Anemia in acute loss
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Here is the full response:
Anemia Due to Acute Blood Loss (Posthemorrhagic Anemia)
Sources: Harrison's Principles of Internal Medicine 22E (2025), Frameworks for Internal Medicine, Goldman-Cecil Medicine
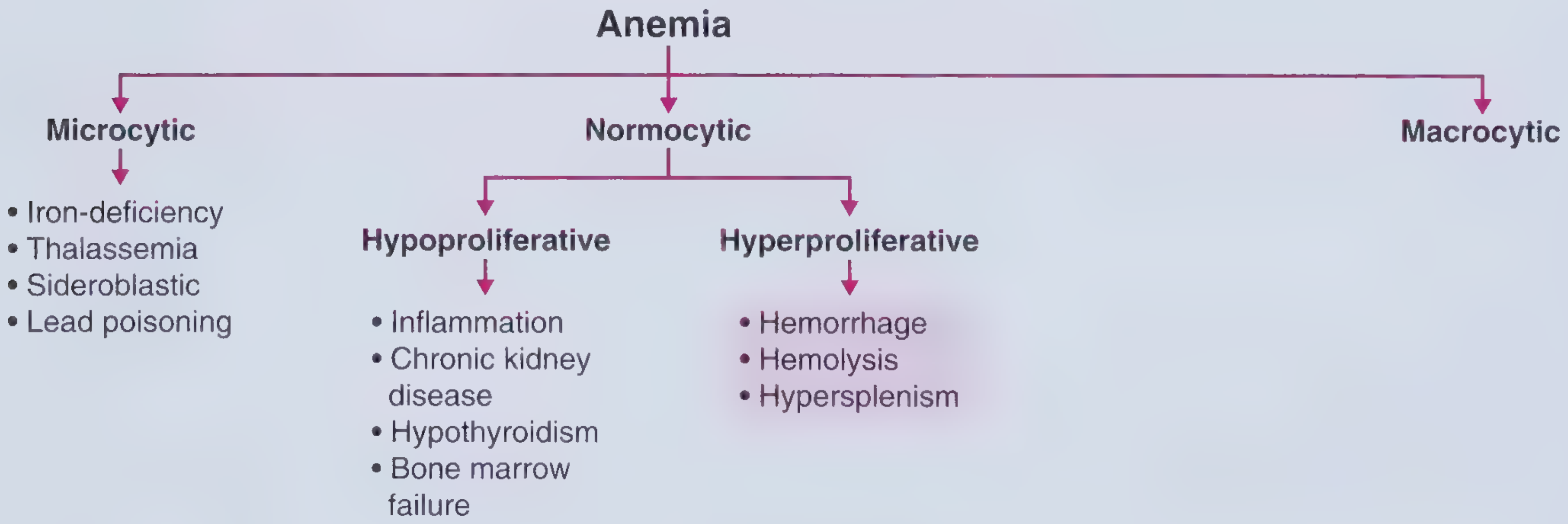
Classification Context
Acute blood loss anemia is classified as normocytic, hyperproliferative anemia - the bone marrow responds actively to replace lost red cells.
Mechanisms of Anemia
Blood loss causes anemia by two main mechanisms:
- Direct loss of red cells - the acute posthemorrhagic type (covered here)
- Gradual depletion of iron stores - if loss is protracted, leading to iron-deficiency microcytic anemia
Three Clinical/Pathophysiologic Stages
Stage 1 - Hypovolemia (Immediate)
- The dominant feature is hypovolemia, not yet anemia
- Organs with high blood supply (brain, kidneys) are most threatened - loss of consciousness and acute renal failure are major risks
- Key point: A blood count at this stage will NOT show anemia - hemoglobin concentration is unchanged because plasma and red cells are lost proportionally
- Only after IV fluids are given does the Hb begin to fall over several hours
- Physical exam findings reflect sympathetic activation: tachycardia, tachypnea, decreased pulse pressure, cold/pale/mottled skin, decreased urine output
Stage 2 - Hemodilution (Hours later)
- Baroreceptors and stretch receptors trigger release of vasopressin and other peptides
- The body shifts fluid from the extravascular to intravascular compartment, producing hemodilution
- Hypovolemia gradually converts to dilutional anemia
- The hemoglobin now reflects the amount of blood lost. For example: if Hb = 7 g/dL at 3 days, approximately half of total blood volume was lost
Stage 3 - Bone Marrow Response (Days to weeks)
- Provided bleeding stops, the marrow gradually corrects the anemia
- Reticulocyte count and erythropoietin levels become elevated (hyperproliferative response)
- This is physiologically identical to the marrow response seen in hemolysis
Clinical Features by Volume Lost
| Blood Loss | % of Total Volume | Clinical Features |
|---|---|---|
| Mild | < ~15% (1 unit donation) | Usually asymptomatic; enhanced O₂ delivery via Bohr effect (decreased pH / increased CO₂) |
| Moderate | Up to 30% | Tachycardia, tachypnea; blood pressure typically normal or mildly decreased |
| Severe | > 30% | Orthostatic hypotension progressing to hypotensive shock; dyspnea, diaphoresis, cold/clammy skin, decreased urine output, delayed capillary refill |
- Healthy young adult men (~30s): ~6 L total blood volume
- By the 7th decade: ~5 L total blood volume
Symptoms of the Resulting Anemia
Symptoms of the anemia itself (once it develops) depend on how quickly it develops:
- Rapid onset: fatigue, loss of stamina, breathlessness, tachycardia (especially on exertion)
- Gradual onset: young patients may tolerate Hb as low as 7-8 g/dL before symptoms, due to:
- Rightward shift of O₂-Hb dissociation curve (increased 2,3-BPG)
- Increased cardiac output and regional blood flow redistribution
- Blood shunted away from kidney, gut, and skin to protect brain and heart
- Compensatory mechanisms can cover a 2-3 g/dL Hb deficit
Diagnosis
- Usually straightforward with external or obvious bleeding
- Internal bleeding (GI, retroperitoneal, ectopic pregnancy, subarachnoid, aneurysm) may not be immediately obvious
- Never underestimate internal losses - blood loss at the scene is often overestimated visually
- Physical signs to localize:
- Grey Turner sign (flank ecchymosis) - retroperitoneal bleeding
- Cullen sign (umbilical ecchymosis) - intraperitoneal or retroperitoneal bleeding
- Dullness to chest percussion - intrapleural bleeding
- When an abrupt Hb fall occurs, always suspect acute posthemorrhagic anemia (APHA)
- Investigations: sonogram, endoscopy as appropriate
Treatment
Priority order:
- ABCs - Airway, Breathing, Circulation in hemodynamically unstable patients; vasopressors for bleeding-associated hypotension
- Blood transfusion - Unlike chronic anemias, the body is NOT adapted, so transfusion takes priority early
- Stop the hemorrhage - eliminate the source concurrently
Volume replacement:
- Plasma is preferred over saline for volume expansion in acute hemorrhage - crystalloid dilutes clotting factors and can worsen hemostasis
- Trauma also causes vascular and platelet abnormalities that further increase bleeding risk
Surgical blood loss:
- Can be substantial (e.g., up to 2 L in radical prostatectomy)
- Elective surgery: preoperative autologous blood donation may be available
Blood substitutes (experimental):
- Two approaches: fluorocarbon synthetic chemicals and hemoglobin-based oxygen carriers (HBOCs)
- HBOCs have reached phase 2-3 trials but no blood substitute has yet become standard treatment
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 106 - Dan L. Longo
- Frameworks for Internal Medicine, Chapter on Normocytic Hyperproliferative Anemia
- Goldman-Cecil Medicine, Chapter 144 (Normocytic Anemias)
This is a shared conversation. Sign in to Orris to start your own chat.