H2S poisoning
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hydrogen sulfide" AND poisoning
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive answer.
Hydrogen Sulfide (H₂S) Poisoning
Overview
H₂S is a colorless, flammable gas with the characteristic "rotten egg" odor. It is one of the most common causes of fatal gas inhalation. Sources include:
- Occupational: petroleum refining, oil/gas industry, sewage/wastewater workers, manure pits, confined spaces
- Natural: geothermal/volcanic emissions
- Deliberate: suicide method — generated by mixing sulfur-containing detergents with acids in enclosed spaces (well-documented globally)
A critical rescue hazard: fatal enclosed-space incidents routinely claim additional victims when unprepared bystanders attempt rescue.
Pathophysiology
H₂S exerts toxicity through two mechanisms:
-
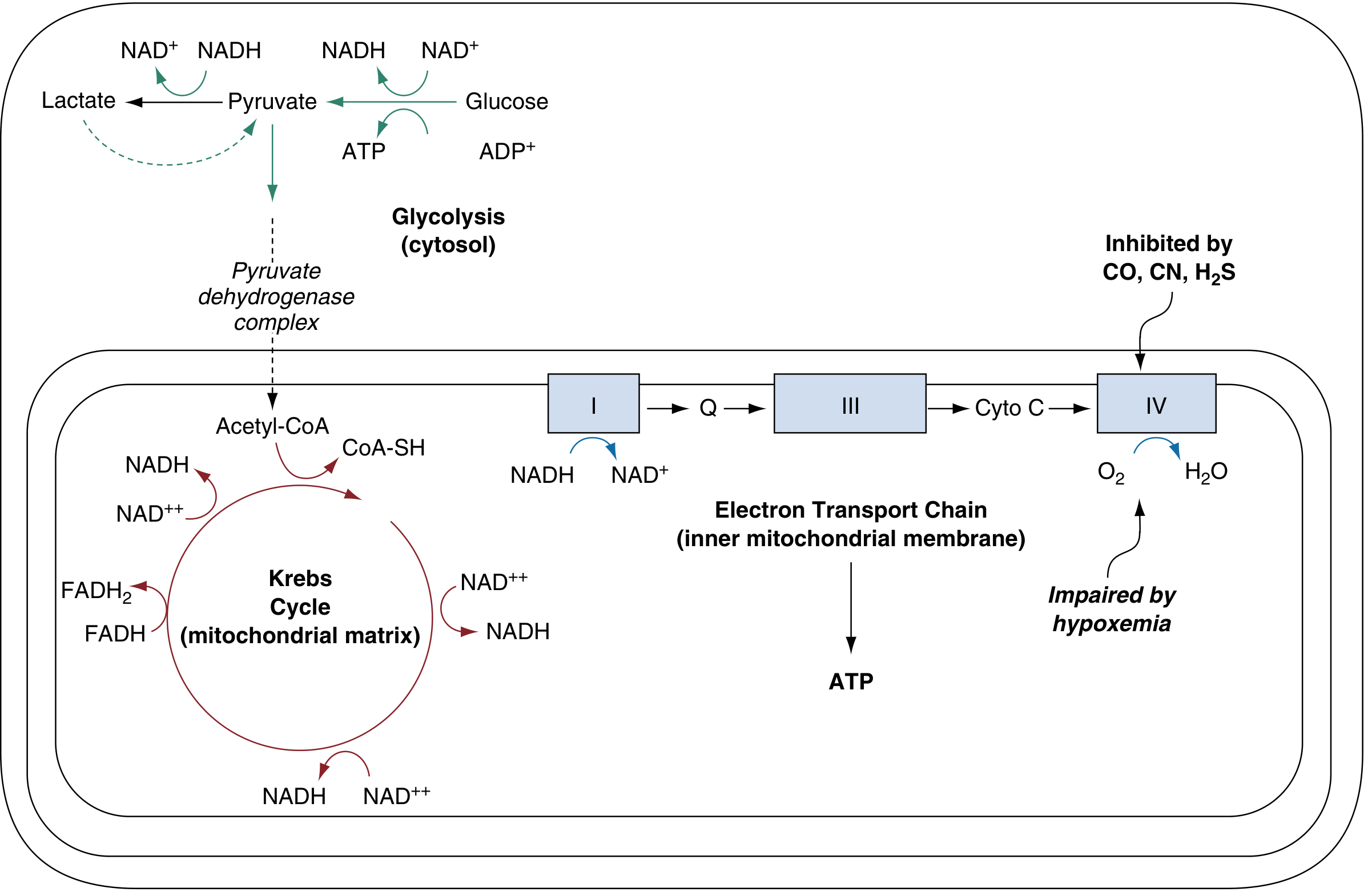
Cellular (cytotoxic) asphyxia — the primary lethal mechanism, identical to cyanide: H₂S binds to the Fe³⁺ of cytochrome c oxidase (Complex IV) in the mitochondrial electron transport chain, halting oxidative phosphorylation. ATP depletion forces anaerobic glycolysis → pyruvate → lactate accumulation → high anion-gap metabolic acidosis.
-
Pulmonary/mucosal irritation — H₂S is one of few chemical asphyxiants that also directly irritates mucous membranes (eyes, airways), causing conjunctivitis, rhinitis, and at high doses, acute lung injury / pulmonary edema.
Key distinction from cyanide: the H₂S–cytochrome bond dissociates spontaneously and rapidly, so patients who survive brief exposures often recover before arriving at the ED.
Olfactory Warning and Its Failure
The "rotten egg" odor is detectable at very low concentrations (~0.01–0.13 ppm). However, two phenomena eliminate the warning:
- Olfactory fatigue: prolonged low-level exposure desensitizes olfactory receptors
- Acute olfactory paralysis: at high concentrations, olfaction is immediately overwhelmed — the smell vanishes precisely when danger is greatest
Clinical Features
| Concentration | Effects |
|---|---|
| Low (≤50 ppm) | Eye/mucous membrane irritation, lacrimation, rhinorrhea |
| Moderate (50–500 ppm) | Headache, dizziness, nausea, cough, dyspnea |
| High (500–700 ppm) | Rapid loss of consciousness ("knockdown"), seizures |
| Massive (>700 ppm) | Death within minutes after a few breaths |
Systemic features (from cellular asphyxia):
- CNS: coma, seizures, agitation
- Cardiovascular: dysrhythmias, bradycardia, cardiovascular collapse
- Metabolic: high anion-gap metabolic acidosis, elevated lactate (>8 mmol/L is highly predictive)
- Pulmonary: delayed pulmonary edema in survivors of massive exposure
- Ocular: corneal injury ("gas eye") — keratoconjunctivitis, can be delayed
"Arterialization" of venous blood: Because tissues cannot extract O₂, venous blood oxygen content approaches arterial levels — a subtle but diagnostically important finding.
Delayed or persistent neuropsychiatric syndromes (similar to post-cardiac arrest or CO poisoning) can occur in survivors.
Diagnosis
- Clinical: primarily by exposure history and setting (occupational/enclosed space)
- ABG + co-oximetry: normal SpO₂ and ABG (unlike CO, pulse oximetry is accurate in isolated H₂S poisoning)
- Elevated lactate (>8 mmol/L supports cytotoxic asphyxiant poisoning)
- Anion-gap metabolic acidosis
- On-scene testing: field detectors; no widely available clinical blood H₂S assay
- Narrow A-V O₂ difference on co-oximetry is suggestive
Management
1. Scene Safety & Decontamination
- Rescuers must use self-contained breathing apparatus (SCBA) — do NOT enter without PPE
- Remove patient from source immediately
- Decontaminate skin and irrigate eyes
2. Supportive Care (all patients)
- High-flow 100% oxygen (primary treatment)
- Airway management, ventilatory support if needed
- For conscious patients with only mild symptoms, removal + O₂ is often sufficient
3. Antidotal Therapy (severe/unconscious patients)
| Agent | Dose | Mechanism | Notes |
|---|---|---|---|
| Sodium nitrite | 300 mg IV over 2–4 min (adult) | Induces methemoglobin → sulfide binds to MetHb forming less toxic sulfmethemoglobin | Must be given within minutes of exposure to be effective |
| Hydroxocobalamin | 5 g IV | Cobalt binds sulfide | Animal data promising; shown to lower sulfide levels but no confirmed human clinical benefit yet |
| Sodium thiosulfate | NOT indicated | — | H₂S is not detoxified by rhodanese; thiosulfate is unnecessary (unlike cyanide poisoning) |
| Hyperbaric oxygen | No defined role | — | Case reports exist but no evidence of superiority over normobaric O₂ |
Note: Amyl nitrite (inhaled) can be used pre-hospital as a MetHb inducer if IV access is unavailable.
4. Disposition
- All symptomatic patients: admit to ICU/critical care
- Monitor for delayed pulmonary edema, corneal injury, and neuropsychiatric sequelae
- Full recovery is achievable with rapid treatment, even in severe cases, provided cardiac arrest has not occurred
Key Differences: H₂S vs. Cyanide vs. CO
| Feature | H₂S | Cyanide (HCN) | CO |
|---|---|---|---|
| Mechanism | Complex IV inhibition | Complex IV inhibition | Complex IV + Hb binding |
| Bond reversibility | Rapid spontaneous | Slow | Moderate |
| Odor | Rotten eggs | Bitter almonds | Odorless |
| Irritant properties | Yes (eyes, airways) | No | No |
| Antidote | Nitrites (± hydroxocobalamin) | Hydroxocobalamin preferred | 100% O₂ / HBO |
| Thiosulfate needed | No | Yes | No |
| Pulse oximetry | Accurate | Accurate | Inaccurate (falsely normal) |
Sources: Tintinalli's Emergency Medicine, p. 1364 | Rosen's Emergency Medicine, p. 3001–3003 | Murray & Nadel's Respiratory Medicine, p. (block 24)
poison's gases in enclosed spaces and its management
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple textbooks covering all major toxic gases encountered in enclosed spaces. Here is the full synthesized answer:
Poisonous Gases in Enclosed Spaces & Their Management
Enclosed spaces concentrate toxic gases to lethal levels quickly. Toxicity depends on gas concentration, duration, solubility (determines where in the airway injury occurs), and mechanism (simple asphyxiation vs. chemical/cellular toxicity). Enclosed-space incidents frequently kill would-be rescuers who enter without proper equipment.
Classification of Toxic Gases
| Category | Mechanism | Examples |
|---|---|---|
| Simple asphyxiants | Displace O₂, no direct tissue toxicity | Methane, CO₂, nitrogen, argon, helium |
| Chemical asphyxiants | Block cellular O₂ utilization | CO, cyanide (HCN), H₂S |
| Pulmonary irritants | Direct airway/alveolar injury | Chlorine, ammonia, phosgene, NO₂ |
| Dual-mechanism | Both irritant + cellular asphyxiant | H₂S |
1. Carbon Monoxide (CO)
The most common cause of death from poisoning worldwide.
Sources in enclosed spaces: combustion of carbon-based fuels — house fires, car engines in garages, malfunctioning heaters/stoves, generators, charcoal grills indoors. Also a deliberate suicide method.
Pathophysiology:
- CO binds hemoglobin with 230–270× greater affinity than O₂ → forms carboxyhemoglobin (COHb) → left-shifts the O₂-dissociation curve → impairs O₂ delivery
- Also binds cytochrome c oxidase → direct cellular poisoning
- Net effect: tissue hypoxia with deceptively normal PaO₂ on standard ABG
Clinical features (by COHb level):
| COHb | Symptoms |
|---|---|
| 10–20% | Headache, nausea, malaise, fatigue, dizziness |
| 20–40% | Confusion, agitation, visual disturbance, tachycardia |
| 40–60% | Seizures, coma, cardiac arrhythmia/ischemia |
| >60% | Death |
- "Cherry-red" skin — rarely seen clinically
- Pulse oximetry is falsely normal — COHb reads as oxyhemoglobin; co-oximetry required
- Lactic acidosis, rhabdomyolysis, pulmonary edema in severe cases
- Delayed neuropsychiatric syndrome: cognitive dysfunction, mood disturbance, memory loss — can appear days to 9 months after recovery
Diagnosis: Co-oximetry measuring COHb; high clinical suspicion in fire/closed-space victims
Treatment:
| Step | Action |
|---|---|
| Remove from source | Immediate evacuation |
| 100% O₂ | Normobaric; reduces COHb half-life from ~5 hours → ~60 min |
| Hyperbaric O₂ (HBO) | 2.5–3.0 atm; increases dissolved O₂ 10-fold; 3 treatments within 24 h reduce delayed neuropsychiatric sequelae |
| Supportive | Airway, ventilation, treat arrhythmias, seizures |
HBO indications: coma/altered consciousness, COHb >25%, cardiac involvement, neurological deficits, pregnancy.
2. Hydrogen Sulfide (H₂S)
Among the most common causes of fatal gas inhalation.
Sources: petroleum/oil/gas industry, sewage tanks, manure pits, volcanic emissions, suicide (mixing sulfur-containing detergents with acid).
Pathophysiology (dual mechanism):
- Cellular asphyxia: binds cytochrome c oxidase (Complex IV) — identical to cyanide, but the bond dissociates rapidly and spontaneously → patients with brief exposure often recover before ED arrival
- Mucosal/pulmonary irritant: causes conjunctivitis, respiratory irritation, and at high dose, pulmonary edema + corneal injury
Key danger — olfactory failure: The "rotten egg" odor is lost at high concentrations via acute olfactory paralysis or at low sustained levels via olfactory fatigue, eliminating all warning.
Clinical features:
| Concentration | Effects |
|---|---|
| Low | Eye/throat irritation, lacrimation |
| Moderate | Headache, dizziness, cough, dyspnea |
| High | Rapid "knockdown" loss of consciousness, seizures |
| Massive | Death within seconds–minutes |
- High anion-gap metabolic acidosis + elevated lactate
- Delayed pulmonary edema and corneal burns in survivors
Treatment:
| Step | Action | Notes |
|---|---|---|
| Scene safety | SCBA for rescuers | Do NOT enter without PPE |
| Remove + decontaminate | Remove clothing, irrigate skin/eyes | |
| High-flow 100% O₂ | Primary treatment | Most patients recover with this alone |
| Sodium nitrite 300 mg IV over 2–4 min | Creates MetHb → sulfmethemoglobin | Only for severe/unconscious patients; must be given within minutes |
| Hydroxocobalamin | Binds sulfide | Animal evidence; no confirmed human benefit yet |
| Sodium thiosulfate | NOT indicated | H₂S not detoxified by rhodanese (unlike cyanide) |
| HBO | No defined role | Not shown superior to normobaric O₂ |
3. Hydrogen Cyanide (HCN)
Sources in enclosed spaces: combustion of synthetic materials (wool, nylon, silk, acrylic, polyurethane, melamine) — common in house/building fires with synthetics. Industrial uses (metallurgy, fumigation, chemical synthesis). Also a deliberate method in homicide/mass casualty events.
Pathophysiology: Binds Fe³⁺ of cytochrome oxidase (Complex IV) with high affinity → complete cessation of oxidative phosphorylation → cellular asphyxia despite normal O₂ delivery.
Clinical features:
- Headache, dyspnea, anxiety → seizures, coma, cardiovascular collapse
- "Arterialization" of venous blood (high venous O₂ saturation)
- High anion-gap metabolic acidosis; lactate >10 mmol/L correlates with toxic cyanide levels in fire victims
- Not cyanotic initially (hemoglobin O₂-carrying capacity unaffected)
- Bitter almond odor — present in only ~50% of people (genetic anosmia)
Key warning: In house fires with synthetic materials, CO and cyanide poisoning co-exist and are synergistically lethal.
Diagnosis: Clinical + lactate; whole-blood cyanide: toxic >0.5 µg/mL, fatal >2.5 µg/mL (results delayed, for confirmation only)
Treatment:
| Agent | Dose | Mechanism |
|---|---|---|
| Hydroxocobalamin (preferred) | 5 g IV over 15 min (adult); 70 mg/kg pediatric | Cobalt binds CN⁻ → cyanocobalamin → renal excretion |
| Sodium nitrite + Sodium thiosulfate (Cyanide Antidote Kit) | NaNO₂ 300 mg IV; Na₂S₂O₃ 12.5 g IV | Nitrite → MetHb (alternative CN binding site); thiosulfate + rhodanese → thiocyanate |
| 100% O₂ | Always give | Supportive |
Critical: If CO co-exposure is suspected (fire victim), use hydroxocobalamin — do NOT use nitrites (adding MetHb to CO-poisoned patient worsens O₂ delivery catastrophically).
Empirical treatment for fire victim with GCS <10 + lactate >8 mmol/L or COHb >10%: hydroxocobalamin without waiting for confirmation.
4. Chlorine (Cl₂)
Sources: Industrial leaks, swimming pool chemicals, water treatment plants, potential chemical weapon.
Pathophysiology: Intermediate water solubility → injures both upper AND lower airways. Reacts with moist mucosa → hydrochloric acid + hypochlorous acid → oxidative injury, inflammation.
Clinical features:
- Immediate: Pungent odor (good warning), eye/throat irritation, nausea/vomiting (low exposure)
- High exposure: Cough, hoarseness, bronchospasm, pulmonary edema within 6 hours; ARDS possible
Treatment:
- Remove from source
- Humidified 100% O₂
- Nebulized bronchodilators (β-agonists ± anticholinergics)
- Nebulized sodium bicarbonate — may neutralize acids, symptom relief
- Ocular irrigation
- Supportive respiratory care; no proven pharmacologic antidote
5. Phosgene (COCl₂)
Sources: Industrial chemical manufacturing (plastics, pharmaceuticals, dyes, pesticides, polyurethane). Heating of chlorinated fluorocarbons (Freon®). Former chemical warfare agent (WWI — caused 80% of gas fatalities).
Pathophysiology: Low water solubility → minimal upper airway warning → penetrates to alveoli → hydrolyzes to CO₂ + HCl → acylation of alveolar-capillary membranes → delayed capillary leak → noncardiogenic pulmonary edema (up to 24 h later).
Clinical features (triphasic):
- Immediate: Mild eye/throat irritation or none; characteristic "freshly mown hay" odor
- Latent: Apparent improvement
- Delayed (6–24 h): Dyspnea, pulmonary edema — onset within 4 hours = poor prognosis
Treatment:
- Mandatory rest — exertion dramatically worsens pulmonary edema
- O₂ only if SpO₂ <92% (avoid hyperoxia)
- Nebulized β-agonists, nebulized N-acetylcysteine, NSAIDs (animal/case report evidence)
- Early corticosteroids for lung injury
- Protective mechanical ventilation (low tidal volume, high PEEP) if intubation needed
- Observe all exposed patients ≥24 h even if initially asymptomatic
6. Nitrogen Dioxide (NO₂)
Sources: Silo gas ("silo filler disease"), products of combustion, industrial processes, blast weapons.
Pathophysiology: Low water solubility → penetrates deep to alveoli; slow conversion to nitric acid → delayed alveolar injury and pulmonary edema (12–72 h). Can also cause methemoglobinemia.
Clinical features — classic triphasic pattern:
- Initial: Mild dyspnea, flu-like symptoms
- Transient improvement
- Worsening dyspnea → pulmonary edema (12–72 h later)
Treatment:
- Supportive (humidified O₂, ventilatory support)
- Early corticosteroids — case reports show benefit for ALI
- Methylene blue if significant methemoglobinemia
7. Ammonia (NH₃)
Sources: Household cleaners, industrial chemicals, fertilizers, refrigeration systems.
Pathophysiology: Highly water-soluble → primarily upper airway injury; at high concentrations penetrates lower airways → bronchospasm, pulmonary edema, reactive airway disease.
Clinical features: Immediately pungent odor (good warning) → eye, nose, throat irritation, bronchospasm; severe exposure → pulmonary edema, permanent lung injury.
Treatment:
- Humidified O₂, nebulized bronchodilators
- Anticholinergics for secretion control
- Ocular irrigation (alkaline burns); evaluate for corneal injury
General Management Principles for All Enclosed-Space Gas Exposures
Scene Response
- Do NOT enter without appropriate respiratory protection (SCBA minimum)
- Identify the gas type if possible (on-scene monitors, history, odor)
- Evacuate all exposed persons
Emergency Management Algorithm
ALL EXPOSURES:
├── Remove from source
├── High-flow O₂ (100%)
├── Decontaminate skin/eyes as needed
├── Airway assessment (singed hair, hoarseness, soot = early intubation)
└── IV access + monitoring (ECG, SpO₂, ABG, COHb, lactate)
CHEMICAL ASPHYXIANT (CO/HCN/H₂S suspected)?
├── CO → 100% O₂ ± HBO
├── HCN → Hydroxocobalamin 5 g IV (first-line)
│ If no CO co-exposure: cyanide antidote kit acceptable
└── H₂S → 100% O₂; sodium nitrite if severe + within minutes
PULMONARY IRRITANT (Cl₂/phosgene/NO₂/NH₃)?
├── O₂, humidification, bronchodilators
├── Bicarbonate nebulization (Cl₂, NH₃)
├── Corticosteroids (NO₂, phosgene)
└── Observe ≥24 h (phosgene/NO₂ — delayed edema)
Lab/Diagnostic Workup
- Co-oximetry: COHb, MetHb levels (pulse oximetry is unreliable for CO/MetHb)
- ABG + lactate: Lactate >8–10 mmol/L → chemical asphyxiant until proven otherwise
- ECG: Arrhythmias, ischemia (CO, cyanide)
- Chest X-ray: Pulmonary edema, infiltrates
- Whole-blood cyanide: Confirmatory, not for acute management decisions
Disposition
| Severity | Disposition |
|---|---|
| Mild symptoms, resolved | Observe ≥4–6 h (24 h for phosgene/NO₂); discharge if clear |
| Significant exposure | Admit for monitoring |
| Severe (coma, arrest, acidosis) | ICU; consider HBO for CO/dual CO+CN |
| Pregnant patients with CO | Lower threshold for HBO |
Sources: Tintinalli's Emergency Medicine, pp. 1361–1365 | Rosen's Emergency Medicine, pp. 3001–3003 | Goldman-Cecil Medicine, p. 972 | Murray & Nadel's Respiratory Medicine
44yr old male with diziness and 1 episode of vomiting BP-170/110 and rbs-126 while lying down he is fine but not able to sit or stand
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have all the content needed for a comprehensive clinical answer. Let me now synthesize.
Clinical Assessment: 44M — Dizziness + Vomiting + BP 170/110
Reading the Clinical Picture
| Feature | Interpretation |
|---|---|
| Positional pattern — fine when lying, symptomatic sitting/standing | Strongly suggests vestibular origin (not pre-syncope — that worsens supine→standing due to orthostatic fall, but this patient is worse upright in any position, suggesting head-position-dependent vestibular activation) |
| Dizziness + 1 episode vomiting | Characteristic vestibular autonomic response |
| BP 170/110 | Significant hypertension — may be pre-existing, stress-reactive, or rarely the cause |
| RBS 126 mg/dL | Mildly elevated fasting or borderline post-prandial — note for metabolic risk but not acutely causative here |
| Age 44M | Must exclude posterior circulation stroke |
Most Likely Diagnosis
Peripheral Vertigo — most probable
The positional nature (worse with any upright/movement, relief lying still) and the pattern of nausea/vomiting with preserved consciousness and no focal neurological deficit point to a peripheral vestibular cause.
Top two differentials:
| Feature | BPPV | Vestibular Neuritis |
|---|---|---|
| Duration of each episode | <30–60 seconds, triggered by specific head movements | Constant vertigo for hours to days |
| Onset | Episodic | Sudden, worsens over hours |
| Nausea/Vomiting | Present | Present, often severe |
| Hearing | Normal | Normal (labyrinthitis = + hearing loss) |
| Hallpike test | Positive (upbeat + torsional nystagmus) | Should NOT be done (may worsen symptoms) |
| Head impulse test (HIT) | Negative | Positive (corrective saccade) |
| Epley maneuver | Highly effective | Ineffective |
| Recurrence | Frequent | Rare (2–11%) |
| Viral prodrome | Absent | Sometimes present |
If single episode with brief vertigo per movement: BPPV most likely If onset was acute and constant for hours/days: Vestibular neuritis more likely
Cannot Miss: Central Causes — Must Exclude
With BP 170/110 + age 44 + vomiting, the following red flags must be actively sought:
| Diagnosis | Red Flag Features |
|---|---|
| Cerebellar hemorrhage/infarction | Sudden severe headache, true truncal ataxia (unable to sit unsupported), dysmetria |
| Vertebrobasilar insufficiency (VBI)/TIA | Diplopia, dysarthria, dysphagia, facial numbness, limb weakness, Horner syndrome |
| Posterior inferior cerebellar artery occlusion (Wallenberg syndrome) | Loss of pain/temperature sensation on face (ipsilateral) + body (contralateral), hoarseness, ataxia, Horner |
| Hypertensive emergency with CNS involvement | BP >180/120 + altered sensorium, focal deficits, papilledema |
The HINTS exam (Head Impulse, Nystagmus, Test of Skew) is the bedside gold standard to separate peripheral from central:
- Peripheral (benign): Abnormal HIT + unidirectional nystagmus + no skew deviation
- Central (dangerous): Normal HIT + direction-changing nystagmus + skew deviation → get MRI immediately
Examination Priorities
- Neurological exam: Cerebellar signs — finger-nose test, heel-shin, gait (if safe), tandem walk
- Cranial nerves: CN III–VIII, especially ocular movements, facial sensation, hearing
- HINTS exam at bedside
- Fundoscopy: Papilledema (hypertensive emergency)
- Nystagmus character: Direction, fatigability, spontaneous vs. positional
- Blood pressure both arms: Vertebrobasilar pathology can cause asymmetry
Investigations
| Investigation | Rationale |
|---|---|
| Non-contrast CT Brain | Exclude cerebellar/brainstem hemorrhage (initial, fast) |
| MRI Brain + MRA posterior fossa | Gold standard for posterior circulation ischemia — more sensitive than CT for posterior fossa lesions; obtain if CT negative but central features suspected |
| ECG | Screen for arrhythmia as dizziness cause |
| FBS/HbA1c | RBS 126 — evaluate for diabetes |
| Renal function, urinalysis | Hypertension workup |
| CBC, electrolytes | Rule out anemia, hyponatremia |
| Audiometry | If hearing loss suspected (labyrinthitis vs. neuritis) |
Management
Immediate
- Keep patient supine — already their comfort position; avoid unnecessary position changes
- IV access, monitoring (BP, HR, SpO₂)
- Reassess BP after 15–20 min rest (white-coat/pain effect may account for some elevation)
Symptomatic Relief (Vestibular Suppressants)
| Drug | Dose | Notes |
|---|---|---|
| Promethazine 25 mg IM/IV | Most effective for vomiting | Sedating; useful acutely |
| Metoclopramide 10 mg IV | For nausea/vomiting | Less sedating |
| Meclizine (Antivert) 25–50 mg PO | Vestibular suppressant | Onset ~1 hour; not useful acutely IV |
| Diazepam 2–5 mg IV/IM | Vestibular suppression | Benzodiazepines not recommended for vestibular neuritis long-term; short-term only |
| Prochlorperazine 10 mg IV | Antiemetic | Good for acute vestibular symptoms |
Avoid long-term vestibular suppressants in vestibular neuritis — they delay central compensation.
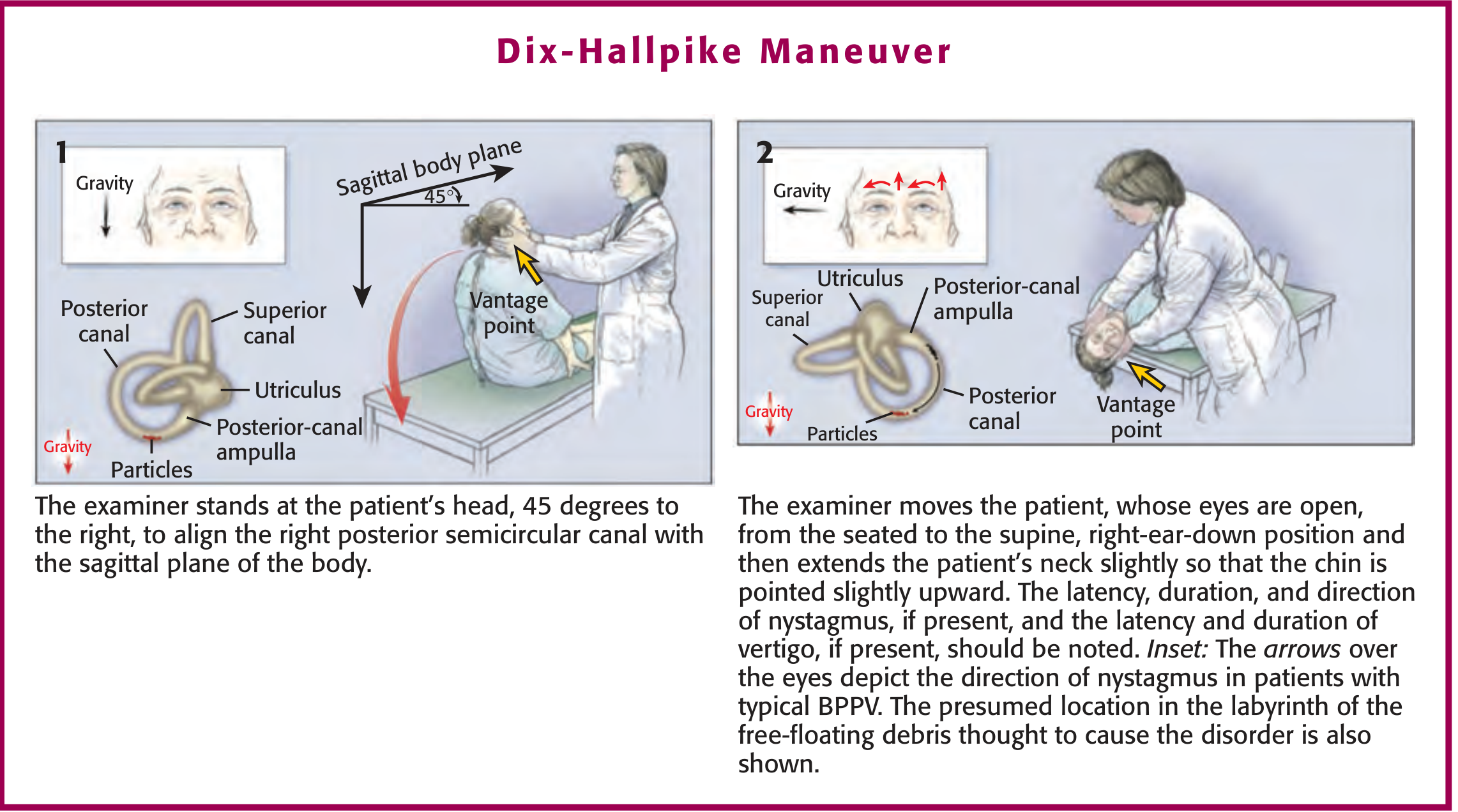
If BPPV confirmed (positive Hallpike):
Epley Maneuver — highly effective bedside repositioning treatment; resolves symptoms in ~80% immediately or within days.
Hypertension Management
- Do not aggressively lower BP acutely without evidence of end-organ damage — rapid reduction in a patient with posterior circulation compromise can worsen ischemia
- If hypertensive emergency confirmed (BP >180/120 + end-organ damage): controlled IV reduction by ~20–25% in first hour
- If no emergency: oral antihypertensive (amlodipine, ARB, or ACE-I) and outpatient follow-up
Summary: Immediate Action Plan
1. Lie patient supine → symptom relief confirms vestibular, not cardiovascular cause
2. Full neuro exam + HINTS bedside exam
3. IV access → antiemetic (metoclopramide or promethazine)
4. CT brain to exclude hemorrhage
5. ECG
6. BP recheck after 20 min rest
7. If CT normal + HINTS peripheral → Dix-Hallpike → Epley if BPPV confirmed
8. If ANY central features → urgent MRI + neurology consult
9. RBS 126 → check HbA1c, fasting glucose; refer for diabetic/hypertensive workup
10. Discharge only after ambulation tolerated and symptoms significantly improved
Bottom line: This patient most likely has BPPV or vestibular neuritis but is a 44-year-old hypertensive male — posterior circulation stroke must be excluded before assuming a benign peripheral cause. — Rosen's Emergency Medicine, p. 187–191
This is a shared conversation. Sign in to Orris to start your own chat.