Principles and Application of MRI in ent according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive content from multiple ENT textbooks. Let me compose the complete, detailed answer.
Principles and Application of MRI in ENT
Based on: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vols 1 & 2); K.J. Lee's Essential Otolaryngology; Shambaugh Surgery of the Ear
1. PHYSICAL PRINCIPLES OF MRI
Basic Mechanism
MRI generates images by exploiting the response of biological tissues to an applied and changing magnetic field, without the use of ionizing radiation. The signal is derived from hydrogen protons, which are most abundant in tissue fat and water.
When placed in a high magnetic field, spinning protons align in the direction of the field. Radiofrequency (RF) pulses are then transmitted into the patient, exciting the protons and changing their orientation relative to the magnetic field. As protons realign (relax), they release energy as an RF signal detected by receiver coils, which is then reconstructed into an image.
- Cummings Otolaryngology, Ch. 8
Magnets Used in Clinical MRI
| Type | Description |
|---|---|
| Permanent magnets | Composed of large magnetic metallic elements; no continual energy input needed; generate a uniform field between components |
| Superconducting magnets | Electromagnets of niobium-titanium wire; require energy to start; maintained in superconducting state by liquid nitrogen and liquid helium shells |
Field Strength: The tesla (T) is the unit of magnetic strength (1 T = 10,000 gauss). The Earth's field is 0.5 gauss. Clinical MRI units operate at 0.3 to 3.0 T, with research scanners up to 9.0 T. Higher field strength yields a higher signal/noise ratio and better image quality.
- Cummings Otolaryngology, Ch. 8
2. COILS AND TECHNICAL CONSIDERATIONS
Receiver Coils
A surface coil acts as a receiving antenna for the RF signal emitted after initial RF stimulation. For head and neck work:
- Standard head coil: Adequate for disease above the angle of the mandible; allows imaging of adjacent brain and orbits - useful when lesions extend intracranially
- Neck coil: Volume neck coil or anterior neck coil; covers skull base to clavicles; significantly improves signal/noise ratio
- Surface coils collect signal from a smaller body part, which improves resolution
Surface coils are mandatory for head and neck imaging. Low-field "open" MRI units do not provide the spatial resolution or signal/noise characteristics required for evaluating skull base or laryngeal anatomy.
- Cummings Otolaryngology, Ch. 8 & Ch. 107
Slice Thickness
Slice thickness is most commonly 3 to 5 mm, with thinner sections for smaller regions of interest (e.g., facial nerve). A thinner slice has a smaller signal/noise ratio. Volume acquisition techniques may be needed for small structures. Covering the neck from skull base to superior mediastinum often requires two separate acquisitions.
3. PULSE SEQUENCES AND SIGNAL CHARACTERISTICS
The following is an overview of the main pulse sequences used in ENT/head and neck MRI:
T1-Weighted Images (T1WI)
- Short TR (500-700 ms) and short TE (15-40 ms)
- Fat = high signal (bright/white) - provides natural contrast in head and neck
- Air, rapid blood flow, cortical bone, CSF, vitreous = low signal (dark/black)
- Muscle = low to intermediate signal
- Bone marrow = bright (fat within marrow)
- The fundamental head and neck sequence: provides excellent soft tissue anatomy, high signal/noise ratio, minimal motion artifact (4-5 min acquisition)
T2-Weighted Images (T2WI)
- Long TR and long TE
- Fluid = high signal (bright)
- Fat = high signal
- T2WI is sensitive for pathology; postobstructive change with high fluid content is typically bright on T2, while tumors usually show intermediate brightness
- Particularly useful for differentiating tumor from retained secretions
Gadolinium-Enhanced T1WI
- IV gadolinium (a paramagnetic contrast agent) shortens T1 relaxation times and increases signal intensity in vascularized/inflamed tissues
- Enhances solid tumors, perineural spread, meningeal disease, infected mucosa
- Gadolinium substantially lower allergic reaction risk than iodinated CT contrast
- Contraindicated/used conservatively in renal dysfunction (risk of nephrogenic systemic fibrosis)
Fat-Suppressed Sequences (Fat-Sat)
- Selectively darken lipid-rich areas, allowing enhancing lesions to stand out
- Critical for distinguishing gadolinium enhancement from adjacent fat
- Applied to both T1WI (post-contrast) and T2WI
- Particularly important at the skull base and pterygopalatine fossa
Short T1 Inversion Recovery (STIR)
- Suppresses fat signal; highlights edema and fluid
- Useful for detecting marrow infiltration, lymph node disease, and inflammatory change
Diffusion-Weighted Imaging (DWI)
-
Measures tissue cellularity and water diffusivity
-
Restricted diffusion (bright DWI, low apparent diffusion coefficient [ADC]) indicates hypercellular or dense tissue (malignant tumors, cholesteatoma, epidermoid cysts)
-
ADC values (sinonasal):
- Benign lesions: ADC ≥ 1.5 (±0.5) × 10⁻³ mm²/s
- Malignant lesions: ADC ≤ 0.98 (±0.5) × 10⁻³ mm²/s
-
DWI is particularly useful in distinguishing epidermoid cysts (restricted diffusion) from arachnoid cysts (no restriction)
-
Increasingly used for detecting residual and recurrent nasopharyngeal carcinoma (NPC) after treatment
-
Cummings Otolaryngology, Ch. 8 & Ch. 47
Gradient-Echo Sequences
- Faster acquisition; useful for vascular imaging (MR angiography)
- More susceptible to metallic artifacts than spin-echo
4. MRI ARTIFACTS IN ENT
| Artifact | Cause | Effect |
|---|---|---|
| Motion artifact | Patient movement, swallowing, breathing | Anatomic distortion, signal mismapping; worse at high field strength |
| Chemical shift artifact | Difference in resonance frequencies of fat and water protons | Bright band on one side and dark band opposite; pseudocapsule around a lesion; most noticeable on T1WI |
| Metallic/susceptibility artifact | Dental amalgam, orthodontic braces, metallic implants | Signal dropout; may obscure mandible, maxilla, floor of mouth |
| Mascara artifact | Metallic compounds in eye makeup | Localized signal loss in anterior orbit/globe |
To limit motion artifact: sequences under 4 minutes are preferred; patients instructed not to swallow and breathe shallowly.
Fig. 8.5 from Cummings illustrates metallic artifact from orthodontia distorting anterior facial structures:
5. ADVANTAGES AND DISADVANTAGES OF MRI IN ENT
Advantages
- No ionizing radiation
- Superior soft tissue contrast and differentiation
- Direct imaging in any plane (axial, coronal, sagittal, oblique)
- Multiple sequences allow precise tissue characterization
- Better delineates perineural spread, intracranial extension, marrow invasion
- Distinguishes tumor from retained secretions (key in sinuses)
- Reduced artifacts from dental amalgam compared to CT
- Can fuse with CT/PET for radiotherapy planning
- Better detection of ectopic mediastinal parathyroid glands (sensitivity >80%)
Disadvantages
-
Long scan duration (susceptibility to motion artifact)
-
Small bore induces claustrophobia
-
Contraindications: ferromagnetic implants, older cardiac pacemakers/defibrillators, ferromagnetic aneurysm clips
-
Cochlear implants require special precautions (see below)
-
No visualization of fine bony detail (CT is superior for this)
-
Less useful in the thorax (motion, field distortions)
-
Gadolinium contraindicated in renal impairment
-
Cummings Otolaryngology, Ch. 107
6. ENT-SPECIFIC APPLICATIONS
6a. Paranasal Sinuses and Nasal Cavity
MRI at 1.5 T or greater is the preferred modality for evaluating neoplastic sinus disease. CT and MRI are complementary - CT for bony anatomy and surgical planning, MRI for soft tissue characterization.
MRI roles in sinus disease:
- Distinguishes tumor from postobstructive secretions (tumors: intermediate T2; secretions: bright T2)
- Detects perineural spread: nerve enhancement and enlargement on gadolinium T1 predict spread; retrograde involvement of Meckel's cave/cavernous sinus carries poor prognosis
- Assesses skull base invasion: dural thickening >2 mm, loss of hypointense zone, nodular enhancement are highly predictive of dural invasion
- Differentiates orbital periosteum from tumor: lamina papyracea enhancement indicates orbital involvement
- Detects encroachment into fat-rich spaces (periorbita, pterygopalatine fossa, parapharyngeal space) on precontrast T1WI - tumor appears darker against bright fat
- Fungal disease appears iso- or hypo-intense on T1, with signal void on T2 (characteristic finding)
- Post-obliterative frontal sinus: MRI can distinguish mucocele from fat necrosis and infection
Multi-sequence example (ethmoid SCC) showing complementary sequences:
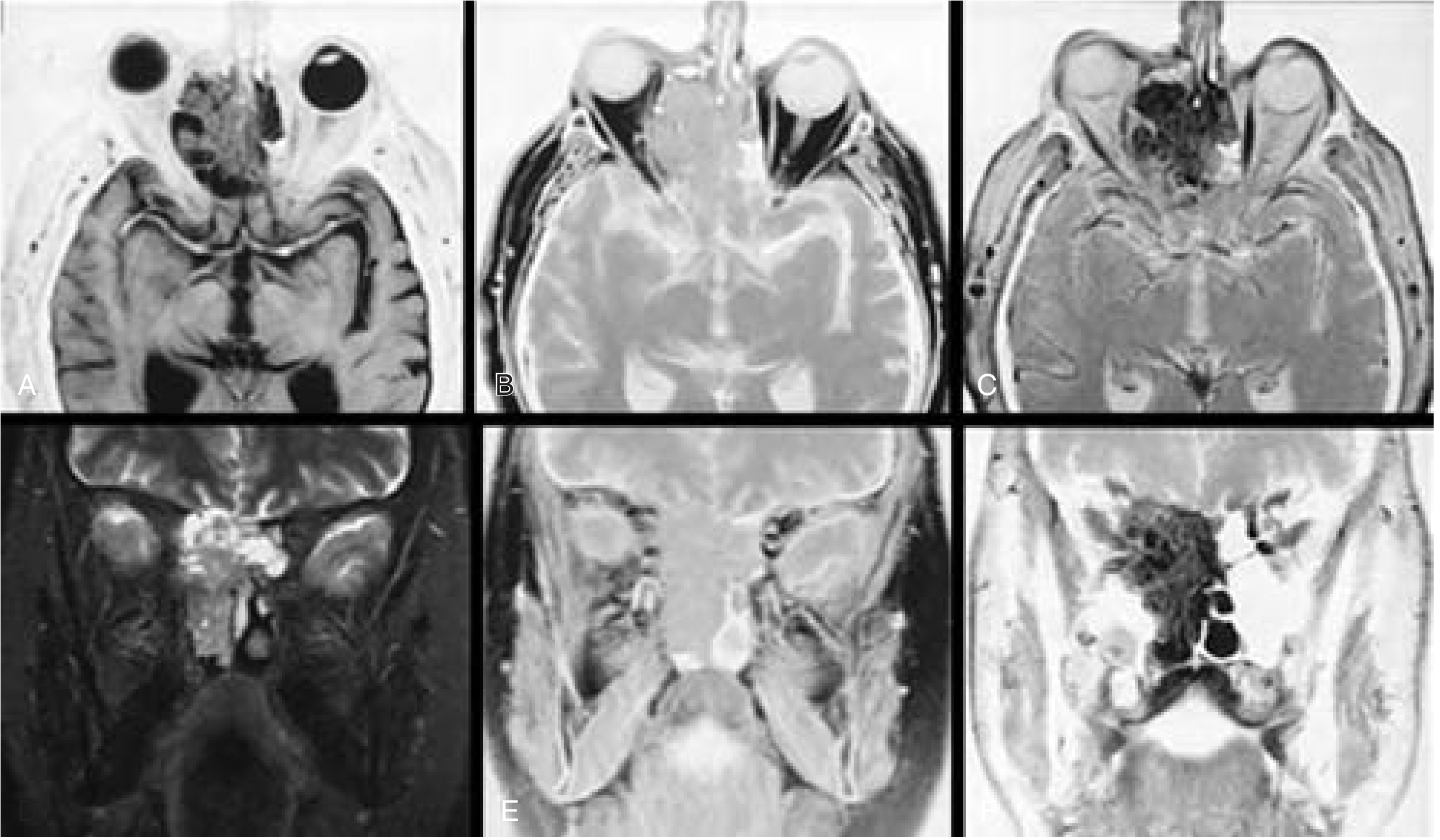
Fig. 94.1 from Cummings: Ethmoid SCC - (A) FS T2 TSE axial: high signal tumor with orbital infiltration; (B) T1-SE axial: low signal tumor; (C) FS T1 gadolinium-DTPA: tumor enhancement; (D) STIR coronal: skull base destruction clearly demonstrated.
- Cummings Otolaryngology, Ch. 94; Scott-Brown's Vol 1, Ch. 99
6b. Salivary Gland Tumors
MRI is the modality of choice for evaluating salivary neoplasms, due to the excellent soft tissue differentiation and the fatty background of the parotid gland.
Key principles:
- Parotid lesions are easily identified against the hyperintense fat on T1WI
- Post-contrast fat-saturated T1WI: fat becomes dark, mass stands out clearly
- Gadolinium helps assess perineural spread (enhancement along cranial nerves), intracranial extension, and bone marrow invasion
- Any irregular/ill-defined mass on US or suspicious cytology on FNA should be further evaluated with MRI
Tissue characterization:
| Feature | Benign | Malignant |
|---|---|---|
| Margins | Smooth, well-defined | Ill-defined |
| T2 signal | High | Low |
| Enhancement | Moderate, with capsule | Irregular, infiltrative |
| Perineural spread | Absent | Cranial nerve enhancement/enlargement |
Specific tumors:
- Pleomorphic adenoma: Low T1, high T2 (similar to water); solid enhancement on fat-suppressed post-gadolinium T1WI; recurrent disease appears as single or multiple T2 hyperintense masses in parotidectomy bed
- Warthin tumor: Partially cystic lesion; common in smokers >40 years
- Adenoid cystic carcinoma: Infiltrative; classic perineural spread along V3 through foramen ovale (coronal gadolinium views)
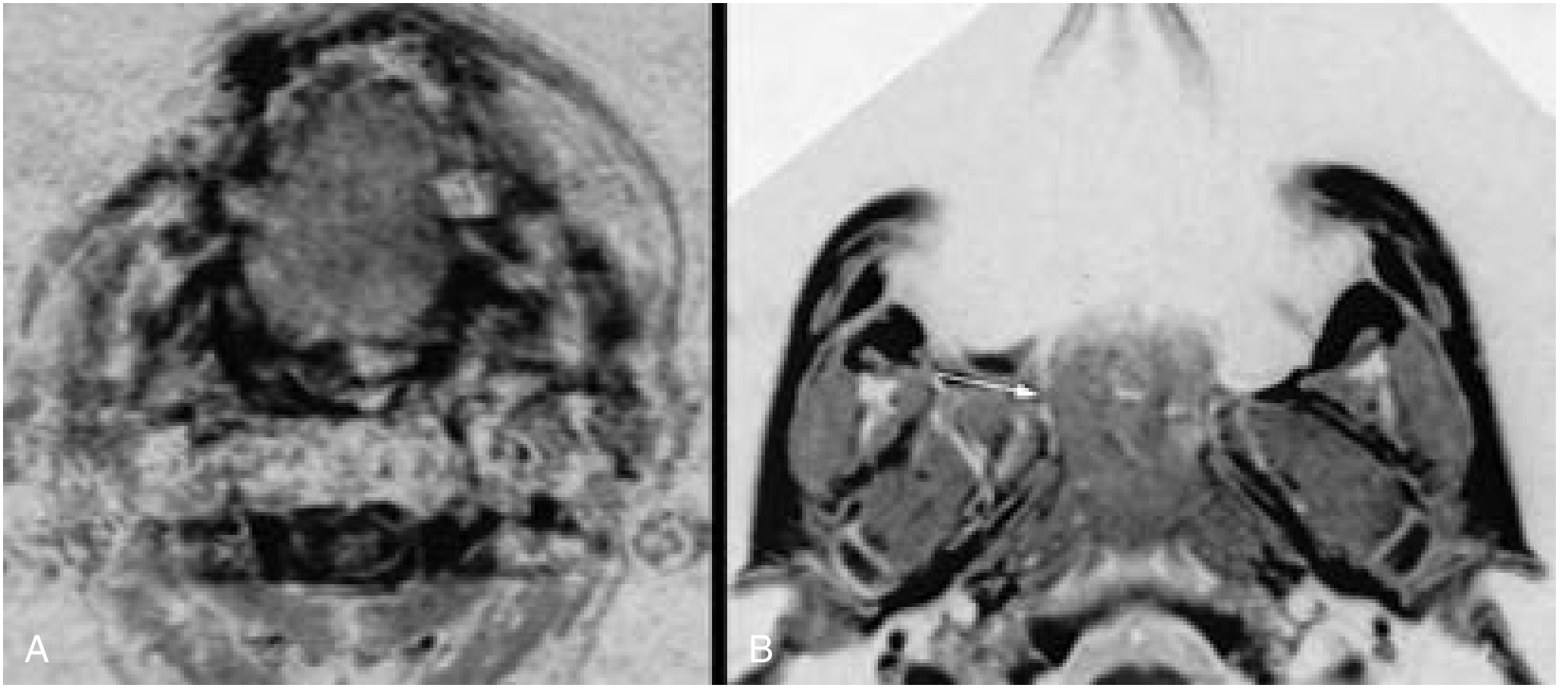
MRI showing adenoid cystic carcinoma with perineural spread:
Fig. 82.5 from Cummings: (A) Axial gadolinium MRI - enhancing infiltrative adenoid cystic carcinoma in deep lobe of left parotid; (B) Coronal gadolinium MRI - extension of tumor along V3 through foramen ovale indicating perineural spread.
- Cummings Otolaryngology, Ch. 82
6c. Nasopharyngeal Carcinoma (NPC)
MRI is the preferred modality for NPC staging and treatment planning because of its superior soft tissue resolution.
-
Delineates parapharyngeal extension, perineural spread, and marrow infiltration
-
Differentiates tumor infiltration from retained secretions in paranasal sinuses
-
Better defines optic chiasma, optic nerves, and brainstem - preserving organs-at-risk in radiotherapy planning
-
MRI/CT image fusion enables precise radiotherapy targeting
-
More useful than CT for monitoring disease and detecting recurrence after treatment
-
DWI has increased diagnostic accuracy for residual/recurrent NPC; modern MRI with DWI is on par with PET-CT for detecting residual and recurrent disease
-
Scott-Brown's Otorhinolaryngology (combined vol), Ch. on NPC
6d. Skull Base
MRI provides three-layer visualization at the skull base:
- Cribriform plate with periosteal covering
- Dura mater
- Subarachnoid space
A thickened, enhancing dura suggests periosteum penetration and intracranial-extradural invasion. Brain edema on MRI is more suggestive of intracranial-intradural brain invasion. Retrograde perineural spread to Meckel's cave or cavernous sinus is a poor prognostic indicator.
DWI at skull base:
- Epidermoid cysts: restricted diffusion (bright on DWI), distinguishable from arachnoid cysts (no restriction)
- Cholesteatoma: also shows restricted diffusion on non-EPI DWI sequences
6e. Temporal Bone and Ear
MRI plays specific roles in ear disease:
- Inner ear malformations: T2 FIESTA or constructive interference in steady state (CISS) sequences beautifully delineate the membranous labyrinth, endolymph, and perilymph
- Acoustic neuroma / Vestibular schwannoma: High T2 signal; gadolinium-enhancing lesion in internal auditory canal (IAC) and CPA angle
- Endolymphatic hydrops (Meniere's disease): Gadolinium-enhanced MRI (delayed, 4 hours post-IV) shows reduced endolymphatic signal in 3T MRI
- Cholesteatoma: DWI (non-EPI) shows restricted diffusion; used to detect residual/recurrent cholesteatoma without revision surgery
6f. Thyroid and Parathyroid
MRI in parathyroid disease:
-
Less common than ultrasound/sestamibi as a first-line localizing tool
-
Sensitivity for abnormal parathyroid: 74-88%
-
Useful for revision surgery (not degraded by surgical clips)
-
Excellent for detecting ectopic mediastinal glands (sensitivity >80%)
-
Parathyroid adenomas: intermediate to low T1 signal; high T2 signal
-
Accuracy is reduced in concomitant thyroid disease (present in up to 40% of hyperparathyroid patients)
-
Scott-Brown's Vol 1, Ch. 72
6g. Larynx and Hypopharynx
- Useful for staging laryngeal cancers and evaluating cartilage invasion (T4 disease)
- MRI slightly superior to CT for cartilage invasion but longer acquisition is a limitation
- Surface coil required; patients should refrain from swallowing during sequences
- Less useful in the thorax (respiratory motion artifact)
6h. Neck Spaces and Lymph Nodes
- MRI delineates fascial planes and neck space anatomy with high accuracy
- Useful for parapharyngeal space, retropharyngeal, and carotid space lesions
- DWI helps differentiate benign from malignant lymph nodes
- Preferred over CT for pediatric neck masses (no radiation)
6i. Fetal Neck Masses (Prenatal MRI)
MRI is an adjunct to prenatal ultrasound for evaluating fetal neck masses:
-
Superior soft tissue delineation for tracheal distortion and airway assessment
-
Better differentiation between solid and cystic structures
-
Less affected by raised BMI, poor fetal position, oligohydramnios
-
Useful for identifying syndromes, craniofacial anomalies, and intracranial pathology
-
In 50% of cases, MRI findings differ from ultrasound; MRI agreed with final histology in 73% of cases
-
Relevant for planning EXIT procedure (ex utero intrapartum treatment) for airway management
-
Scott-Brown's Vol 2, Ch. 36
7. MRI AND COCHLEAR IMPLANTS
A dedicated concern in ENT is the interaction between cochlear implants and MRI:
Four potential interactions:
- Movement of stimulator/receiver or electrode array
- Generation of noxious/injurious auditory stimuli
- Generation of heat
- Demagnetization
Key findings:
- Energies from ≤1.5 T fields do not produce sufficient heat to be troublesome
- Patients have not reported injurious auditory sensations at standard field strengths
- Movement is not problematic at field strengths <1.5 T; external stabilization can further limit risk
- Demagnetization does occur - up to 10% of magnetic strength lost per scan; degree depends on scan duration and field strength
Manufacturer solutions:
- Advanced Bionics: Special magnetless implant (headpiece stabilized by special earpiece)
- Cochlear Corporation (Nucleus): Removable magnet - can be extracted under local anesthesia as outpatient, replaced later
- MED-EL Pulsar: Titanium silastic housing permitting magnet removal if MRI is necessary
MRI at 1.5 T with an implant in place is not a firm contraindication in modern devices, but institutional protocols for screening must be followed.
- Shambaugh Surgery of the Ear, Ch. 6
8. CONTRAINDICATIONS TO MRI IN ENT
| Absolute/Relative Contraindication | Notes |
|---|---|
| Ferromagnetic aneurysm clips | Risk of displacement |
| Cardiac pacemakers/defibrillators (older) | Newer devices often MR-compatible |
| Cochlear implants | See above; manufacturer protocols apply |
| Ferromagnetic foreign bodies (orbital) | Pre-screening mandatory |
| Intraocular metallic foreign bodies | Risk of movement/injury |
| Renal dysfunction (gadolinium) | Risk of nephrogenic systemic fibrosis |
Each institution must have metal-screening protocols in place before MRI.
Summary Table: MRI vs CT in ENT
| Feature | MRI | CT |
|---|---|---|
| Soft tissue differentiation | Superior | Moderate |
| Bone detail | Poor | Superior |
| Radiation | None | Yes |
| Perineural spread | Best modality | Less sensitive |
| Sinus inflammation | Complementary | Primary modality |
| Cholesteatoma | DWI excellent | Basic anatomy only |
| Cochlear implant | Special precautions | Generally safe |
| Tumor vs secretion | Superior (T2) | Cannot reliably distinguish |
| Scan time | Longer | Faster |
| Claustrophobia | Relevant | Less relevant |
| Cost | Higher | Lower |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapters 8, 47, 82, 94, 107
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vols 1 & 2, Chapters on sinuses, NPC, parathyroid, fetal neck masses
- Shambaugh Surgery of the Ear, Chapter on cochlear implants and MRI
This is a shared conversation. Sign in to Orris to start your own chat.