data showing superiority over risperidone for negative symptoms
- Two major active metabolites — DDCAR has a half-life of 1–3 weeks, making washout prolonged
- Bipolar depression dose (1.5–3 mg) is lower than schizophrenia/mania dose (1.5–6 mg)
- The antidepressant mechanism works via VTA D3 autoreceptor blockade → disinhibition of mesocortical dopamine → ↑ PFC D1 stimulation
- Very low metabolic burden — good choice in patients with obesity/diabetes risk
- Adjunctive MDD approval came in 2022 — the most recent FDA indication
- Akathisia > parkinsonism in its EPS profile (because 5-HT1A partial agonism reduces parkinsonism)
Sources: Stahl's Essential Psychopharmacology (Neuroscientific Basis), Kaplan & Sadock's Comprehensive Textbook of Psychiatry, The Maudsley Prescribing Guidelines 15th ed.
How to differentiate schizoaffrctive schizophrenia and mdd eith psychotic features
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.