Heart bipass sergery
Reading File
Finding Sources
Finding Sources
Searching the Web
heart bypass surgery CABG procedure overview 2024
Reading File
Reading File
Searching PubMed
"coronary artery bypass grafting" outcomes
Loading Image
Reading File
Here is a thorough overview of heart bypass surgery (CABG) based on major surgical and cardiology textbooks.
Heart Bypass Surgery (Coronary Artery Bypass Grafting - CABG)
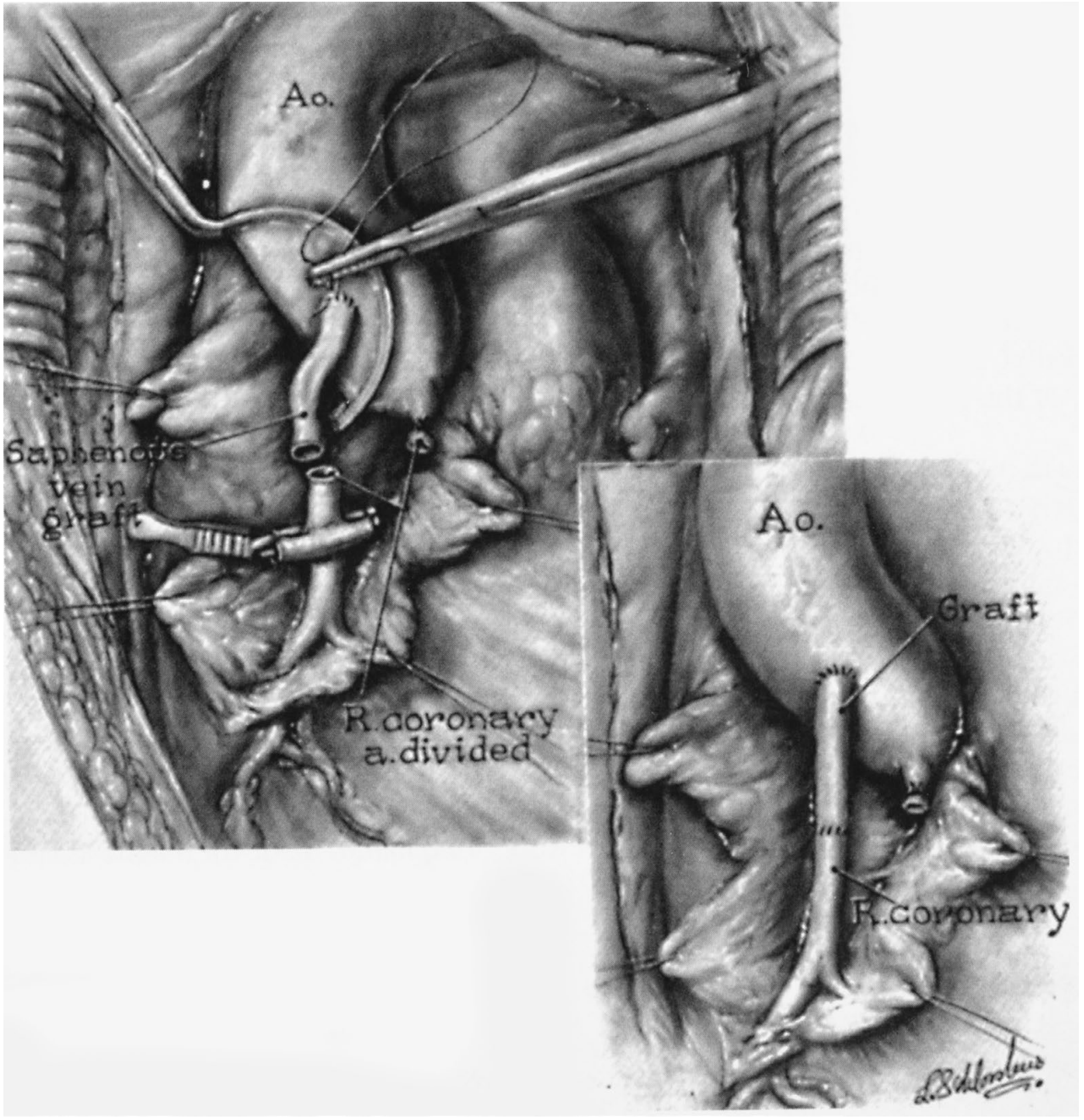
Classic CABG illustration showing the saphenous vein graft connected from the aorta (Ao.) to the right coronary artery - Sabiston Textbook of Surgery
What Is It?
Coronary artery bypass grafting (CABG) is open-heart surgery designed to restore blood flow to the heart muscle when one or more coronary arteries are significantly narrowed or blocked by atherosclerosis. A healthy blood vessel (graft) is taken from elsewhere in the body and used to create a detour (bypass) around the blocked segment.
Why Is It Done?
The heart muscle depends entirely on the coronary arteries for oxygen. When these arteries become blocked by cholesterol plaques, the heart muscle becomes starved of blood - causing angina (chest pain) at first, and a heart attack if the blockage is complete.
CABG is indicated when:
- Medications and lifestyle changes no longer control angina
- There is significant obstruction of the left main coronary artery
- There is three-vessel disease (all three major coronary arteries blocked)
- There is two-vessel disease with significant involvement of the proximal left anterior descending (LAD) artery
- The left ventricular ejection fraction is reduced (EF <35%)
- The patient has diabetes mellitus with multivessel coronary disease - in this group, CABG is superior to stenting (PCI) for preventing death, heart attack, and repeat procedures
- The patient cannot take dual-antiplatelet therapy (required after stenting)
(Harrison's Principles of Internal Medicine 22E, p. 575-598; Sabiston Textbook of Surgery)
The Graft Conduits (Bypass Vessels)
The surgeon must harvest a vessel to use as the new "pipe." There are three main options:
| Conduit | Source | Patency (long-term) |
|---|---|---|
| Internal mammary artery (IMA) | Inside chest wall | Best - preferred choice |
| Radial artery | Forearm | Very good |
| Saphenous vein | Leg | Good short-term; 10-20% occlude in year 1, then ~2-4%/year thereafter |
The left internal mammary artery (LIMA) to LAD anastomosis is the gold standard. Survival is significantly better with arterial grafts than with saphenous vein grafts for the LAD. A 2025 meta-analysis (PMID 40695535) confirmed that "no-touch" harvesting of the saphenous vein further improves long-term patency.
Types of CABG
1. On-Pump CABG (Traditional)
- The heart is stopped and the patient is placed on a cardiopulmonary bypass (CPB) machine (heart-lung machine), which oxygenates and circulates blood during surgery.
- Provides a still, bloodless field for precise sewing.
- Associated with some risk of neurological complications from the bypass circuit.
2. Off-Pump CABG (Beating Heart Surgery)
- Surgery is performed on the beating heart without CPB.
- Reduces some complications related to the bypass circuit.
- A 2024 meta-analysis (PMID 38626442) found comparable overall outcomes between on-pump and off-pump techniques, with some advantages in specific patient subgroups.
3. Minimally Invasive CABG
- Performed through a small thoracotomy (a limited chest opening) rather than a full sternotomy.
- Can shorten recovery time and reduce morbidity in suitable patients.
- Total endoscopic approaches are also available in specialized centers.
The Surgical Steps (Overview)
- Anesthesia and monitoring lines are placed.
- The surgeon makes a median sternotomy (splitting the breastbone) to access the heart.
- The graft vessel is harvested (LIMA is taken off the chest wall; saphenous vein is taken from the leg).
- For on-pump surgery, the patient is connected to the heart-lung bypass machine and the heart is stopped with a cold cardioplegia solution.
- The graft is sewn (anastomosed) to the coronary artery beyond the blockage, and the other end is attached to the aorta (or left as the LIMA pedicle).
- The heart is restarted, the bypass machine is disconnected.
- The chest is closed with sternal wires and sutures.
Outcomes
- Mortality: Less than 1% in low-risk patients with normal heart function, operated by an experienced team. Rises significantly with age >80, poor heart function, and multiple comorbidities.
- Angina relief: Abolished or greatly reduced in approximately 90% of patients after complete revascularization.
- Survival benefit: Proven in left main disease, three-vessel disease, reduced ejection fraction, and diabetics with multivessel disease.
- Graft failure: Saphenous vein grafts occlude in 10-20% within the first year; arterial grafts last considerably longer. Risk factor control (especially cholesterol management) improves graft patency.
- Cardiac rehabilitation post-CABG, including in elderly patients, improves recovery and outcomes - supported by a 2025 systematic review (PMID 41299466).
(Harrison's Principles of Internal Medicine 22E; Sabiston Textbook of Surgery)
CABG vs. Stenting (PCI)
CABG is generally preferred over percutaneous coronary intervention (PCI/stenting) in:
- Left main coronary artery disease
- Three-vessel disease with complex anatomy (high SYNTAX score)
- Diabetics with multivessel disease
- Patients with poor LV function
- Patients who cannot tolerate prolonged antiplatelet therapy
- Recurrent in-stent restenosis
PCI is preferred for simpler, lower-risk anatomy and patients who are poor surgical candidates.
(Based on 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization)
Risks and Complications
- Bleeding and the need for transfusion
- Stroke (especially in older patients or those with aortic disease)
- Atrial fibrillation (very common post-operatively, usually temporary)
- Wound infection (superficial or deep sternal wound infection)
- Kidney injury
- Delirium - occurs in 3-35% of patients after CABG
- Graft occlusion and recurrence of symptoms over time
- Heart attack perioperatively (Type 5 MI)
Recovery
- Hospital stay: typically 5-7 days
- Return to light activity: 4-6 weeks
- Full recovery: 2-3 months
- Cardiac rehabilitation is strongly recommended and has been shown to improve outcomes, including in elderly patients
Key sources: Harrison's Principles of Internal Medicine 22E; Sabiston Textbook of Surgery (Elsevier); Bailey and Love's Short Practice of Surgery 28th Ed; Cleveland Clinic CABG overview; Johns Hopkins Medicine
This is a shared conversation. Sign in to Orris to start your own chat.