Forniers gangrene
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Fournier gangrene"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a complete overview of Fournier's Gangrene:
Fournier's Gangrene
Definition
Fournier's gangrene (FG) is a polymicrobial, synergistic, necrotizing fasciitis of the perineal, genital, or perianal regions. It is a surgical emergency — rapidly progressive and potentially fatal if not treated immediately.
- Also called: idiopathic gangrene of the scrotum, streptococcal scrotal gangrene, perineal phlegmon
- Classically affects men (particularly 45–60 years), but women account for 10–25% of cases
Tintinalli's Emergency Medicine | Campbell-Walsh Urology | Sabiston Textbook of Surgery
Etiology & Pathogenesis
FG begins as a benign infection or abscess that becomes virulent, typically from three anatomic sources:
- Urogenital tract (urethral strictures, periurethral abscesses, urinary catheters)
- Anorectal (perirectal abscesses, fistulae)
- Cutaneous (trauma, surgical wounds)
Microbiology — polymicrobial with synergistic aerobic and anaerobic organisms:
- E. coli, Bacteroides spp., Streptococcus pyogenes, Staphylococcus aureus, Klebsiella, Clostridia, Corynebacteria
Mechanism: Bacterial infection causes microthrombosis of small subcutaneous vessels → tissue ischemia → gangrene of overlying skin. Infection spreads along fascial planes (Dartos, Colles', Scarpa's, Buck's fascia), often far beyond visible skin changes.
Clinical Image

Risk Factors
| Risk Factor | Prevalence |
|---|---|
| Diabetes mellitus | 32–66% of cases |
| Chronic alcohol abuse | 25–50% |
| Obesity | Common |
| Immunosuppression | Common |
| Cancer / malnutrition | Recognized |
| Peripheral vascular disease | Recognized |
| Advanced age | >60 years = increased mortality |
| SGLT-2 inhibitors | Emerging association (see below) |
Clinical Features
Early:
- Genital/perineal pain (65%), often with pruritus
- Prodrome of lethargy and fever (may be afebrile on arrival)
- Swelling (65%), erythema (35%)
Advanced (dramatic presentation):
- Crepitus — pathognomonic, due to gas-forming organisms
- Purple/black bullae, necrotic patches
- Foul odor, grayish skin cast
- Ecchymosis and skin ischemia
Key principle: Systemic signs (sepsis) are often out of proportion to the visible skin findings, because infection tracks deep along fascial planes. Pain out of proportion to visible extent should raise immediate suspicion.
Fascial Spread
- Urogenital sources → spread along Buck's and Dartos fascia → Colles' fascia; limited posteriorly at the perineal body
- Anorectal sources → perianal skin involvement
- Can extend to anterior abdominal wall, all the way to the clavicles
- Testes are usually spared — their blood supply originates intra-abdominally
Diagnosis
Primarily clinical. Imaging supports but must not delay surgical intervention.
CT scan (preferred):
- Soft-tissue air within deep fascia and associated fluid collections
- Delineates extent of disease
Bedside Ultrasound:
- Scrotal wall thickening
- "Dirty shadowing" — air within tissues
LRINEC Score (Laboratory Risk Indicator for Necrotizing Infection):
| Lab Parameter | Threshold | Points |
|---|---|---|
| C-reactive protein | >150 mg/L | 4 |
| WBC count | >15,000/μL | 1 (15k–25k) / 2 (>25k) |
| Hemoglobin | <13.5 g/dL | 1 (<11: 2) |
| Serum sodium | <135 mmol/L | 2 |
| Serum creatinine | >1.6 mg/dL | 2 |
| Serum glucose | >180 mg/dL | 1 |
Score ≥6 → positive predictive value 92%, negative predictive value 96% for necrotizing infection.
— Sabiston Textbook of Surgery
Treatment
FG is managed with a multimodal, aggressive approach:
1. Resuscitation
- Hemodynamic stabilization, aggressive IV fluid resuscitation
- ICU admission postoperatively
2. Broad-Spectrum Antibiotics (start immediately)
Coverage must include gram-positive, gram-negative, and anaerobic organisms:
| Regimen | Dose |
|---|---|
| Piperacillin-tazobactam | 3.375–4.5 g IV q6h |
| OR Imipenem | 1 g IV q24h |
| OR Meropenem | 500 mg–1 g IV q8h |
| Plus Vancomycin | (MRSA coverage) |
| ±Clindamycin | 600–900 mg IV q8h (toxin inhibition) |
| ±Metronidazole | 1 g IV load, then 500 mg IV q8h |
3. Surgical Debridement (cornerstone of management)
- Urgent, wide surgical debridement to margins of healthy, bleeding tissue
- Extent of disease is almost always far greater than external appearance suggests
- Average 3–4 return trips to the OR for serial debridement
- Second-look operation at 24–48 hours to exclude progression
- Testes can almost always be spared
- Fecal diversion (endorectal tubes, or colostomy if sphincter damaged) may be required
Intraoperative appearance:
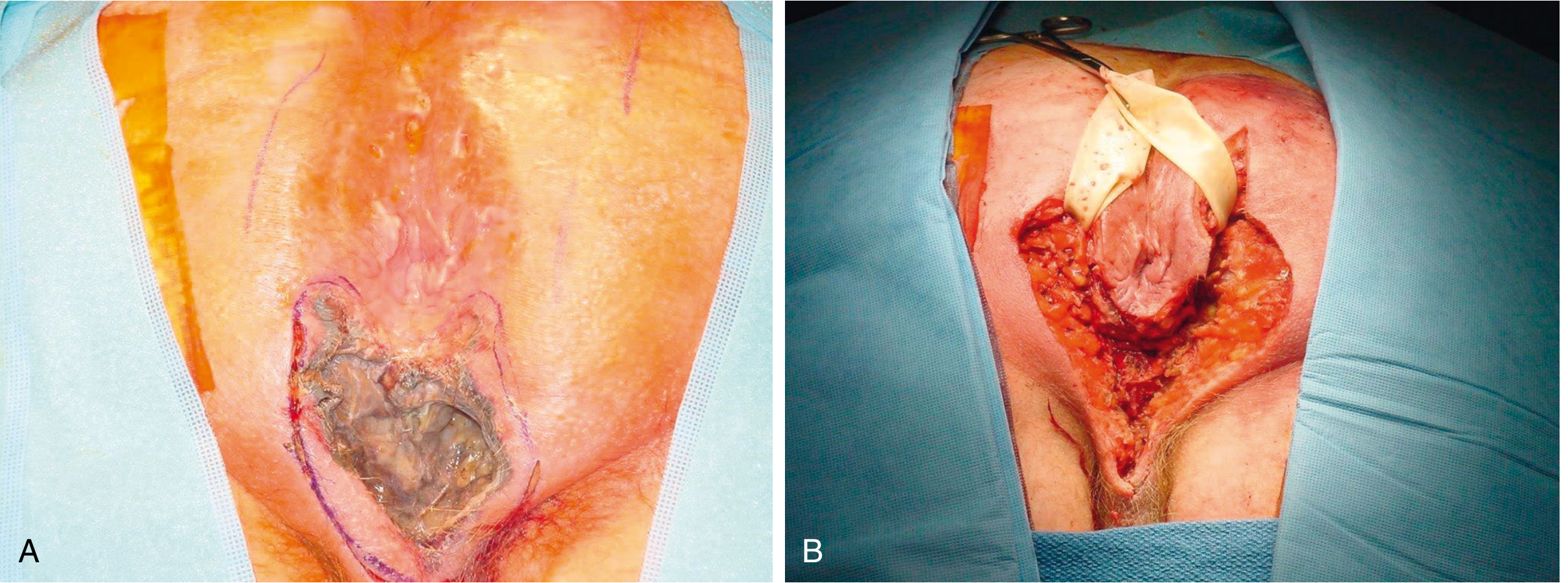
4. Wound Care & Reconstruction
- Negative pressure wound therapy (VAC) — reduces hospitalization, accelerates wound healing
- Split-thickness skin grafts for perineal/scrotal defects
- Flap reconstruction for large defects (systematic review: PMID 41720016)
5. Hyperbaric Oxygen (HBO)
- Adjunctive option — several groups report favorable results
- Does not improve overall mortality per Tintinalli; remains controversial
Prognosis & Mortality
- Historical mortality: 3–67%; contemporary estimates: 12–30%
- Age >60 and treatment complications are the most important predictors of death
- Survivors experience significant morbidity: sexual dysfunction ~65%, long-term disability
Prognostic Scoring Systems:
- Fournier's Gangrene Severity Index (FGSI)
- Ulludag FG Severity Index
- Age-Adjusted Charlson Comorbidity Index (ACCI)
- Surgical Apgar Score (sAPGAR) All validated to predict mortality and guide therapeutic aggressiveness.
Special Consideration: SGLT-2 Inhibitors
A 2025 systematic review (PMID 39871381) examined the association between SGLT-2 inhibitors (e.g., empagliflozin, canagliflozin, dapagliflozin) and Fournier's gangrene. The FDA issued a safety warning in 2018 linking this drug class to FG — an important consideration in diabetic patients presenting with perineal infections.
Sources: Sabiston Textbook of Surgery, Schwartz's Principles of Surgery, Campbell-Walsh Urology, Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.