I have sufficient information to write a comprehensive answer. Let me now compose the full structured response.
Clinical Case Analysis: 54-Year-Old Male with Obstructive Jaundice + Palpable Gallbladder
DIAGNOSIS
Periampullary Carcinoma (most likely Carcinoma of the Head of Pancreas)
This case is a classic presentation. The triad of:
- Persistently and progressively deepening jaundice (obstructive, not fluctuating)
- Palpable, non-tender, soft cystic gallbladder - this is Courvoisier's Law (positive)
- Significant constitutional features - anorexia, gross weight loss
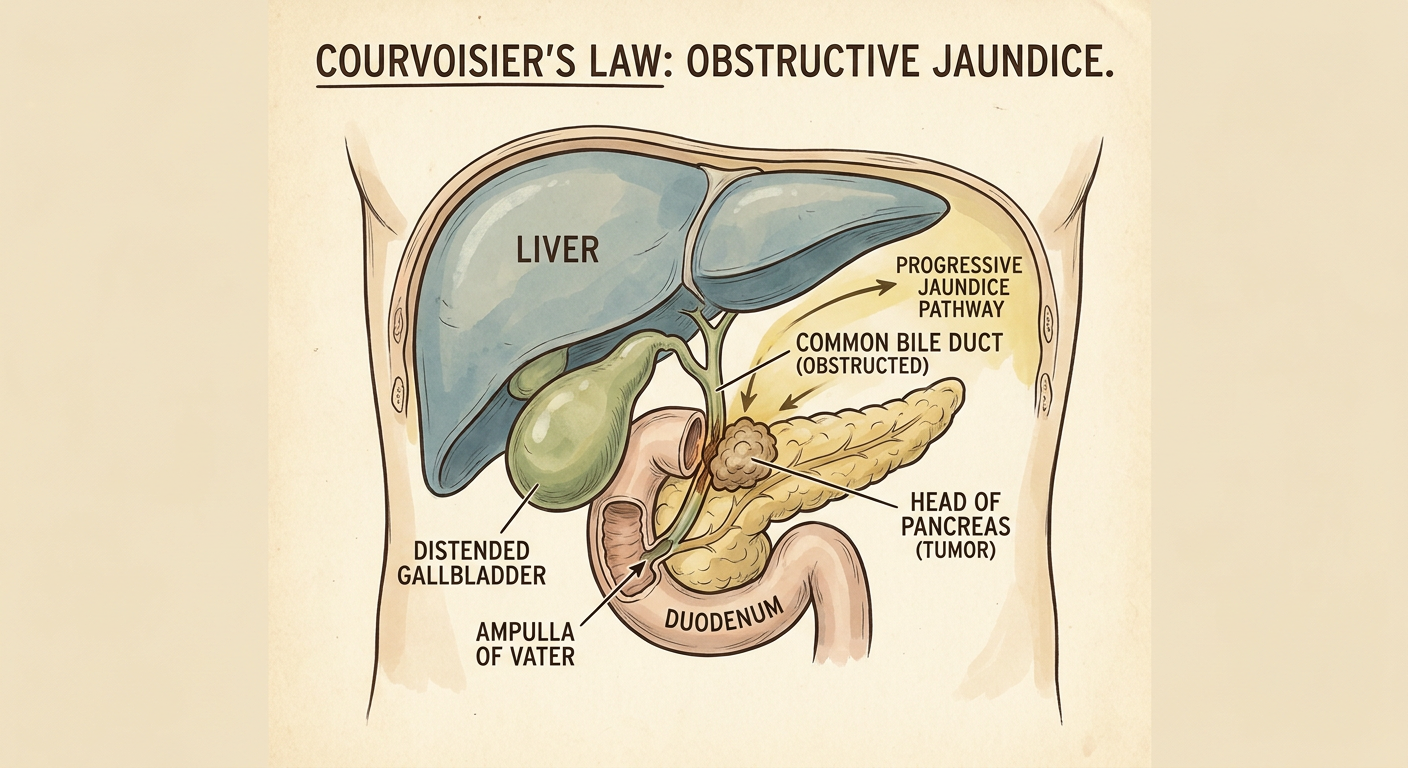
...strongly points to a malignant obstruction of the lower end of the common bile duct, most likely carcinoma of the head of pancreas or another periampullary tumour. The intermittent fever with chills and rigors indicates ascending cholangitis superimposed on biliary obstruction.
Courvoisier's Law: "If the gallbladder is palpable and the patient is jaundiced, the obstruction of the bile duct is unlikely to be due to a stone." This is because chronic cholelithiasis causes a fibrosed, thickened, non-distensible gallbladder - whereas a neoplastic obstruction occurring in a previously normal gallbladder allows it to dilate passively.
DIAGRAM 1: Anatomy of the Lesion - Courvoisier's Law
PART 1: DETAILED WORK-UP (5 Marks)
A. History (detailed points)
- Duration, onset, progression of jaundice - whether painless or painful
- Nature of pain - dull aching (pancreatic cancer) vs colicky (stone)
- Colour of stools (pale/clay-coloured = obstructive) and urine (dark = conjugated bilirubin)
- Pruritus (bile salts in skin)
- Symptoms of cholangitis: Charcot's triad (pain + fever + jaundice) or Reynold's pentad
- Weight loss quantification and time frame
- Past history of gallstones, pancreatitis, alcohol, smoking
- Family history of pancreatic malignancy
B. Clinical Examination
- Icterus severity - scleral, skin, mucous membranes
- Confirm: Non-tender, soft, cystic, palpable gallbladder (Courvoisier's sign)
- Hepatomegaly (smooth, tender - suggests biliary obstruction; nodular - liver secondaries)
- Splenomegaly (portal hypertension)
- Ascites (peritoneal deposits)
- Virchow's node (left supraclavicular lymphadenopathy - Sister Mary Joseph nodule)
- Cachexia, muscle wasting
C. Investigations
Routine (Pre-op preparation):
| Investigation | Purpose |
|---|
| CBC | Anaemia, leucocytosis (cholangitis) |
| Blood group & cross-match | Surgical preparation |
| Serum electrolytes, urea, creatinine | Renal function |
| Blood glucose | Pancreatic endocrine function |
| Coagulation profile (PT, INR, aPTT) | Obstructive jaundice impairs Vit K absorption |
| Serum proteins & albumin | Nutritional status, hepatic synthetic function |
| Urine R/M + bile salts/pigments | Confirm obstructive jaundice |
| ECG, Chest X-Ray | Cardiac assessment for anaesthesia |
Liver Function Tests (LFTs):
- Total & direct bilirubin - markedly raised, predominantly direct (conjugated)
- Alkaline phosphatase - very high (marker of biliary obstruction)
- GGT - elevated
- AST/ALT - mildly elevated (secondary hepatocellular damage)
- Serum albumin - may be reduced
Imaging Workup:
| Investigation | Findings Expected |
|---|
| USG abdomen (1st line) | Dilated CBD, dilated intrahepatic ducts, distended GB, mass in head of pancreas |
| CECT abdomen (triple phase) | Characterize tumour, assess resectability (involvement of portal vein, SMA) |
| MRCP | Non-invasive - shows level of obstruction, relation to ducts |
| ERCP | Diagnostic + therapeutic - brush cytology, stent placement |
| EUS (Endoscopic USG) | Best for staging small tumours, FNA biopsy |
| PET scan | Detect metastases |
Tumour Markers:
- CA 19-9 - primary marker for pancreatic carcinoma (sensitivity ~80%)
- CEA - less specific but useful
- AFP, CA-125 if cholangiocarcinoma considered
PART 2: PREPARATION FOR GENERAL ANAESTHESIA (5 Marks)
This patient has obstructive jaundice which creates specific preoperative challenges:
1. Correct Coagulopathy
- Obstructive jaundice prevents fat-soluble vitamin (especially Vitamin K) absorption
- Give Vitamin K 10 mg IM/IV for 3-5 days; monitor PT/INR and correct to within 2 seconds of normal
- Fresh Frozen Plasma (FFP) if urgent correction needed
2. Relieve Jaundice Preoperatively
- Biliary decompression before major surgery reduces hepatorenal complications:
- Endoscopic biliary stenting (ERCP-guided) - preferred
- Percutaneous Transhepatic Biliary Drainage (PTBD) if ERCP fails
- Target: Bring bilirubin < 10 mg/dL before surgery
3. Prevent Hepatorenal Syndrome
- Obstructive jaundice causes renal tubular toxicity from bile salts
- IV fluid hydration: adequate preoperative hydration with Normal Saline
- Monitor urine output (target >0.5 mL/kg/hr)
- Mannitol infusion intraoperatively (10% mannitol 200 mL IV) to maintain renal tubular flow
- Avoid nephrotoxic drugs (NSAIDs, aminoglycosides)
4. Nutritional Optimization
- Patient has gross weight loss and anorexia
- Correct with high-protein, high-calorie diet or parenteral nutrition if necessary
- Correct anaemia if Hb < 10 g/dL (packed red cell transfusion)
- Correct hypoalbuminemia (albumin infusion if <2.5 g/dL)
5. Treat Cholangitis
- Broad-spectrum IV antibiotics (covering gram-negative enterics and anaerobes):
- Piperacillin-tazobactam, or
- Cephalosporin + Metronidazole
- Start 48-72 hours preoperatively
6. Specific Anaesthetic Considerations
- Blood cross-matching (major blood loss expected in Whipple's)
- Glucose monitoring (pancreatic endocrine insufficiency)
- Avoid halothane (hepatotoxic) - prefer isoflurane/sevoflurane
- Central line + arterial line for monitoring
- Epidural analgesia setup for postoperative pain
7. Consent & Counselling
- Explain diagnosis, prognosis, surgical risk
- High-risk patient: jaundice + malnutrition + age 54
PART 3: OUTLINE OF TREATMENT (5 Marks)
A. CURATIVE TREATMENT
Whipple's Pancreaticoduodenectomy (Pancreaticoduodenectomy)
- Standard operation for resectable carcinoma of head of pancreas / periampullary carcinoma
- Resects: Head of pancreas + duodenum + lower CBD + gallbladder + antrum of stomach (classic Whipple's) or with pylorus preservation
- Reconstruction: Pancreaticojejunostomy + Hepaticojejunostomy + Gastrojejunostomy
- Resectability criteria: No involvement of portal vein, SMA, or distant metastases
- Only ~15-20% of pancreatic cancers are resectable at presentation
Adjuvant therapy post-surgery:
- Gemcitabine-based chemotherapy
- Chemoradiotherapy in selected cases
B. PALLIATIVE TREATMENT
When the tumour is unresectable (majority of cases), palliation aims to:
- Relieve obstructive jaundice
- Relieve gastric outlet obstruction
- Relieve pain
| Palliative Procedure | Purpose | Method |
|---|
| Choledochojejunostomy | Biliary bypass | Surgical - connect CBD proximal to obstruction to jejunum |
| Hepaticojejunostomy | Biliary bypass | If CBD involved |
| Endoscopic biliary stenting | Non-surgical jaundice relief | ERCP-guided plastic or metal stent |
| PTBD | Biliary drainage | Radiological, if ERCP not possible |
| Gastrojejunostomy | Prevent duodenal obstruction | Surgical bypass of impending duodenal block |
| Chemical splanchnicectomy | Pain relief | 50% ethanol injection into coeliac ganglia (at surgery or CT-guided) |
| Opioid analgesics | Pain control | Morphine/Fentanyl patches |
| Palliative chemo | Tumour control | Gemcitabine ± nab-paclitaxel |
| Radiotherapy | Tumour control | EBRT to primary |
| Nutritional support | General palliation | Pancreatic enzyme supplements, PEG feeding |
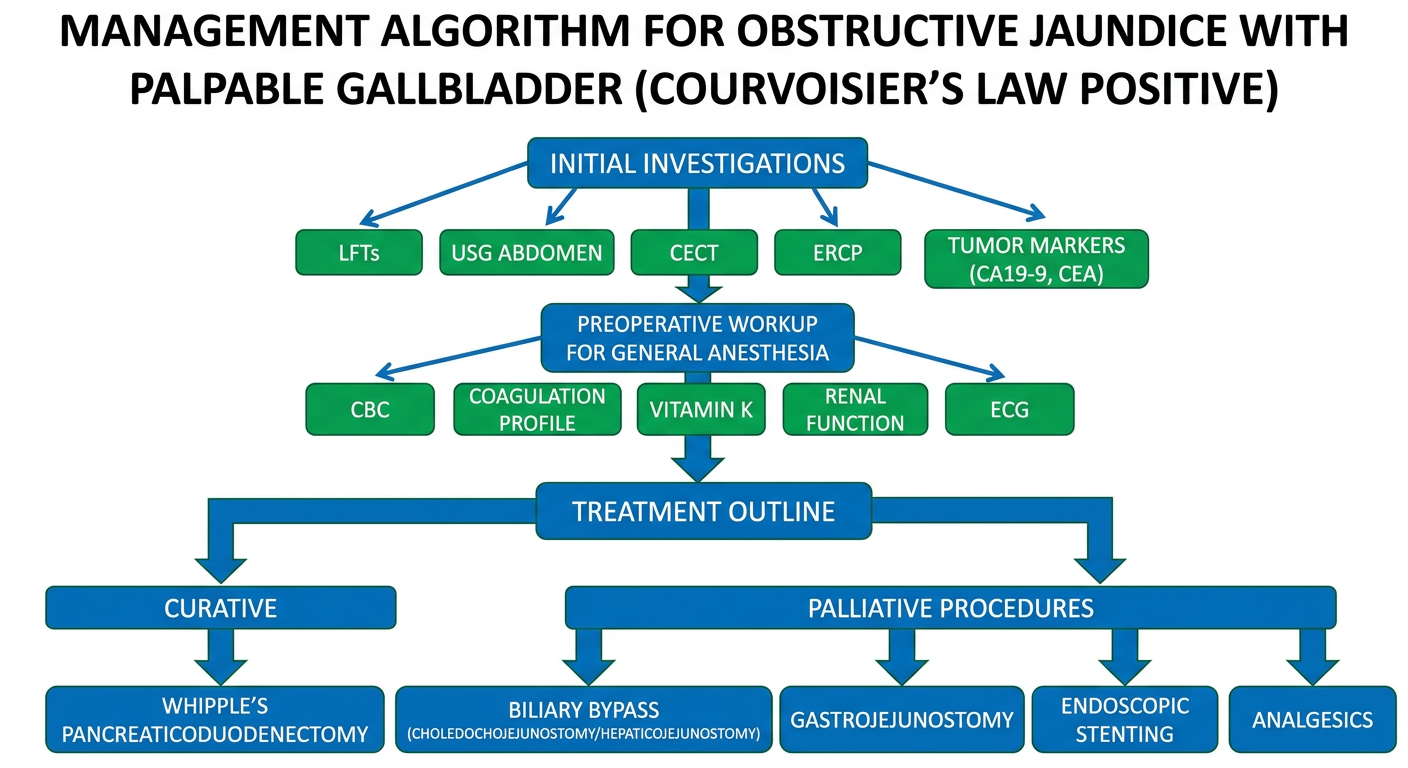
DIAGRAM 2: Management Algorithm
SUMMARY TABLE
| Feature | This Patient | Significance |
|---|
| Painless progressive jaundice x 4 months | Yes | Malignant obstruction |
| Palpable non-tender gallbladder | Yes | Courvoisier's sign positive |
| Fever, chills, rigors x 15 days | Yes | Ascending cholangitis |
| Anorexia + gross weight loss | Yes | Malignant cachexia |
| Age 54, male | Yes | High-risk group for periampullary Ca |
Most likely diagnosis: Carcinoma of the head of pancreas (periampullary carcinoma)
Key points to remember for the exam:
- This is a 5+5+5 = 15 mark question requiring equal depth in workup, pre-op prep, and treatment
- Always mention Courvoisier's law in the diagnosis
- Preoperative correction of Vitamin K / coagulopathy is the most frequently tested step
- Whipple's procedure = curative; biliary bypass + stenting = palliative
- Palliation addresses three problems: jaundice, duodenal obstruction, and pain