brachial plexuses ,mammary gland, median nerve, radial nerve, ulnar nerve , shoulder joint, elbow joint , axillary artery, radial artery, brachial aretry, scalp, parotid gland, thyroid gland, cavernous sinus, palatine tonsil, tongue, lateral wall of nose, posterior wall of nose , middle ear , facial nerve. these are the important questions for my anatomy university exam give me a proper schedule to complete them in a week. the time that i can spend on these topics is 2 hrs a day
anatomy study schedule brachial plexus upper limb head neck exam preparation tips
7-Day Anatomy Exam Schedule
2 Hours/Day | 20 Topics | Exam-Ready by Sunday
Grouping Logic
| Cluster | Topics |
|---|---|
| Upper Limb - Nerves | Brachial plexus, Median, Radial, Ulnar |
| Upper Limb - Vessels & Joints | Axillary A, Brachial A, Radial A, Shoulder joint, Elbow joint |
| Breast | Mammary gland |
| Head & Neck - Glands | Parotid, Thyroid |
| Head & Neck - Sinuses & Ear | Cavernous sinus, Middle ear |
| Oral & Pharyngeal | Tongue, Palatine tonsil |
| Nasal & Scalp | Scalp, Lateral wall of nose, Posterior wall of nose |
| Nerve | Facial nerve |
Day-by-Day Schedule
DAY 1 - Monday, June 29
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 1:20 | Brachial Plexus | Roots (C5-T1), Trunks, Divisions, Cords, Branches (RTDCB). Mnemonic: "Robert Taylor Drinks Cold Beer." Pre/post-ganglionic injuries. Erb's palsy (C5-C6), Klumpke's palsy (C8-T1). Axillary, musculocutaneous, radial, median, ulnar nerve origins. Long thoracic, dorsal scapular, suprascapular nerves. |
| 1:20 - 2:00 | Mammary Gland | Structure (15-20 lobes), Cooper's ligaments, lymphatic drainage (axillary - 75%, internal mammary), blood supply (internal thoracic, lateral thoracic, intercostals), nerve supply (anterior & lateral cutaneous branches of intercostals 2-6). Clinical: peau d'orange, carcinoma lymph spread. |
Tip: Draw the brachial plexus from scratch at least 3 times before bed. It's the hardest topic - give it maximum mental energy.
DAY 2 - Tuesday, June 30
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:40 | Median Nerve | Origin (lateral + medial cords, C5-T1). Course (arm, cubital fossa, forearm, carpal tunnel, hand). Muscles (LOAF in hand: Lateral 2 lumbricals, Opponens pollicis, Abductor pollicis brevis, Flexor pollicis brevis). Injury: carpal tunnel - ape hand, Pope's blessing. Anterior interosseous nerve branch. |
| 0:40 - 1:20 | Radial Nerve | Origin (posterior cord, C5-T1). Spiral groove of humerus - wrist drop. Deep branch (posterior interosseous nerve). Superficial branch (sensory). Muscles (all extensors + brachioradialis). Injuries at different levels. |
| 1:20 - 2:00 | Ulnar Nerve | Origin (medial cord, C8-T1). Course behind medial epicondyle - "funny bone." Cubital tunnel, Guyon's canal. Muscles (hypothenar, medial 2 lumbricals, all interossei, adductor pollicis). Claw hand (ring + little fingers). Froment's sign. |
Tip: Make a comparison table: median vs radial vs ulnar - origin, course, muscles, injury, clinical sign. This is a favourite exam format.
DAY 3 - Wednesday, July 1
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:40 | Shoulder Joint | Ball-and-socket, most mobile/least stable joint. Articular surfaces, capsule, ligaments (glenohumeral, coracohumeral, coracoacromial). Rotator cuff muscles (SITS: Supraspinatus, Infraspinatus, Teres minor, Subscapularis). Bursae. Relations. Dislocation directions (anterior most common - axillary nerve injury). |
| 0:40 - 1:20 | Elbow Joint | Hinge joint. Bones (humerus, radius, ulna). Ligaments (medial/ulnar collateral, lateral/radial collateral, annular). Cubital fossa contents (from lateral to medial: Radial Nerve, Biceps tendon, Brachial Artery, Median Nerve - "Really Be Brave Man"). Injuries: pulled elbow, golfer's vs tennis elbow. |
| 1:20 - 2:00 | Axillary Artery | 3 parts relative to pectoralis minor. Part 1 (1 branch: superior thoracic). Part 2 (2 branches: thoracoacromial, lateral thoracic). Part 3 (3 branches: subscapular, anterior/posterior circumflex humeral). Relations, axillary vein, brachial plexus cords. |
DAY 4 - Thursday, July 2
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:25 | Brachial Artery | Continuation of axillary. Course (medial to biceps, cubital fossa). Branches (profunda brachii, superior/inferior ulnar collaterals, nutrient artery to humerus). Bifurcation at radial neck into radial + ulnar arteries. Clinical: blood pressure measurement site. |
| 0:25 - 0:50 | Radial Artery | Course (lateral forearm, anatomical snuffbox, palm). Branches (radial recurrent, superficial palmar branch, princeps pollicis, deep palmar arch). Pulse palpation at wrist. Allen's test. |
| 0:50 - 1:20 | Scalp | 5 layers (SCALP): Skin, dense Connective tissue, Aponeurosis (epicranial), Loose areolar tissue, Pericranium. Dangerous layer = loose areolar (infection spreads). Blood supply (supratrochlear, supraorbital, superficial temporal, posterior auricular, occipital arteries). Sensory innervation (V1, V2 anteriorly; C2, C3 posteriorly). |
| 1:20 - 2:00 | Parotid Gland | Largest salivary gland. Location (retromandibular fossa). Contents (facial nerve VII superficial, retromandibular vein deep to VII, external carotid artery deepest). Stensen's duct (opposite upper 2nd molar). Blood supply, venous drainage. Frey's syndrome (auriculotemporal nerve). Mumps, parotid tumours. |
DAY 5 - Friday, July 3
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:45 | Thyroid Gland | H-shaped, isthmus at 2nd-4th tracheal rings. Capsule and surgical capsule. Blood supply (superior thyroid artery from ECA, inferior thyroid artery from thyrocervical trunk). Veins (superior, middle, inferior - drain into IJV except inferior which drains into brachiocephalic). Lymphatics. Relations (parathyroids, RLN - close to inferior thyroid artery, pyramidal lobe). Clinical: RLN injury in thyroidectomy - hoarseness. |
| 0:45 - 1:20 | Cavernous Sinus | Location (either side of sella turcica). Contents: CN III, IV, V1, V2, VI and internal carotid artery (+ sympathetic plexus). VI is in free - most vulnerable to raised pressure. Communications (superior/inferior petrosal sinuses, ophthalmic veins, pterygoid plexus). Thrombosis: dangerous area of face (upper lip, nose). Clinical signs. |
| 1:20 - 2:00 | Middle Ear (Tympanic Cavity) | 6 walls (roof = tegmen tympani, floor = jugular wall, lateral = tympanic membrane, medial = labyrinthine, anterior = carotid, posterior = mastoid). Ossicles (malleus, incus, stapes). Muscles (tensor tympani - CN V3; stapedius - CN VII). Chorda tympani (branch of VII - taste anterior 2/3 tongue). Eustachian tube. Otitis media, mastoiditis complications. |
DAY 6 - Saturday, July 4
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:35 | Tongue | Anterior 2/3 vs posterior 1/3. Mucosa (filiform, fungiform, circumvallate, foliate papillae). Muscles - intrinsic + extrinsic (genioglossus, hyoglossus, styloglossus, palatoglossus). Motor: XII (hypoglossal) except palatoglossus (CN X). Sensory: anterior 2/3 - general (V3/lingual), taste (VII/chorda tympani); posterior 1/3 - both (IX/glossopharyngeal). Blood supply (lingual artery). |
| 0:35 - 1:05 | Palatine Tonsil | Location (between palatoglossal and palatopharyngeal arches - tonsillar fossa). Capsule (from pharyngobasilar fascia). Blood supply: main = tonsillar branch of facial artery; also ascending pharyngeal, ascending palatine, greater palatine, lingual artery. Paratonsillar vein (bleeds in tonsillectomy). Waldeyer's ring. Deep to tonsil: internal carotid artery - danger in tonsillectomy. |
| 1:05 - 1:35 | Lateral Wall of Nose | 3 conchae (superior, middle, inferior). 4 meatuses. Openings: inferior meatus (nasolacrimal duct), middle meatus (frontal, maxillary, anterior ethmoidal sinuses - hiatus semilunaris), superior meatus (posterior ethmoidal), sphenoethmoidal recess (sphenoidal sinus). Kiesselbach's area (Little's area) - common nosebleed site. |
| 1:35 - 2:00 | Posterior Wall of Nose (Nasopharynx/Posterior Choana) | Choanae boundaries (vomer medially, palatine bone laterally, sphenoid above, horizontal plate of palatine below). Adenoids (pharyngeal tonsil) on roof. Eustachian tube opening on lateral wall. Salpingopharyngeal fold. Fossa of Rosenmuller (pharyngeal recess) - nasopharyngeal carcinoma site. Blood supply of nasal cavity (sphenopalatine artery - main; ethmoidal arteries, facial artery). |
DAY 7 - Sunday, July 5
| Time | Topic | Focus Points |
|---|---|---|
| 0:00 - 0:50 | Facial Nerve (CN VII) | Course: internal auditory meatus → geniculate ganglion → 3 branches in petrous bone (greater petrosal nerve, nerve to stapedius, chorda tympani) → exits at stylomastoid foramen → parotid gland → 5 terminal branches (TMPZB: Temporal, Zygomatic, Buccal, Marginal mandibular, Cervical). Motor to all muscles of facial expression (except buccinator - it's supplied but also by V3 for proprioception). Parasympathetics (lacrimal gland via pterygopalatine, submandibular/sublingual via submandibular ganglion). LMN vs UMN facial palsy. Bell's palsy. |
| 0:50 - 1:30 | Rapid Revision | Flip back through all topics in 40 mins. Focus on: brachial plexus diagram, nerve injury signs table, cavernous sinus contents, thyroid surgical dangers, Kiesselbach's area, ossicles of middle ear, tongue innervation summary. |
| 1:30 - 2:00 | Self-Test | Cover your notes. Write from memory: (1) branches of axillary artery, (2) contents of cavernous sinus, (3) 5 branches of facial nerve, (4) muscles supplied by ulnar nerve, (5) blood supply of tonsil. Check answers. Flag weak areas. |
Key Mnemonics Summary
| Topic | Mnemonic |
|---|---|
| Brachial plexus structure | Roots, Trunks, Divisions, Cords, Branches = "Robert Taylor Drinks Cold Beer" |
| Scalp layers | SCALP |
| Rotator cuff | SITS (Supraspinatus, Infraspinatus, Teres minor, Subscapularis) |
| Cubital fossa (lat → med) | "Really Be Brave Man" (Radial N, Biceps tendon, Brachial A, Median N) |
| Median nerve hand muscles | LOAF |
| Facial nerve branches | To My Zulu Boy Comes (Temporal, Marginal mandibular, Zygomatic, Buccal, Cervical) |
| Axillary artery branches | 1-2-3 rule (parts 1, 2, 3 give 1, 2, 3 branches respectively) |
General Tips
- Draw, don't just read. For brachial plexus, facial nerve, and cavernous sinus - sketching the diagram burns it into memory far faster than re-reading.
- Clinical correlations = exam marks. Examiners love asking about RLN and thyroidectomy, axillary nerve and shoulder dislocation, cavernous sinus thrombosis, and facial nerve palsy. Know the clinical angle for each topic.
- Active recall over passive reading. After each session, close the book and write down everything you remember. Then check.
- Prioritise Day 1 and Day 7. Brachial plexus is the most complex topic and facial nerve is the most commonly examined cranial nerve - these deserve your sharpest focus.
- Group study on Day 7 if possible. Teaching a classmate the facial nerve or brachial plexus in the last 30 minutes is one of the best retention strategies.
can u give any mnemonic to remember all the brachial plexus branches
Brachial Plexus Branches - Complete Mnemonics
First, the Structure (RTDCB)
"Robert Taylor Drinks Cold Beer" Roots → Trunks → Divisions → Cords → Branches
ROOTS Level Branches
| Branch | Root |
|---|---|
| Dorsal Scapular Nerve | C5 |
| Long Thoracic Nerve | C5, C6, C7 |
"My Aunt Keeps Selling Drugs" - just remember 2 branches at root level: Dorsal Scapular + Long Thoracic Or simply: "Don't Lose" (Dorsal scapular, Long thoracic)
TRUNK Level Branches
| Branch | Origin |
|---|---|
| Nerve to Subclavius | Upper trunk |
| Suprascapular Nerve | Upper trunk |
"Upper trunk gives 2 S's" → Subclavius + Suprascapular
CORDS Level Branches
LATERAL CORD → "My Lateral Cord Makes People Move"
| Letter | Branch |
|---|---|
| L | Lateral pectoral nerve |
| M | Musculocutaneous nerve |
| M | Medial root of median nerve (lateral cord contributes) |
Short form: "Lateral Cord = LMM" (Lateral pectoral, Musculocutaneous, Median contribution)
MEDIAL CORD → "My Medial Cord Makes Many More Nerves"
| Branch | Memory |
|---|---|
| Medial pectoral nerve | |
| Medial cutaneous nerve of arm | |
| Medial cutaneous nerve of forearm | |
| Ulnar nerve | |
| Medial root of median nerve |
"Men Prefer Making Unusual Moves" Medial pectoral, Medial cutaneous arm, Medial cutaneous forearm, Ulnar, Median (medial root)
Or think: Medial cord = 5 branches, all start with M except Ulnar
POSTERIOR CORD → "ULTRA" ✅ (the most testable one)
| Letter | Branch |
|---|---|
| U | Upper subscapular nerve |
| T | Thoracodorsal nerve (nerve to latissimus dorsi) |
| L | Lower subscapular nerve |
| R | Radial nerve |
| A | Axillary nerve |
"ULTRA" - Posterior cord gives 5 branches, remember ULTRA
THE TERMINAL BRANCHES (5 major nerves)
"My Aunt Reads Uncle's Magazines"
| Letter | Nerve | Cord Origin |
|---|---|---|
| M | Musculocutaneous | Lateral |
| A | Axillary | Posterior |
| R | Radial | Posterior |
| U | Ulnar | Medial |
| M | Median | Lateral + Medial |
Full Picture on One Page
ROOTS (C5-T1)
├── Dorsal Scapular (C5) } "Don't Lose"
└── Long Thoracic (C5,6,7) }
TRUNKS (Upper only)
├── Nerve to Subclavius } "Two S's from
└── Suprascapular nerve } Upper trunk"
CORDS
├── LATERAL → LMM
│ Lateral pectoral
│ Musculocutaneous
│ Median (lateral root)
│
├── MEDIAL → "Men Prefer Making Unusual Moves"
│ Medial pectoral
│ Med. cut. nerve of arm
│ Med. cut. nerve of forearm
│ Ulnar
│ Median (medial root)
│
└── POSTERIOR → ULTRA
Upper subscapular
Thoracodorsal
Lower subscapular
Radial
Axillary
Quick Exam Hack
- Lateral = 3
- Medial = 5
- Posterior = 5
Remember: "3 - 5 - 5" or "Lateral is the smallest cord"
divisions of brachial plexus
Divisions of the Brachial Plexus
What Are Divisions?
They sit behind the clavicle (retroclavicular / infraclavicular region)
The 6 Divisions
| Trunk | Anterior Division | Posterior Division |
|---|---|---|
| Upper trunk (C5, C6) | Anterior division of upper trunk | Posterior division of upper trunk |
| Middle trunk (C7) | Anterior division of middle trunk | Posterior division of middle trunk |
| Lower trunk (C8, T1) | Anterior division of lower trunk | Posterior division of lower trunk |
How Divisions Form the Cords
ANTERIOR divisions:
Upper + Middle ──────────────────→ LATERAL CORD
Lower ───────────────────────────→ MEDIAL CORD
POSTERIOR divisions:
Upper + Middle + Lower ───────────→ POSTERIOR CORD
| Cord | Formed by | Spinal levels |
|---|---|---|
| Lateral cord | Anterior div. of Upper + Middle trunk | C5, C6, C7 |
| Medial cord | Anterior div. of Lower trunk | C8, T1 |
| Posterior cord | Posterior div. of ALL 3 trunks | C5, C6, C7, C8, T1 |
The Functional Logic (Why It Makes Sense)
Anterior divisions → supply flexor compartments (front of limb) Posterior divisions → supply extensor compartments (back of limb)
Memory Trick
"All Posterior divisions go Posterior - no exceptions" "Anterior divisions SPLIT - upper+middle go Lateral, lower goes Medial"
Upper trunk ──── Ant ──┐
├──→ LATERAL CORD
Middle trunk ─── Ant ──┘
Lower trunk ──── Ant ──────→ MEDIAL CORD
Upper trunk ──── Post ─┐
├──→ POSTERIOR CORD
Middle trunk ─── Post ─┤
│
Lower trunk ──── Post ─┘
Important Exam Points
| Point | Detail |
|---|---|
| No branches arise from divisions | Divisions are purely a regrouping zone - this is a classic MCQ trap |
| Where are divisions located? | Behind the clavicle (between scalene muscles and axilla) |
| Posterior cord is the widest | Gets input from C5 to T1 (all roots) |
| Lateral cord = C5, 6, 7 only | This is why median nerve has both lateral and medial roots (to get C8, T1 input) |
| Why does median nerve have two roots? | Lateral root (C5-7 from lateral cord) + Medial root (C8-T1 from medial cord) unite to form the complete median nerve |
One-Line Summary for Quick Revision
"3 trunks → 6 divisions (each trunk splits into ant + post) → 3 cords (ant upper+mid = lateral, ant lower = medial, all post = posterior)"
brachial plexus line diagram to present in exam
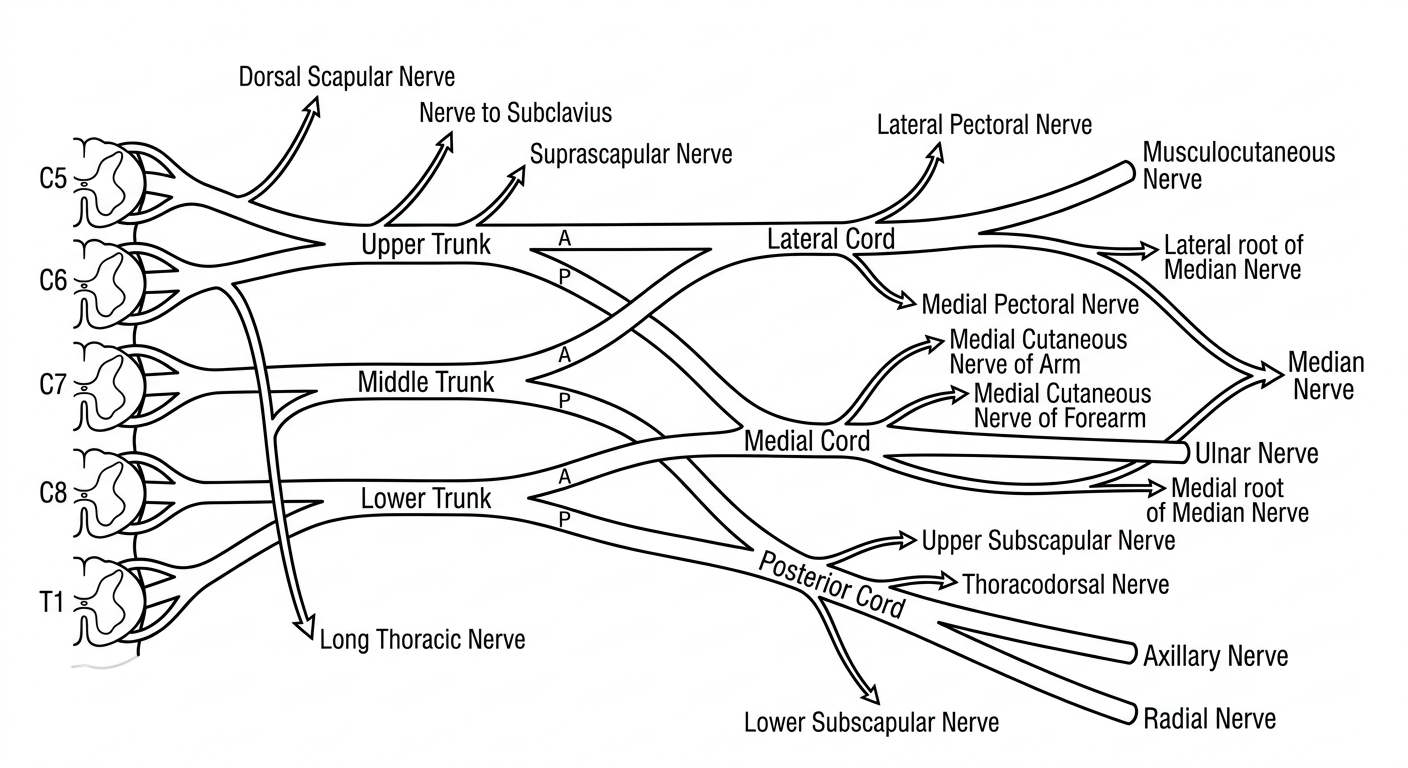
How to Draw It Fast in Exam (Step-by-Step)
- C5 + C6 → Upper trunk
- C7 → Middle trunk
- C8 + T1 → Lower trunk
- A of Upper + A of Middle → Lateral cord
- A of Lower → Medial cord
- P of ALL three → Posterior cord
What to Label for Maximum Marks
| Must Label | Don't Forget |
|---|---|
| All 5 roots (C5-T1) | Dorsal scapular (C5) at root level |
| All 3 trunks | Long thoracic (C5,6,7) at root level |
| All 6 divisions (A & P) | Suprascapular + Nerve to subclavius at upper trunk |
| All 3 cords | ULTRA branches of posterior cord |
| All 5 terminal branches | Median nerve = two roots uniting (M shape) |
Pro tip: Draw the median nerve as an "M" or "V" shape where the lateral and medial roots unite - examiners specifically look for this and it shows you understand the anatomy.
Make a comparison chart of median vs radial vs ulnar nerve injuries
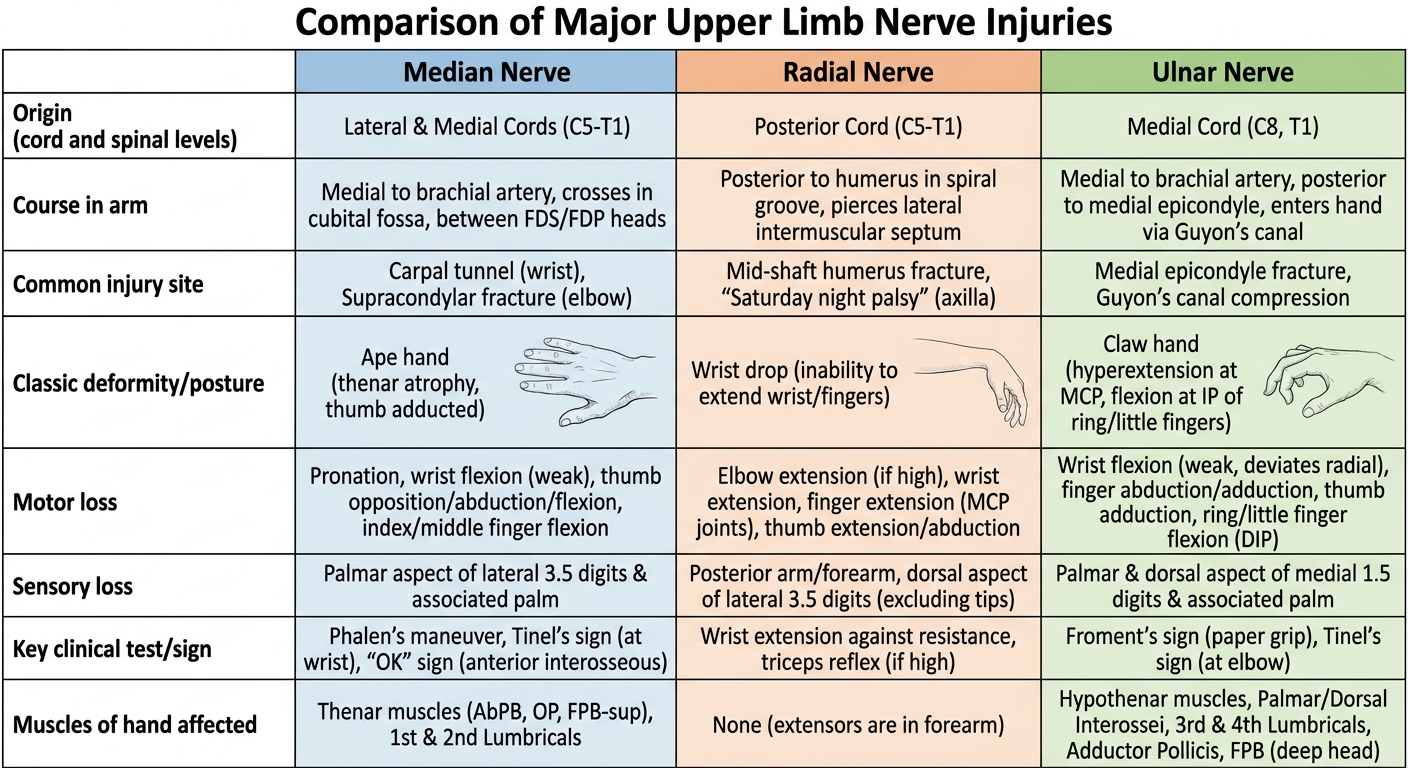
Median vs Radial vs Ulnar - Complete Comparison
| Feature | Median Nerve | Radial Nerve | Ulnar Nerve |
|---|---|---|---|
| Cord origin | Lateral + Medial cords | Posterior cord | Medial cord |
| Spinal levels | C5, C6, C7, C8, T1 | C5, C6, C7, C8, T1 | C8, T1 |
| Common injury site | Carpal tunnel (wrist) | Spiral groove of humerus | Behind medial epicondyle |
| Classic cause | Carpal tunnel syndrome, wrist laceration | Midshaft humeral fracture, "Saturday night palsy" | Cubitus valgus, leaning on elbow |
| Classic deformity | Ape hand | Wrist drop | Claw hand (ring + little fingers) |
| Motor loss | Thenar muscles (LOAF), lateral 2 lumbricals | All extensors of wrist + fingers + thumb, brachioradialis | Hypothenar, medial 2 lumbricals, all interossei, adductor pollicis |
| Sensory loss | Lateral 3½ fingers (palm side) + dorsal tips | Dorsum of lateral 3½ fingers (small area), anatomical snuffbox | Medial 1½ fingers, both palmar and dorsal |
| Key clinical sign | Pope's blessing (can't flex index/middle fingers) | Finger/wrist drop | Froment's sign (flexes thumb IP joint when pinching) |
| Hand weakness | Opposition + abduction of thumb | Extension at wrist and fingers | Grip, pinch, finger abduction/adduction |
| Pen/writing test | Can't oppose thumb to write | Can't extend wrist to write | Weak grip on pen |
The Three Deformities Explained
🤚 Ape Hand (Median nerve)
- Thenar eminence wastes away (flat palm)
- Thumb falls into same plane as fingers (lost opposition)
- Called "ape" because apes cannot oppose their thumb
- Test: ask patient to touch thumb to little finger - cannot do it
🤚 Wrist Drop (Radial nerve)
- Wrist hangs flexed due to loss of all wrist extensors
- Cannot extend wrist, MCP joints, or thumb
- Brachioradialis also lost (elbow flexion weakened in midpronation)
- Test: ask patient to extend wrist against resistance - cannot do it
🤚 Claw Hand (Ulnar nerve)
- Ring and little fingers are clawed (hyperextended at MCP, flexed at IP joints)
- Index and middle fingers are not clawed because their lumbricals are intact (supplied by median nerve)
- This is called the "ulnar paradox" - a lesion at the wrist produces a worse claw than a lesion at the elbow
- Test: Froment's sign - ask patient to grip a paper between thumb and index finger - patient flexes thumb IP joint (uses FPL from median nerve to compensate)
Ulnar Paradox - Exam Favourite
High ulnar nerve lesion (elbow): FDP to ring/little fingers is also paralyzed, so fingers can't flex at IP joints - less clawing Low ulnar nerve lesion (wrist): FDP intact, so fingers CAN flex at IP joints - more clawing The higher the lesion, the less the claw = ulnar paradox
Quick 3-Word Memory
| Nerve | Injury site | Deformity |
|---|---|---|
| Median | Carpal tunnel | Ape hand |
| Radial | Spiral groove | Wrist drop |
| Ulnar | Medial epicondyle | Claw hand |
"Monkey Apes, Radios Drop, Ulcers Claw" - Median=Ape, Radial=Drop, Ulnar=Claw
radial nerve diagram with branches
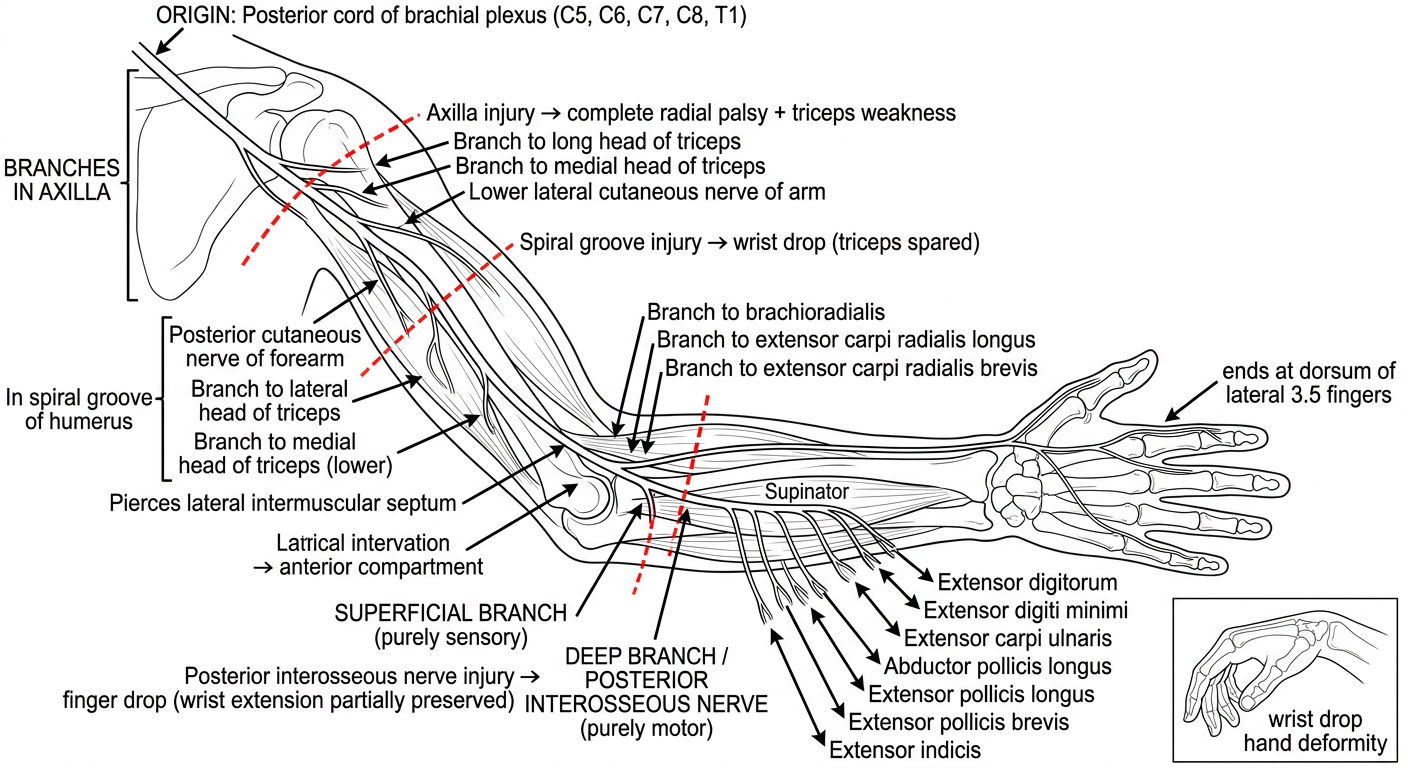
Radial Nerve - Complete Branch Breakdown
Origin
- Posterior cord of brachial plexus
- Spinal levels: C5, C6, C7, C8, T1
Branches in the AXILLA
| Branch | Supplies |
|---|---|
| Nerve to long head of triceps | Triceps (long head) |
| Nerve to medial head of triceps | Triceps (medial head) |
| Posterior cutaneous nerve of arm | Skin of posterior arm |
| Lower lateral cutaneous nerve of arm | Skin of lower lateral arm |
Branches in the SPIRAL GROOVE (arm)
| Branch | Supplies |
|---|---|
| Nerve to lateral head of triceps | Triceps (lateral head) |
| Nerve to medial head of triceps (lower) | Triceps (medial head, lower part) |
| Posterior cutaneous nerve of forearm | Skin of posterior forearm all the way to wrist |
The spiral groove is where the radial nerve winds around the posterior surface of the humerus between the lateral and medial heads of triceps. A midshaft humeral fracture injures it here.
Branches at LATERAL EPICONDYLE / Cubital Fossa
| Branch | Supplies |
|---|---|
| Nerve to brachioradialis | Brachioradialis |
| Nerve to ECRL | Extensor carpi radialis longus |
| Nerve to ECRB | Extensor carpi radialis brevis |
BIFURCATION - The Key Point
Radial Nerve
│
├──→ SUPERFICIAL BRANCH (purely SENSORY)
│ └── Dorsum of lateral 3½ fingers
│ (not the tips - tips by median nerve)
│
└──→ DEEP BRANCH = POSTERIOR INTEROSSEOUS NERVE (purely MOTOR)
└── Winds through supinator muscle
then supplies all remaining extensors
POSTERIOR INTEROSSEOUS NERVE (PIN) Branches
| Muscle | Action |
|---|---|
| Supinator | Supination |
| Extensor digitorum | Extends fingers 2-5 at MCP |
| Extensor digiti minimi | Extends little finger |
| Extensor carpi ulnaris | Extends + adducts wrist |
| Abductor pollicis longus | Abducts thumb |
| Extensor pollicis longus | Extends thumb IP joint |
| Extensor pollicis brevis | Extends thumb MCP joint |
| Extensor indicis | Extends index finger independently |
3 Injury Levels - Exam Favourite
| Level | Site | What is Lost | What is Spared |
|---|---|---|---|
| Axilla | Crutch palsy, axillary dislocation | Everything - triceps, wrist + finger extension, sensation | Nothing |
| Spiral groove | Midshaft humeral fracture | Wrist drop, finger drop, sensation on dorsum | Triceps spared (branches given off above) |
| PIN (below elbow) | Radial tunnel syndrome | Finger drop only | Wrist extension preserved (ECRL given off above bifurcation), no sensory loss |
Key exam MCQ: In spiral groove injury - triceps is spared because its branches arise proximal to the spiral groove. Elbow extension is intact.
PIN injury exam trap: No sensory loss (PIN is purely motor) + wrist drops to ulnar side (ECU lost, ECRL intact pulls wrist to radial side during extension attempt)
One-Line Summary
"Radial nerve = posterior cord → axilla → spiral groove → lateral epicondyle → splits into superficial (sensory) + deep/PIN (motor extensors)"