Teach me thyroid surgery at the level of NEET PG exam.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Now I have all the material needed. Here is the complete NEET PG-level teaching on thyroid surgery:
Thyroid Surgery - NEET PG Complete Guide
1. HISTORICAL HIGH-YIELD POINTS
| Milestone | Person/Detail |
|---|---|
| First thyroidectomy | Abu al-Qasim (952 AD) - patient barely survived from blood loss |
| Term "thyroid" coined | Thomas Wharton, 1646 (from Greek thyreos = shield) |
| Anatomy first described | Leonardo da Vinci, early 16th century |
| "Father of modern thyroid surgery" | Theodor Kocher - performed >5000 thyroidectomies, mortality 0.5%, Nobel Prize 1909 (first Nobel to a surgeon) |
| Dunhill operation | Bilateral operation: complete unilateral lobectomy + contralateral subtotal resection, for thyrotoxicosis |
2. INDICATIONS FOR THYROIDECTOMY
Three broad categories (remember HGC):
- Hyperthyroidism - when nonsurgical management has failed or is not preferred
- Goiter - with or without compressive symptoms (dysphagia, dyspnea, stridor)
- Cancer / nodules - thyroid malignancy or suspicious nodules
3. TYPES OF THYROID SURGERY (VERY HIGH-YIELD)
| Procedure | What is removed | Remnant left |
|---|---|---|
| Total thyroidectomy | All visible thyroid tissue | None |
| Near-total thyroidectomy | Nearly all; < 1 g remnant at ligament of Berry | < 1 g |
| Subtotal thyroidectomy | Most; bilateral remnants | 3-5 g |
| Hemithyroidectomy / Lobectomy | One lobe + isthmus + pyramidal lobe | Contralateral lobe |
| Isthmusectomy | Isthmus + pyramidal lobe only | Both lobes intact |
When to use which operation:
- Thyroid cancer - total thyroidectomy (facilitates radioiodine ablation and surveillance)
- Graves' disease - total or near-total thyroidectomy (ATA guideline); Dunhill operation was classic
- Toxic nodule / MNG - lobectomy or total thyroidectomy depending on extent
- Low-risk DTC (< 4 cm, no extrathyroidal extension, no nodes) - lobectomy acceptable per ATA 2015 guidelines
- Isthmus papillary cancer - isthmusectomy (selected cases)
4. PREOPERATIVE PREPARATION
- Biochemical - TFTs, serum calcium, vitamin D
- Imaging - neck ultrasound (mandatory); CT neck/chest if substernal extension suspected
- FNA - for all suspicious nodules as indicated
- Laryngoscopy - check vocal cord function preoperatively if: prior neck/upper chest surgery, voice changes, known posterior extrathyroidal extension, extensive central nodal disease
- Render euthyroid before surgery:
- Antithyroid drugs (carbimazole/PTU) + beta-blockers
- Lugol's iodine / SSKI given 10 days pre-op for Graves' disease - reduces thyroid vascularity and bleeding
5. SURGICAL TECHNIQUE - STEP BY STEP
Patient Positioning
- Supine, arms tucked
- Sandbag/roll between scapulae to extend the neck - brings thyroid anteriorly (especially helpful for substernal goiters)
- Head on foam/gel ring; back raised ~20 degrees
- Neck extended but not hyperextended (prevents postoperative posterior neck pain)
Incision
- Kocher collar incision - transverse, 3-5 cm (up to longer if needed), placed 1 cm below the cricoid cartilage in or parallel to a natural skin crease
- Extended through platysma
- Subplatysmal flaps raised:
- Superiorly to thyroid cartilage
- Inferiorly to suprasternal notch
Exposure
- Strap muscles divided in midline (linea alba of neck)
- Sternohyoid separated from sternothyroid by blunt dissection
- Strap muscles rarely need to be divided transversely - if needed, cut high to preserve ansa cervicalis innervation
- If tumor invades strap muscles - resect en bloc
- Middle thyroid veins ligated and divided first (allows medial retraction of lobe)
Superior Pole Dissection
- Thyroid retracted inferiorly and medially first
- Superior pole vessels individually ligated close to the thyroid (skeletonize them on the gland)
- Critical point: avoid the External Branch of Superior Laryngeal Nerve (EBSLN) - it runs along the cricothyroid muscle just medial to the superior pole and can be injured if ligation is done far from thyroid
- EBSLN injury: loss of high-pitched phonation (singer's nerve) - Cernea classification
Identification of RLN and Parathyroids
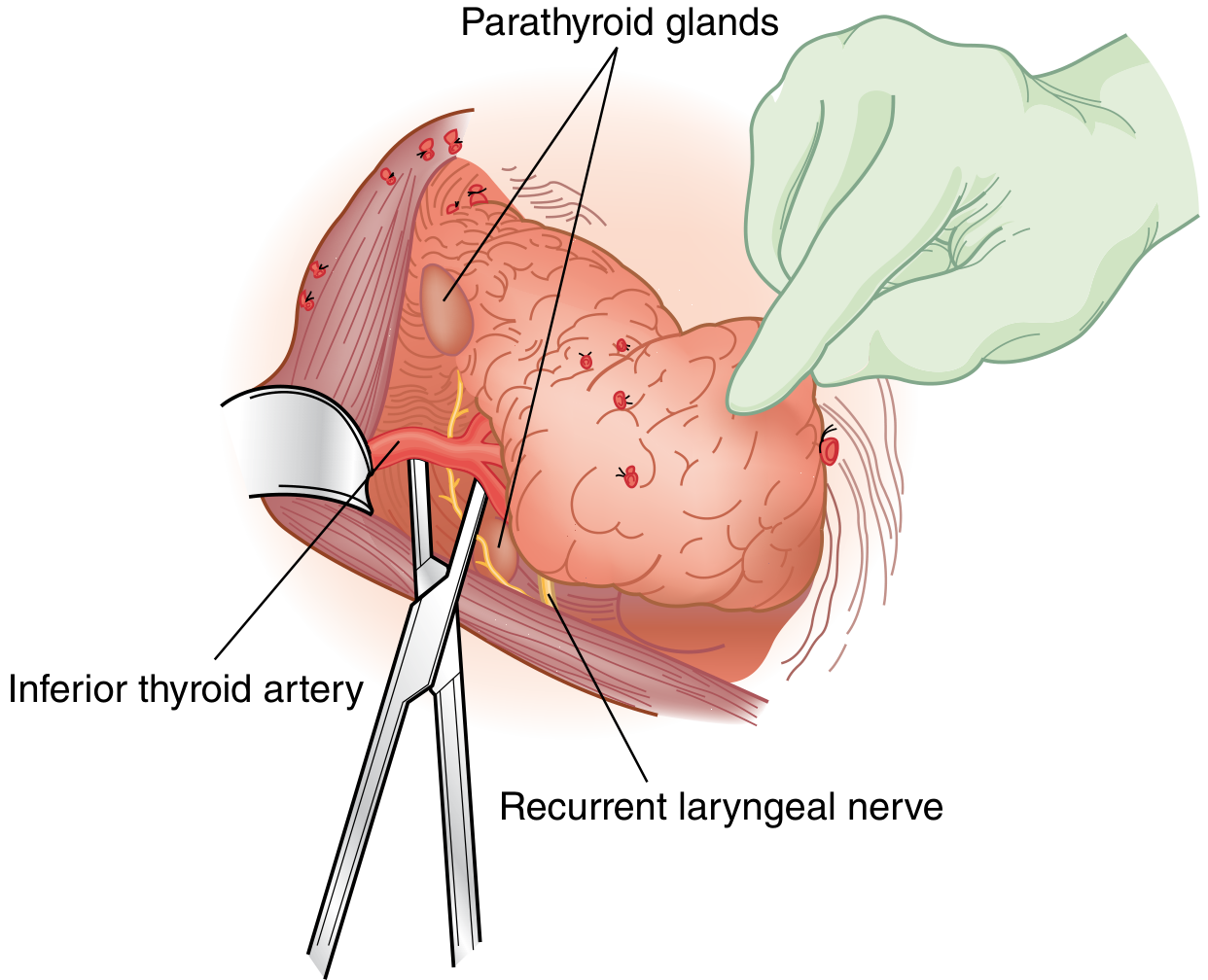
- Thyroid retracted anteromedially
- RLN found in tracheoesophageal groove
- Parathyroids usually within 1 cm of the crossing of the inferior thyroid artery and RLN
- Inferior thyroid artery ligated at branches close to thyroid surface (extracapsular dissection) - to preserve parathyroid blood supply
Ligament of Berry
- Most dangerous zone for RLN - the nerve is closest to the thyroid here and often passes through this ligament
- Do not use electrocautery near the RLN in this area
- Control bleeding with gentle pressure, then carefully ligate
Division
- If lobectomy: divide isthmus lateral to midline to minimize future hypertrophy of remnant
- Pyramidal lobe present in up to 80% of patients; must be dissected cephalad (can reach hyoid bone) until tissue tapers into fibrous band
Closure
- Strap muscles reapproximated with small gap at lower midline (allows blood to exit deeper space)
- Platysma closed with absorbable sutures
- Skin - fine subcuticular suture (cosmetic)
- No drain needed in majority of cases
- Valsalva maneuver by anesthesia to confirm hemostasis before closing
6. KEY SURGICAL ANATOMY (EXAM FAVORITE)
Recurrent Laryngeal Nerve (RLN)
| Feature | Left RLN | Right RLN |
|---|---|---|
| Origin | Loops around aortic arch | Loops around subclavian artery |
| Course | More vertical | More oblique (greater surgical risk) |
| Groove | Tracheoesophageal groove (both sides) | - |
| Most dangerous zone | Ligament of Berry | Ligament of Berry |
- RLN runs deep to inferior thyroid artery in most cases (may be anterior to it - variable)
- Best identified at level of cricoid cartilage
- ATA 2015: visual identification of RLN is strongly recommended in ALL cases
- Intraoperative neuromonitoring (IONM) may reduce transient RLN injury (especially in high-risk cases); does not reduce permanent injury significantly
External Branch of Superior Laryngeal Nerve (EBSLN)
- Supplies cricothyroid muscle (only intrinsic laryngeal muscle NOT supplied by RLN)
- Injury: loss of ability to raise pitch - damages professional singers
- Cernea Type 2A and 2B are at high risk during superior pole dissection
- Protected by: ligating superior pole vessels close to thyroid capsule
Parathyroid Glands
- Superior parathyroids - more constant in position, near superior pole, posterior surface of thyroid
- Inferior parathyroids - more variable, near inferior pole, anterior to RLN
- Blood supply: branches of inferior thyroid artery (primarily)
- Identification: yellowish-tan, soft; bleeds when cut (unlike fat which does not)
- If inadvertently removed: confirm on frozen section + autotransplant into sternocleidomastoid
7. COMPLICATIONS - VERY HIGH YIELD
A. Recurrent Laryngeal Nerve Injury
| Type | Presentation | Timing |
|---|---|---|
| Unilateral | Hoarseness, weak voice, bovine cough | Immediate post-op |
| Bilateral | Stridor, respiratory distress - emergency, may need tracheostomy | Immediate post-op |
| Transient | Resolves within weeks-months (neurapraxia) | - |
| Permanent | Persistent >6 months (neurotmesis) | - |
- Incidence: ~1-2% permanent in experienced hands
- Management of unilateral permanent: voice therapy, medialization procedures (thyroplasty)
B. Hypoparathyroidism / Hypocalcemia
- Most common serious complication after total thyroidectomy
- Causes: devascularization, manipulation, or inadvertent removal of parathyroids
- Transient (most common) vs permanent (< 1-2%)
- Hungry Bone Syndrome - especially in hyperthyroid patients after total thyroidectomy: severe prolonged hypocalcemia despite normal PTH (high bone turnover absorbs calcium); associated low phosphate, low magnesium, high potassium
Symptoms of hypocalcemia:
- Perioral tingling, fingertip numbness
- Chvostek's sign (tapping facial nerve - facial twitch)
- Trousseau's sign (BP cuff inflation - carpopedal spasm)
- Severe: tetany, laryngospasm, seizures
Management:
- Oral calcium + calcitriol supplementation
- Monitor serum calcium / intraoperative PTH post-closure
- Preoperative calcitriol in high-risk patients (Graves' disease, reoperative surgery)
C. Postoperative Neck Hematoma
- Incidence ~1%
- Presentation: neck swelling, pain, respiratory distress (compresses trachea)
- Emergency management: open the wound at bedside immediately to decompress, then return to OR for formal exploration
- Can be life-threatening due to airway compromise
D. Thyroid Storm (Thyrotoxic Crisis)
- Occurs in 1-5% of hospitalized thyrotoxic patients
- Triggered by: surgery (especially if patient not euthyroid), trauma, infection, cessation of antithyroid drugs
- Burch-Wartofsky scoring system (1993) - grades severity based on temperature, CNS, GI/hepatic, cardiovascular, precipitating event
- Treatment: PTU (blocks synthesis + peripheral conversion), beta-blockers, hydrocortisone, Lugol's iodine (after PTU), cooling, supportive care
E. External Branch SLN Injury
- Loss of high-pitched phonation, voice fatigue
- Missed on routine post-op voice assessment (cord moves normally)
F. Other Complications
- Tracheal injury (rare)
- Esophageal injury (rare)
- Chylous fistula (left-sided dissections, thoracic duct injury)
- Wound infection, seroma
- Hypothyroidism (expected after total thyroidectomy - treated with levothyroxine)
8. SPECIFIC CLINICAL SCENARIOS
Graves' Disease Surgery
- Render euthyroid pre-op: carbimazole + propranolol
- Add Lugol's iodine for 10 days before surgery (Wolff-Chaikoff effect - reduces vascularity)
- Preferred operation: total or near-total thyroidectomy
- Higher risk of hypoparathyroidism (start prophylactic calcitriol)
Thyroid Cancer Surgery
- Papillary / Follicular (DTC): total thyroidectomy for tumors > 4 cm, bilateral disease, extrathyroidal extension, nodal disease; lobectomy acceptable for low-risk unifocal < 4 cm
- Medullary thyroid cancer: total thyroidectomy + central neck dissection (Level VI); check calcitonin and CEA; rule out pheochromocytoma before surgery (RET mutation, MEN2)
- Anaplastic: poor prognosis; surgery rarely curative; role is airway management
Substernal Goiter
- Usually extirpated via cervical approach (same Kocher incision)
- Median sternotomy or thoracotomy needed if: truly intrathoracic blood supply, tumor components, or unable to deliver via neck
- Higher risk of RLN injury (nerve distorted)
Minimally Invasive Thyroidectomy
- Mini-incision: 3 cm, no flap, deliver thyroid into wound
- Endoscopic approaches: axillary, anterior chest, breast - scar-free neck
- Transoral (through mouth) - newest approach
- Robotic assistance available for all remote-access approaches
- Benefits over open not clearly established for all patients
9. NEET PG HIGH-YIELD QUICK FACTS
| Fact | Answer |
|---|---|
| Most common complication of thyroidectomy | Transient hypocalcemia |
| Most common permanent complication | RLN injury OR permanent hypoparathyroidism |
| Nerve at risk during superior pole ligation | EBSLN (external branch of SLN) |
| Nerve at risk at ligament of Berry | RLN |
| Incision used in thyroidectomy | Kocher collar incision |
| Position during thyroidectomy | Supine, neck extended, sandbag between scapulae |
| Pyramidal lobe frequency | ~80% of patients; extends from isthmus toward hyoid |
| Remission after subtotal thyroidectomy for Graves | ~70-80%; recurrence risk related to remnant size |
| Nobel Prize for thyroid surgery | Theodor Kocher, 1909 |
| Blood supply to parathyroids | Inferior thyroid artery (primarily) |
| Dunhill operation | Unilateral total lobectomy + contralateral subtotal for Graves' |
| Wolff-Chaikoff effect | High iodine load transiently suppresses thyroid synthesis - basis for Lugol's pre-op |
| "Singer's nerve" | External branch of SLN (cricothyroid muscle) |
| Autotransplantation of parathyroid | Into sternocleidomastoid muscle |
| Emergency action for neck hematoma | Open wound immediately + return to OR |
10. POSTOPERATIVE FOLLOW-UP
- After total thyroidectomy: levothyroxine replacement (weight-based); serum calcium monitoring 1-2 days post-op; TSH suppression if cancer
- After lobectomy: thyroid function test at 6 weeks; ~15-20% will need levothyroxine if remaining lobe insufficient
- Thyroid cancer follow-up: serum thyroglobulin + neck ultrasound; radioiodine ablation if indicated (total thyroidectomy needed for RAI to work)
- Most patients discharged within 2-24 hours; return to normal activity within 1 week
Sources: Sabiston Textbook of Surgery 21e, Schwartz's Principles of Surgery 11e, Current Surgical Therapy 14e, Fischer's Mastery of Surgery 8e
This is a shared conversation. Sign in to Orris to start your own chat.