Respiratory alkalosis full details for md exams 10marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from Harrison's 22e, Costanzo Physiology, Brenner & Rector's Kidney, Morgan & Mikhail's Anesthesiology, and Comprehensive Clinical Nephrology. Let me compile the full, exam-ready answer.
Respiratory Alkalosis - Complete MD Exam Answer (10 Marks)
Definition
Respiratory alkalosis is a primary acid-base disorder characterized by a decrease in arterial PaCO2 (hypocapnia) below 35 mmHg, resulting in a rise in arterial pH above 7.45 (alkalemia). It is caused by alveolar hyperventilation, where CO2 output by the lungs exceeds its metabolic production by tissues.
- Harrison's Principles of Internal Medicine 22e, Ch. 50
- Brenner & Rector's The Kidney, Ch. 16
Pathophysiology / Mechanism
Alveolar hyperventilation increases CO2 elimination, reducing PaCO2. By the Henderson-Hasselbalch equation:
pH = 6.1 + log [HCO3-] / (0.03 × PaCO2)
As PaCO2 falls, the ratio [HCO3-]/PaCO2 rises, causing alkalemia. The decreased PaCO2 also lowers [HCO3-] slightly by mass action (CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3-).
- Costanzo Physiology 7e, Ch. 7
Causes (Etiology)
1. Central Stimulation of Respiratory Center
| Cause | Examples |
|---|---|
| Psychogenic / anxiety | Hysterical hyperventilation, panic attacks |
| Pain | Any acute pain |
| CNS disease | Stroke, tumor, meningitis, encephalitis, head injury |
| Fever / sepsis | Gram-negative septicemia (may precede fever/hypoxemia) |
| Drugs | Salicylates (most common drug cause - direct chemoreceptor stimulation), theophylline, aminophylline, analeptics (doxapram) |
| Hormonal | Progesterone (pregnancy - lowers PaCO2 by 5-10 mmHg) |
| Hepatic failure | Severity correlates with degree of hepatic insufficiency |
2. Peripheral Stimulation (Hypoxemia-mediated)
- High altitude
- Pneumonia, pulmonary embolism
- Congestive heart failure
- Non-cardiogenic pulmonary edema
- Asthma
- Severe anemia
3. Iatrogenic / Miscellaneous
- Mechanical ventilation (ventilator-induced)
- Metabolic encephalopathies
Key: Chronic respiratory alkalosis is the most common acid-base disturbance in critically ill patients and portends a poor prognosis when severe.
- Morgan & Mikhail's Clinical Anesthesiology 7e, Table 50-5
- Harrison's 22e, p. 419
Compensatory Responses
Respiratory alkalosis triggers two phases of compensation:
Phase 1 - Acute: Chemical Buffering (minutes)
- Nonbicarbonate cellular buffers (proteins, phosphates in ICF and RBCs) titrate down HCO3-
- CO2 leaves cells; intracellular pH rises
- Rule: For each 10 mmHg ↓ in PaCO2, [HCO3-] falls by ~2 mEq/L
- pH rises by ~0.08 units per 10 mmHg fall in PaCO2
Phase 2 - Chronic: Renal Compensation (begins 2-6 hours; complete in 3-5 days)
- Decreased renal excretion of H+ as titratable acid and NH4+
- Decreased reabsorption of filtered HCO3-
- Decreased synthesis of new HCO3-
- Rule: For each 10 mmHg ↓ in PaCO2, [HCO3-] falls by 4-5 mEq/L
- pH rises by only ~0.03 units per 10 mmHg fall in PaCO2
Key fact: Respiratory alkalosis is the only acid-base disorder in which physiologic compensation can return pH fully to normal (7.35-7.45). This is unique.
- Brenner & Rector's The Kidney, p. [block10]
- Costanzo Physiology 7e, p. 341
ABG Interpretation Summary Table
| Parameter | Acute R. Alkalosis | Chronic R. Alkalosis |
|---|---|---|
| pH | >7.45 (often >7.55) | Near normal or slightly elevated |
| PaCO2 | ↓ (primary) | ↓ (primary) |
| HCO3- | Slightly ↓ (~2 per 10 mmHg) | More ↓ (~4-5 per 10 mmHg) |
| K+ | Slightly ↓ | Slightly ↓ |
| Cl- | ↑ | ↑ |
| Ca2+ (ionized) | ↓ | ↓ |
HCO3- rarely falls below 12 mmol/L in pure respiratory alkalosis.
Clinical Features
Neurological
- Dizziness, mental confusion, seizures - due to reduced cerebral blood flow (hypocapnia causes cerebral vasoconstriction)
- Paresthesias and circumoral numbness - from decreased ionized Ca2+ (Ca2+ binds more to albumin at alkaline pH)
- Tetany (rare) - same mechanism as above
- Inability to take an adequate breath
Cardiovascular
- Minimal in awake conscious patients
- In anesthetized/ventilated patients: fall in cardiac output and BP (due to anesthesia effects on heart rate, SVR, and venous return)
- Cardiac arrhythmias (especially in pre-existing heart disease) - due to left shift of O2-Hb dissociation curve (Bohr effect), reducing O2 delivery to myocardium
Metabolic/Electrolyte Effects
- Hypokalemia: alkalemia drives K+ intracellularly (exchange with H+); usually minor
- Hypophosphatemia: intracellular shift of PO4²-
- Hypocalcemia (ionized): more Ca2+ binds to albumin at high pH
- Left shift of O2-Hb dissociation curve (Bohr effect): Hb holds O2 more tightly, reducing tissue O2 unloading
- Bronchoconstriction: respiratory alkalosis increases bronchial smooth muscle tone
- Decreased pulmonary vascular resistance: opposite to bronchoconstriction
Hyperventilation Syndrome
-
A clinical entity where anxiety/panic drives hyperventilation, causing PaCO2 15-30 mmHg
-
Symptoms of chest tightness, dizziness, paresthesias can perpetuate the cycle
-
No hypoxemia on ABG
-
Diagnosis by exclusion (rule out PE, CAD, hyperthyroidism)
-
Morgan & Mikhail 7e; Harrison's 22e; Brenner & Rector's
Diagnosis
- ABG: pH >7.45, PaCO2 <35 mmHg, HCO3- appropriately decreased
- Serum electrolytes: ↓K+, ↑Cl-, ↓ionized Ca2+
- Determine if acute vs. chronic using compensation formulas above
- Search for underlying cause
Treatment
Treat the Underlying Cause (most important)
- Treat sepsis, hypoxemia (oxygen therapy), hepatic failure, pain, fever
- Stop/adjust offending drugs (salicylates, theophylline)
- Reassure patients with hyperventilation syndrome; rebreathing from paper bag raises PaCO2
Ventilator-Induced Respiratory Alkalosis
- Increase dead space, reduce tidal volume, or change ventilation mode (e.g., assist-control to mandatory ventilation)
- If persistent: sedation with or without skeletal muscle paralysis
Severe Alkalemia (pH >7.55-7.60)
- IV hydrochloric acid (HCl), arginine chloride, or ammonium chloride may be indicated
- Acetazolamide (carbonic anhydrase inhibitor) to reduce HCO3- reabsorption
- Ultrafiltration with low HCO3- dialysate in renal failure
Hyperventilation Syndrome
- Reassurance, rebreathing from paper bag
- Attention to underlying psychological stress
- Beta-blockers may help peripheral hyperadrenergic symptoms
- Antidepressants and sedatives are NOT routinely recommended
Treatment flowchart from Comprehensive Clinical Nephrology:
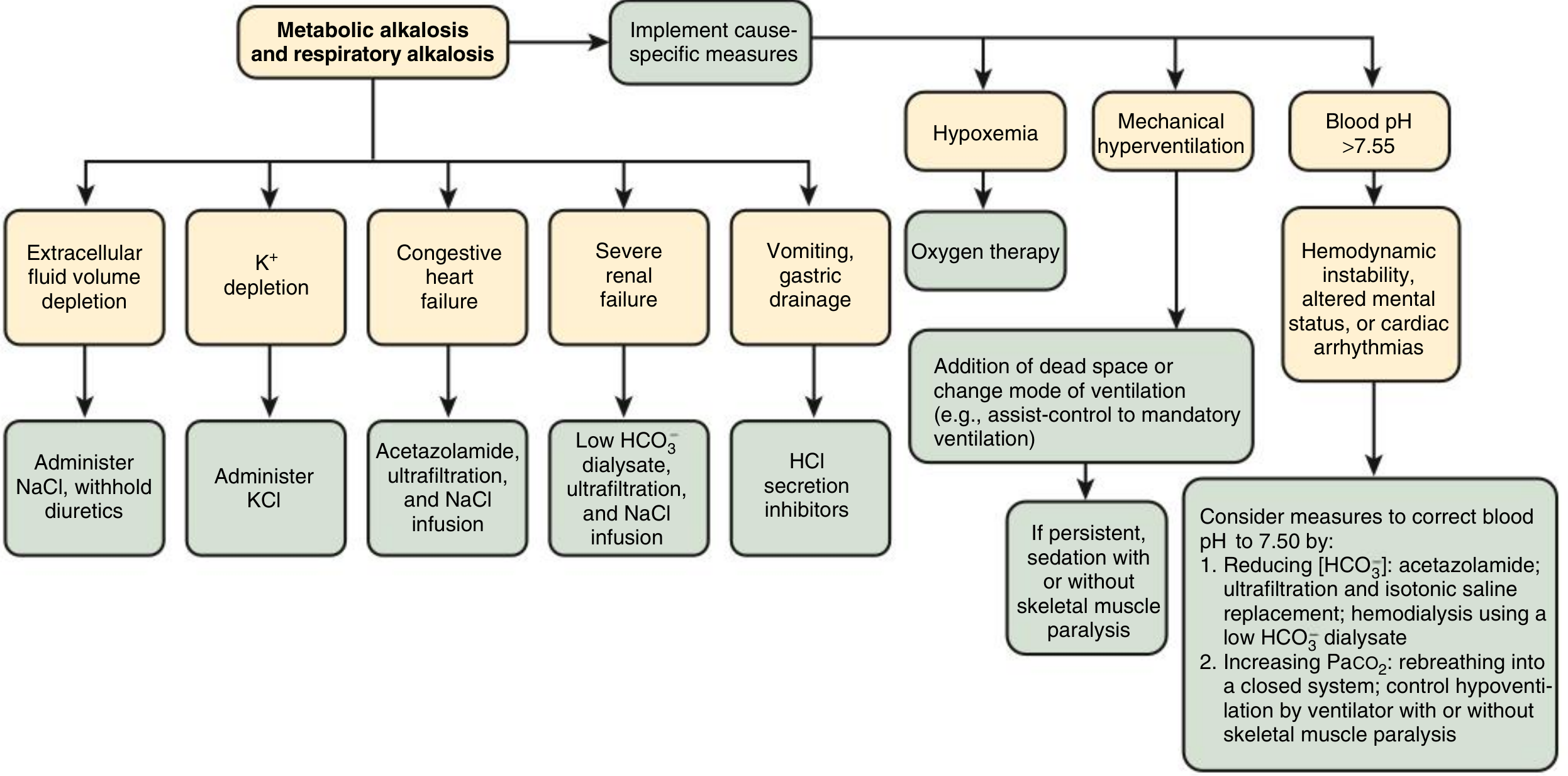
Fig. 15.7 - Treatment of metabolic alkalosis and respiratory alkalosis (Comprehensive Clinical Nephrology 7e)
Mixed Disorders Involving Respiratory Alkalosis
Respiratory alkalosis commonly occurs as part of a mixed disorder:
- Mixed metabolic acidosis + respiratory alkalosis: seen in salicylate poisoning (salicylates cause both metabolic acidosis via organic acid accumulation AND respiratory alkalosis via direct medullary stimulation). pH may be near normal but both disorders are present.
- Mixed respiratory alkalosis + metabolic alkalosis: seen in hepatic failure with vomiting/diuretics
- Approach with caution - correcting one arm alone can create severe imbalance in the other
High-Yield Points for MD Exams
| Point | Detail |
|---|---|
| Only disorder fully compensated | Chronic respiratory alkalosis (pH can normalize) |
| Most common drug cause | Salicylates (direct medullary chemoreceptor stimulation) |
| Most common cause in critically ill | Respiratory alkalosis (worst prognosis when severe) |
| Compensation formula - Acute | HCO3- ↓ 2 mEq/L per 10 mmHg ↓ PaCO2 |
| Compensation formula - Chronic | HCO3- ↓ 4-5 mEq/L per 10 mmHg ↓ PaCO2 |
| Minimum HCO3- in pure respiratory alkalosis | ~12 mmol/L |
| Mechanism of tingling/tetany | ↑ protein-bound Ca2+, ↓ ionized Ca2+ |
| Mechanism of dizziness | Cerebral vasoconstriction from ↓ PaCO2 |
| Earliest sign of gram-negative sepsis | Respiratory alkalosis (before fever, hypoxemia, hypotension) |
| Pregnancy-related | Chronic respiratory alkalosis (progesterone lowers PaCO2 by 5-10 mmHg) |
| O2-Hb curve | Left shift (Bohr effect) - impairs O2 unloading |
Sources:
- Harrison's Principles of Internal Medicine 22e, Ch. 50 (Acid-Base Disturbances)
- Costanzo Physiology 7e, Ch. 7 (Acid-Base Physiology)
- Brenner & Rector's The Kidney (2-Volume Set), Ch. 16
- Morgan & Mikhail's Clinical Anesthesiology 7e, Ch. 50
- Comprehensive Clinical Nephrology 7e, Ch. 15
- Rosen's Emergency Medicine, Ch. 113
This is a shared conversation. Sign in to Orris to start your own chat.