Hcl acid poision consumption management for 24 yr old male pt
Reading File
Finding Sources
Finding Sources
Searching PubMed
"corrosive ingestion" AND "acid" AND management
Finding Sources
Finding Sources
Searching the Web
HCl hydrochloric acid poisoning ingestion management emergency treatment protocol 2024
Finding Sources
Reading Web Page
https://wwwn.cdc.gov/tsp/MMG/MMGDetails.aspx?mmgid=758&toxid…
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to provide a full clinical management guide. Let me compile the final response.
HCl (Hydrochloric Acid) Poisoning - Management in a 24-Year-Old Male
HCl is a strong acid (pH <2) that causes coagulative necrosis - it is one of the most severe caustic ingestions. In adults, ingestion is usually intentional (suicidal), meaning larger volumes are typically consumed than in accidental pediatric cases, leading to worse outcomes. ICU transfer is warranted for pure HCl ingestion regardless of volume.
Pathophysiology
- Acid causes coagulative necrosis with vascular thrombosis, creating an eschar that somewhat limits depth of penetration (vs. alkali liquefactive necrosis)
- Primarily damages the stomach (especially antrum) more than the esophagus - unlike alkali which mainly damages the esophagus
- HCl dissociates into H⁺ and Cl⁻; results in a non-anion gap metabolic acidosis (because both ions contribute to the anion gap measurement)
- Risk of gastric perforation > esophageal perforation compared with alkali
- 2024 retrospective cohort data (Br J Anaesth): HCl accounts for ~20% of ICU caustic admissions and is among the highest-severity agents
Immediate Pre-Hospital / First Aid
| Step | Action |
|---|---|
| Airway | Keep upright; prepare for vomiting during transport |
| Do NOT | Induce vomiting - absolute contraindication (re-exposes esophagus + risk of perforation) |
| Do NOT | Give neutralizing agents (acids/alkalis) - exothermic reaction worsens injury |
| Do NOT | Give activated charcoal |
| Dilution | If the patient is conscious and able to swallow: give 4-8 oz (120-240 mL) of water or milk to dilute and flush residual acid from the esophagus - only effective within the first 5 minutes of ingestion |
| Remove clothing | Prevent ongoing skin injury; use PPE (rubber gloves, apron, eye protection) |
| Call | Poison Control: 1-800-222-1222 (US) |
Emergency Department Management
Step 1 - Airway (Top Priority)
- Immediately assess for upper airway injury: hoarseness, stridor, voice changes, inspiratory dyspnea, uvular edema
- Any of these signs = emergency intubation (video laryngoscope preferred - best view with least trauma)
- Do NOT perform blind nasotracheal intubation
- If edema/necrosis makes intubation impossible → tracheotomy
- For airway edema: consider dexamethasone 10 mg IV (single dose) to reduce edema - benefit rationale similar to post-extubation laryngeal edema
- Use awake flexible endoscopy for intubation if significant symptoms anticipated (anticipated difficult airway)
Step 2 - Circulation and Resuscitation
- IV access - large bore
- Bolus isotonic crystalloid (normal saline) 20-40 mL/kg - fluid shifts from intravascular to interstitial space cause hypotension
- Monitor: HR, BP, urine output, SpO2
- Continuous cardiac monitoring + 12-lead ECG
- Capillary blood glucose check
Step 3 - Investigations
| Test | Rationale |
|---|---|
| ABG / serum pH + bicarbonate | Severity of metabolic acidosis (non-anion gap with HCl) |
| Serum electrolytes, lactate | Lactate elevation = GI necrosis indicator |
| CBC, coagulation profile | Hemorrhage, DIC assessment |
| Blood glucose | Hypoglycemia from stress |
| Chest X-ray + Abdominal X-ray | Pneumomediastinum, pneumothorax, pneumoperitoneum (perforation) |
| CT chest + abdomen | Preferred - more sensitive for perforation (mediastinal air, extraluminal air); also grades esophageal injury |
| Endoscopy (EGD) | 12-48 hours post-ingestion if no perforation suspected |
| Bronchoscopy | If persistent hypoxia or increasing A-a gradient after intubation |
| Nasopharyngoscopy | After vasoconstrictor (e.g. phenylephrine) + local anesthesia (4% lidocaine) to assess supraglottic injury |
Note: If perforation is suspected - go straight to surgery/CT, NOT endoscopy first.
Endoscopic Grading of Caustic Injury (Table 28.1, Sleisenger & Fordtran)
| Grade | Endoscopic Findings | Outcome |
|---|---|---|
| I | Edema and erythema | Heals without sequelae |
| IIA | Hemorrhage, erosions, blisters, ulcers with exudate | Heals without sequelae |
| IIB | Circumferential ulceration | Stricture in 70-100% |
| III | Deep ulcers with brown/black/gray discoloration (necrosis) | Stricture in 70-100% |
| IV | Perforation | Mortality up to 65%; urgent surgery |
EGD should be performed within 12-24 hours (no later than 48 hours). A repeat "re-look" endoscopy at 5 days better predicts esophageal/gastric complications.
Note: ~40-80% of patients with reported caustic ingestion will have no injury on endoscopy.
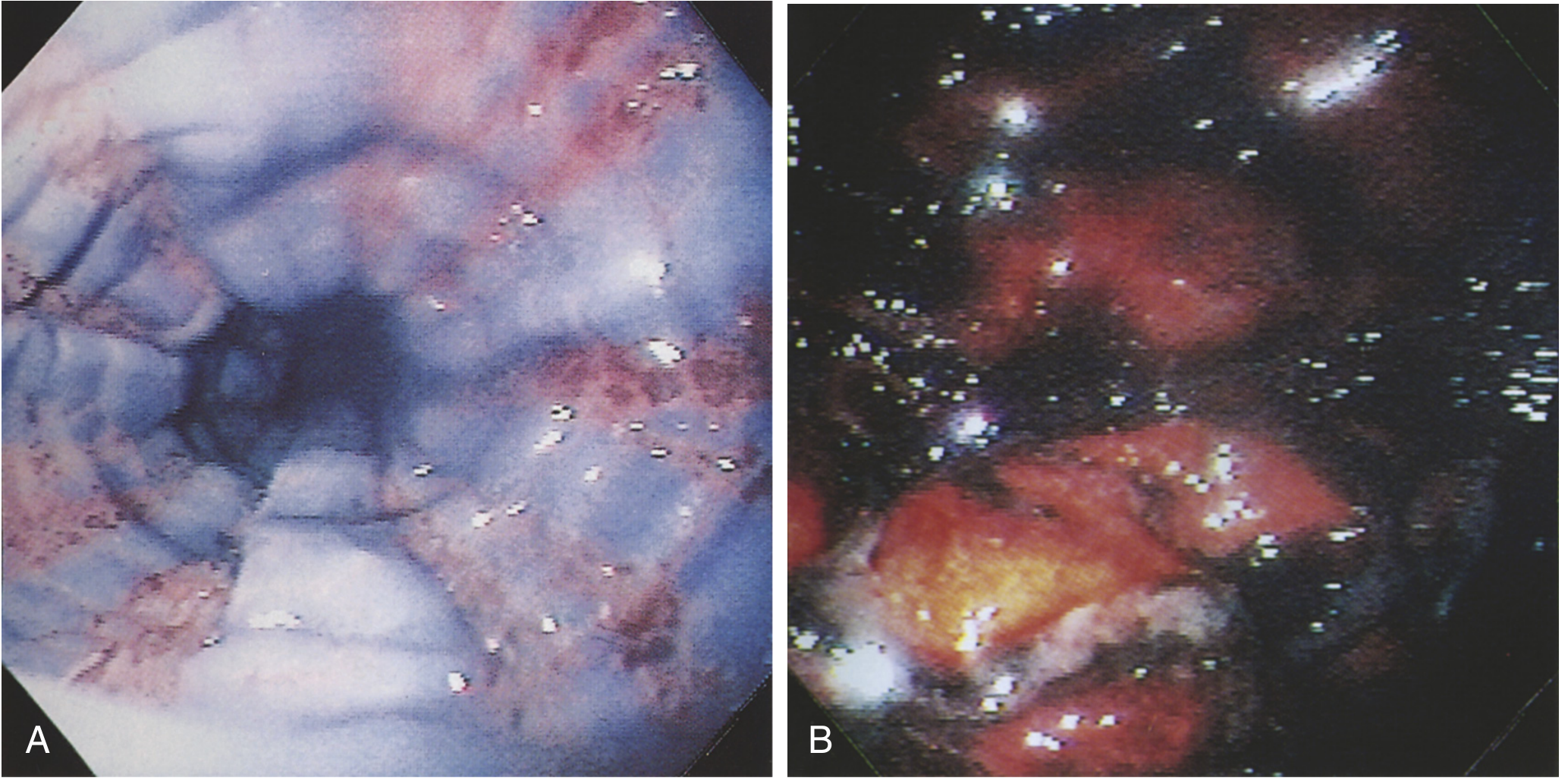
Endoscopic appearance of acid caustic injury: sloughed esophageal mucosa (left) and hemorrhagic/edematous gastric mucosa (right)
Specific Considerations for Acid (HCl) vs. Alkali
| Feature | HCl (Acid) | Alkali (NaOH, etc.) |
|---|---|---|
| Mechanism | Coagulative necrosis | Liquefactive necrosis |
| Primary target | Stomach (antrum) | Esophagus |
| Esophageal perforation risk | Lower | Higher |
| Gastric perforation risk | Higher | Lower |
| Anion gap | Non-anion gap metabolic acidosis | Lactic acidosis from necrosis |
| Nasogastric aspiration | May be considered if presenting within 30-45 min (massive ingestion) | Contraindicated |
Special note on nasogastric aspiration for acid ingestion: Careful NG aspiration may decrease acid absorption and is an exception to the usual "no NG tube" rule - only appropriate within 30-45 minutes of massive HCl ingestion because esophageal perforation risk with acid is lower than with alkali. This is a clinical judgment call. - Rosen's Emergency Medicine, p. 2951
Pharmacological Management
| Drug | Indication | Evidence |
|---|---|---|
| IV PPI (e.g. pantoprazole/omeprazole) | Reduce further acid injury, promote healing | Standard of care |
| Dexamethasone 10 mg IV | Airway edema only (single dose) | Weak - no controlled trials; benefit/risk favors use for life-threatening airway edema |
| Corticosteroids for esophageal stricture prevention | Grade IIB burns | Controversial - generally NOT recommended; one pediatric study showed benefit but overall evidence is poor with risk of hemorrhage, infection, and masking of inflammation |
| Antibiotics | Prophylactic use - NOT indicated; use only for proven perforation/infection | |
| Sucralfate / antacids | Adjunct mucosal protection - may be used | Supportive |
| Prokinetics / antiemetics | Control nausea/vomiting to reduce re-exposure | Supportive |
Decontamination Rules (Summary)
| Intervention | Status |
|---|---|
| Induced emesis | Absolutely CONTRAINDICATED |
| Activated charcoal | CONTRAINDICATED (interferes with endoscopy, no efficacy) |
| Neutralizing agents | CONTRAINDICATED (exothermic reaction) |
| Gastric lavage | CONTRAINDICATED |
| Water/milk dilution | Only if conscious + can swallow + within 5 min of ingestion |
| NG aspiration | Consider ONLY for massive acid ingestion within 30-45 min |
Surgical Indications
Urgent surgical consultation for:
- Free air (pneumoperitoneum, pneumomediastinum)
- Peritonitis / abdominal guarding
- Persistent hypotension unresponsive to fluids
- Increasing severe chest or abdominal pain
- Grade IV perforation on endoscopy/CT
- Grade III necrosis (early exploration may be warranted - controversial; individualized)
Emergency esophagectomy/gastrectomy required for perforation. Colonic interposition may be needed. Best outcomes at specialist referral centers with thoracic surgical capability.
Disposition
| Grade | Management |
|---|---|
| Grade 0 / I | Can be discharged after 4-6 hours observation; liquid diet x 24h, soft food over 3 days |
| Grade IIA | Discharge within 24-48h if asymptomatic; close GI follow-up |
| Grade IIB / III | ICU admission; IV fluids, monitoring, surgical standby |
| Any grade with hemodynamic instability or airway compromise | ICU |
| Grade IV / perforation | Emergency surgery |
| Intentional ingestion (this patient - 24M) | Mandatory psychiatric evaluation |
ICU-Level Red Flags (Transfer/Escalate Immediately)
Per 2025 Intensive Care Medicine guidelines, pure HCl ingestion in an adult regardless of volume warrants ICU transfer to a center with major abdominal and thoracic surgical capability. This patient (24M, intentional ingestion) should be managed at a tertiary center from the outset.
Long-Term Follow-Up
- Esophageal stricture develops in 70-100% of grade IIB/III injuries - may require repeated endoscopic dilation (defer dilation to >4 weeks post-ingestion to reduce perforation risk)
- Esophageal carcinoma risk is increased - long-term endoscopic surveillance required (years to decades post-injury)
- Esophagogram with water-soluble contrast at ~24 hours post-ingestion if high-grade injury to detect delayed perforation
- Psychiatric and psychological support for this young adult (intentional ingestion)
Sources:
- Rosen's Emergency Medicine, Caustic Ingestions chapter, pp. 2948-2952
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 28
- ATSDR Medical Management Guidelines - Hydrogen Chloride
- Ten tips for managing caustic ingestion in adults - Intensive Care Medicine 2025
- Sabzé A et al. (2024). Hydrochloric acid ingestion in adults: 10-year retrospective cohort. Br J Anaesth 133(6):1344-1346
This is a shared conversation. Sign in to Orris to start your own chat.