parathyroid gland and its disorders in detail trousseau sign calcium levels
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive information from authoritative textbooks. Let me compile the detailed answer.
Parathyroid Gland - Anatomy, Physiology, and Disorders
Anatomy and Embryology
Humans normally have four parathyroid glands, located in close proximity to the superior and inferior poles of the thyroid lobes.
- Superior parathyroids: derived from the endoderm of the 4th pharyngeal pouch
- Inferior parathyroids: derived from the 3rd pharyngeal pouch (along with the thymus)
- Supernumerary (extra) glands occur in 3-5% of the population and may be found ectopically along the migratory path, within the thymus, or within the thyroid
Each gland weighs approximately 35-40 mg normally. The chief cells secrete PTH; oxyphil cells appear after puberty and their function remains uncertain.
PTH: Structure and Secretion
PTH is an 84-amino acid peptide encoded by the PTH gene on chromosome 11p15. The mature peptide is secreted after cleavage of prepro-PTH → pro-PTH → PTH.
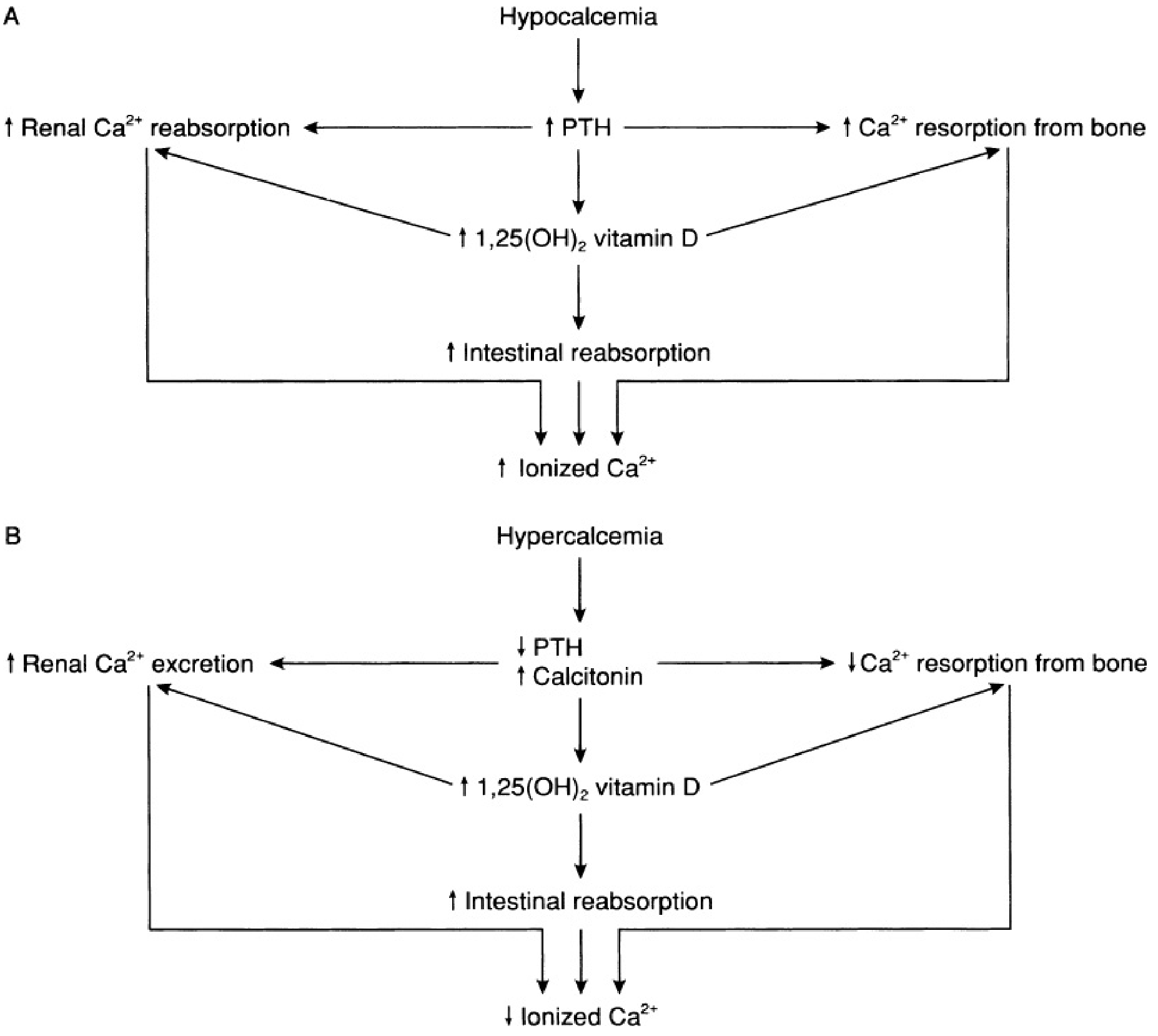
Calcium-Sensing Receptor (CaSR)
Parathyroid cells express the G protein-coupled calcium-sensing receptor (CaSR). When extracellular Ca²⁺ rises:
- CaSR activation → phospholipase C stimulation → IP₃ accumulation → ↑ intracellular Ca²⁺
- This reduces PTH secretion and increases urinary calcium excretion
Conversely, hypocalcemia releases CaSR inhibition, rapidly increasing PTH secretion.
PTH Actions (The Calcium-Phosphate Axis)
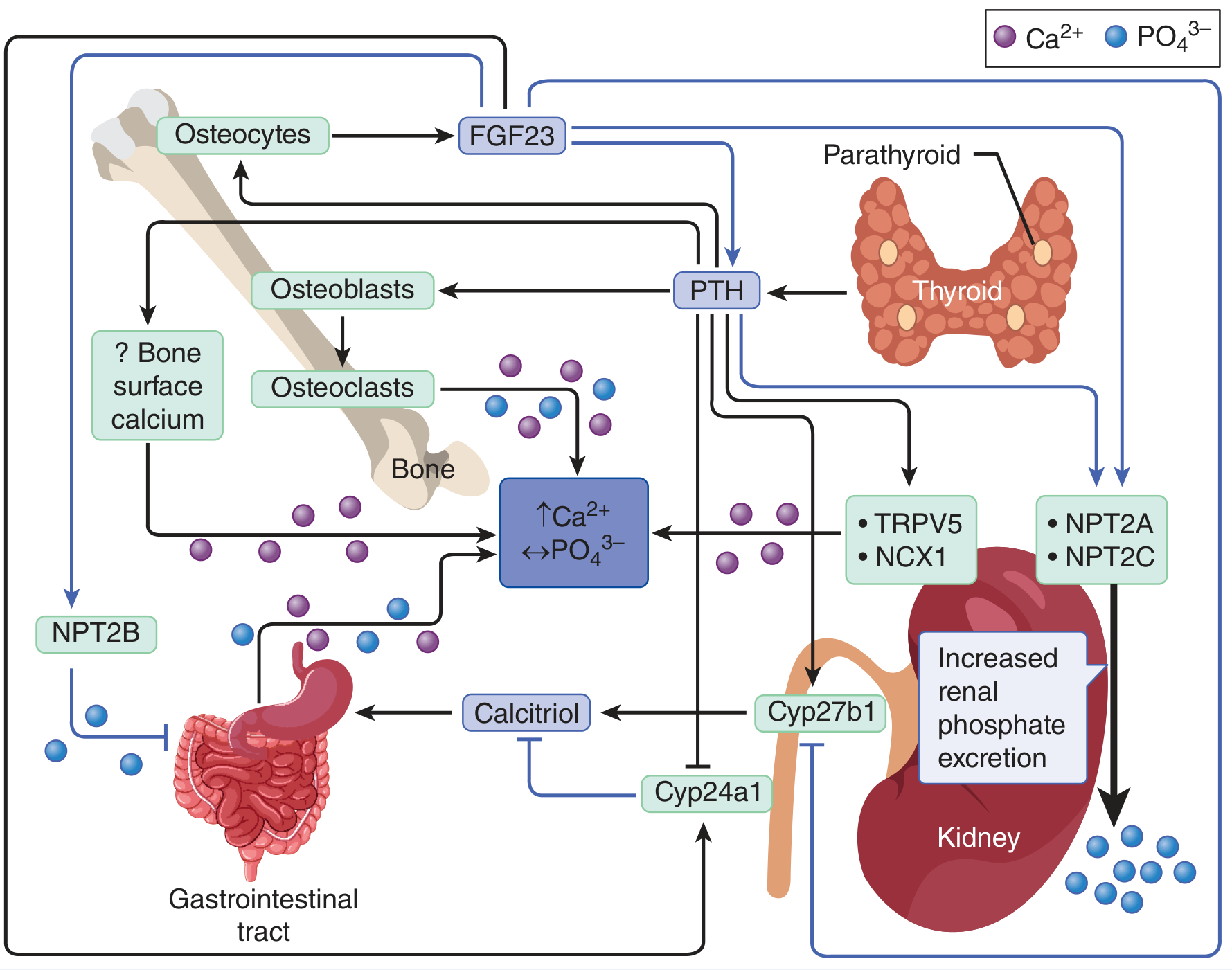
PTH-calcium-phosphate regulation - Goldman-Cecil Medicine
PTH acts on three main organs:
| Organ | Effect |
|---|---|
| Kidney | ↑ Ca²⁺ reabsorption (TRPV5, NCX1); ↑ phosphate excretion (via NPT2A, NPT2C); activates 1α-hydroxylase → ↑ 1,25(OH)₂D (calcitriol) |
| Bone | Stimulates osteoblasts → activates osteoclasts → ↑ Ca²⁺ and PO₄³⁻ release from bone |
| Gut | Indirectly (via calcitriol) → ↑ intestinal Ca²⁺ absorption (NPT2B inhibited for phosphate) |
Net result: PTH raises serum Ca²⁺ and lowers serum phosphate.
FGF23 (from osteocytes) works in opposition, promoting phosphate excretion and inhibiting calcitriol production.
Calcium Homeostasis
Normal serum calcium: 8.5-10.5 mg/dL (total); ionized Ca²⁺ 4.5-5.0 mg/dL
Forms of circulating calcium:
- ~45% bound to albumin
- ~10% bound to anions (citrate, phosphate, bicarbonate)
- ~45% free ionized (the physiologically active fraction)
Correcting for Albumin
Corrected Ca²⁺ = Measured Ca²⁺ + 0.8 × (4 - albumin g/dL)
In hypoalbuminemia: total Ca²⁺ falls but ionized Ca²⁺ may be normal ("false hypocalcemia"). In alkalosis or citrate excess, ionized Ca²⁺ falls with minimal change in total calcium.
PTH/Ca²⁺ Pattern Table (Henry's Clinical Diagnosis)
| Condition | Ionized Ca²⁺ | PTH | Cause |
|---|---|---|---|
| Normocalcemia | Normal | Normal | - |
| Hypoparathyroidism | Low | Low | Parathyroid glands |
| Vitamin D deficiency / renal failure | Low | High | Secondary HPT |
| Primary hypercalcemia (malignancy etc.) | High | Low | CHIMPS* |
| Primary hyperparathyroidism | High | High | Parathyroid adenoma/hyperplasia |
CHIMPS = Cancer, Hyperthyroidism, Iatrogenic, Multiple myeloma, hyperParathyroidism, Sarcoidosis
Parathyroid Disorders
1. Primary Hyperparathyroidism (PHPT)
Etiology
- Solitary parathyroid adenoma: ~85% of cases
- Multiglandular hyperplasia: ~15% (often familial)
- Parathyroid carcinoma: <1%
- Familial forms: MEN 1 (parathyroid + pituitary + pancreas), MEN 2A (parathyroid + medullary thyroid Ca + pheochromocytoma), HPT-JT syndrome, familial isolated hyperparathyroidism (FIHP)
Pathophysiology
Autonomous PTH secretion → hypercalcemia. The CaSR set-point is raised, so PTH secretion continues inappropriately despite elevated calcium.
Clinical Features - "Moans, Groans, Pains, and Stones"
| System | Manifestations |
|---|---|
| Renal | Nephrolithiasis (calcium oxalate/phosphate), nephrocalcinosis, polyuria, polydipsia |
| Musculoskeletal | Bone pain, osteopenia, osteoporosis, fractures, osteitis fibrosa cystica (subperiosteal resorption, "salt-and-pepper" skull, brown tumors), proximal myopathy |
| GI | Nausea, vomiting, constipation, anorexia, peptic ulcers, pancreatitis |
| Neuropsychiatric | Fatigue, lethargy, depression, confusion, coma |
| Cardiac | Shortened QT interval, bradycardia, 1st-degree AV block, arrhythmias |
- Hypercalcemia is usually modest (<11 mg/dL) in PHPT; severe symptoms more likely in malignancy
Diagnosis
- Elevated serum Ca²⁺ + elevated (or "inappropriately normal") PTH
- 24-hour urine calcium elevated (helps distinguish from FHH where urine Ca is low)
- Imaging: sestamibi scan, ultrasound, 4D CT for localization preoperatively
Indications for Surgery (Parathyroidectomy)
- Serum Ca²⁺ > 1 mg/dL above upper normal
- Creatinine clearance <60 mL/min
- 24h urine Ca >400 mg or increased nephrolithiasis risk
- T-score < -2.5 (osteoporosis) at any site
- Age <50 years
- Patient preference / unable to participate in surveillance
Medical Management
- Cinacalcet (calcimimetic): allosteric CaSR activator, 30 mg BID up to 90 mg BID - lowers PTH and serum Ca
- Bisphosphonates: for bone protection
- Hydration + loop diuretics for acute hypercalcemia
2. Secondary Hyperparathyroidism
- PTH rises in response to persistent hypocalcemia (appropriate response)
- Most common cause: chronic kidney disease (CKD) - low calcitriol + hyperphosphatemia → low Ca²⁺ → ↑PTH
- Also: vitamin D deficiency, malabsorption
- Serum Ca²⁺ is low or normal, PTH is elevated
- Treatment: Phosphate binders, vitamin D supplementation (calcitriol), cinacalcet
3. Tertiary Hyperparathyroidism
- Develops in longstanding secondary hyperparathyroidism (typically CKD)
- Parathyroid glands become autonomous - PTH secretion persists despite normocalcemia or even hypercalcemia
- Presumed progression: polyclonal hyperplasia → monoclonal autonomous adenoma
- Serum Ca²⁺ is elevated, PTH is markedly elevated
- Definitive treatment: subtotal or total parathyroidectomy
4. Hypoparathyroidism
Causes
| Category | Examples |
|---|---|
| Surgical (most common) | Post-thyroidectomy, post-parathyroidectomy |
| Parathyroid agenesis | DiGeorge syndrome (22q11.2 deletion - no parathyroids + thymus) |
| Autoimmune | Isolated or polyglandular autoimmune syndrome type 1 (APS-1 / APECED) |
| Infiltration | Hemochromatosis, amyloidosis, sarcoidosis, Wilson's disease, thalassemia |
| Radiation | External beam or ¹³¹I therapy |
| Functional | Hypomagnesemia (blocks PTH secretion AND causes PTH resistance) |
| Genetic | PTH gene mutations, activating CaSR mutations (autosomal dominant hypocalcemia) |
| Hungry bone disease | Post-parathyroidectomy rapid calcium uptake by bones |
Clinical Features of Hypocalcemia
Neuromuscular (most prominent):
- Circumoral and peripheral paresthesia (tingling)
- Muscle cramps and tetany
- Carpopedal spasm
- Chvostek sign and Trousseau sign (see below)
- Laryngospasm / bronchospasm
- Seizures (focal, petit mal, grand mal)
Cardiac:
- QT prolongation
- Impaired cardiac inotropy, dysrhythmias
Other:
- Depression, anxiety, irritability, confusion
- Cataracts (chronic hypocalcemia)
- Abnormal dentition and skeletal malformations (congenital)
- Papilledema (intracranial hypertension)
Treatment
- Acute/symptomatic: IV calcium gluconate (10 mL of 10% solution) slowly
- Chronic: Oral calcium carbonate + active vitamin D (calcitriol 0.25-1 mcg/day)
- Correct concurrent hypomagnesemia
- "Hungry bone" post-parathyroidectomy: may require IV calcium for weeks
5. Pseudohypoparathyroidism (PHP)
- Hypocalcemia + hyperphosphatemia + elevated PTH + tissue resistance to PTH
- Magnesium and calcidiol levels are normal
- Confirmed by PTH infusion test: normal PTH → ↑ urinary cAMP and phosphate; in PHP, this response is absent
- Associated with Albright's hereditary osteodystrophy (PHP type 1a): short stature, round face, brachydactyly, obesity, subcutaneous ossifications
Trousseau Sign
Definition: The development of carpal spasm (carpopedal spasm) when a sphygmomanometer cuff is inflated over the brachial artery to a pressure above systolic blood pressure and maintained for 3 minutes.
What is seen: The hand adopts a characteristic posture with:
- Wrist flexion
- MCP flexion
- IP extension
- Thumb adduction (the "obstetric hand" or "main d'accoucheur")
Mechanism: Occluding circulation renders the peripheral nerve ischemic. Ischemia lowers the threshold for spontaneous depolarization in the setting of low ionized calcium, producing involuntary muscle contraction.
Specificity vs. Chvostek: Trousseau sign is more specific for hypocalcemia than Chvostek sign. Chvostek (tapping the facial nerve anterior to the ear causing facial muscle contraction) can be positive in ~10-25% of normal individuals.
Clinical use: If positive, hypocalcemia should be confirmed by direct measurement of ionized calcium. In mild tetany where spontaneous spasm is not yet evident, Trousseau sign can unmask latent tetany.
Summary: Calcium Levels and Key Disorders
| Condition | Serum Ca²⁺ | PTH | Phosphate | Key feature |
|---|---|---|---|---|
| Primary hyperparathyroidism | ↑ | ↑ | ↓ | Adenoma; "stones, moans, groans" |
| Secondary hyperparathyroidism | ↓ or N | ↑↑ | ↑ (in CKD) | Appropriate response to CKD/Vit D deficiency |
| Tertiary hyperparathyroidism | ↑ | ↑↑↑ | Variable | Autonomous glands in CKD |
| Hypoparathyroidism | ↓ | ↓ or absent | ↑ | Post-surgical most common |
| Pseudohypoparathyroidism | ↓ | ↑↑ | ↑ | PTH resistance; Albright's phenotype |
| Malignancy (PTHrP) | ↑ | ↓ | ↓ | Lung/renal/breast Ca; PTHrP not detected by PTH assay |
| FHH (familial hypocalciuric hypercalcemia) | ↑ | N or ↑ | N | Low urine Ca/Cr ratio; CaSR mutation |
| Vitamin D deficiency | ↓ or N | ↑ | ↓ | Secondary HPT; rickets/osteomalacia |
Sources: Goldman-Cecil Medicine, 2 Vol. Set, Ch. 227 | Mulholland & Greenfield's Surgery, 7e, Ch. 76 | Frameworks for Internal Medicine, Ch. 5 | National Kidney Foundation Primer on Kidney Diseases, 8e | Henry's Clinical Diagnosis and Management by Laboratory Methods, Table 9.8 | Brenner and Rector's The Kidney, 2-Vol. Set
This is a shared conversation. Sign in to Orris to start your own chat.