
Explain please
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a full explanation of the clinical case in that image:
The Answer: Gout (Option C - "Rich Man's Disease")
The image shows swollen, inflamed hand joints in a patient with confirmed hyperuricemia. The diagnosis is Gout - a crystal-induced arthritis caused by the deposition of monosodium urate (MSU) crystals in joints and soft tissues.
Why the Other Options Are Wrong
| Option | Condition | Why it doesn't fit |
|---|---|---|
| A | Rheumatoid Arthritis | Symmetric small joint arthritis, elevated RF/anti-CCP, NOT linked to uric acid |
| B | Osteoarthritis | Degenerative, not inflammatory/hyperuricemic; bony hard swelling (Heberden's nodes) |
| C | Rich Man's Disease (Gout) | Correct - classically linked to hyperuricemia + urate crystal deposition |
| D | Psoriatic Arthritis | Associated with psoriasis skin lesions, not hyperuricemia |
What is Gout? Full Breakdown
Definition & Mechanism
Gout is a chronic disease of monosodium urate (MSU) crystal deposition, presenting as painful and potentially destructive arthritis arising in the setting of hyperuricemia. Urate is the obligatory end-product of human purine metabolism. Unlike most other mammals, humans lack the enzyme uricase, which would normally convert urate to the more soluble compound allantoin - this is why we uniquely develop gout. (Harrison's Principles of Internal Medicine 22E)
The Disease Progression (see diagram below)
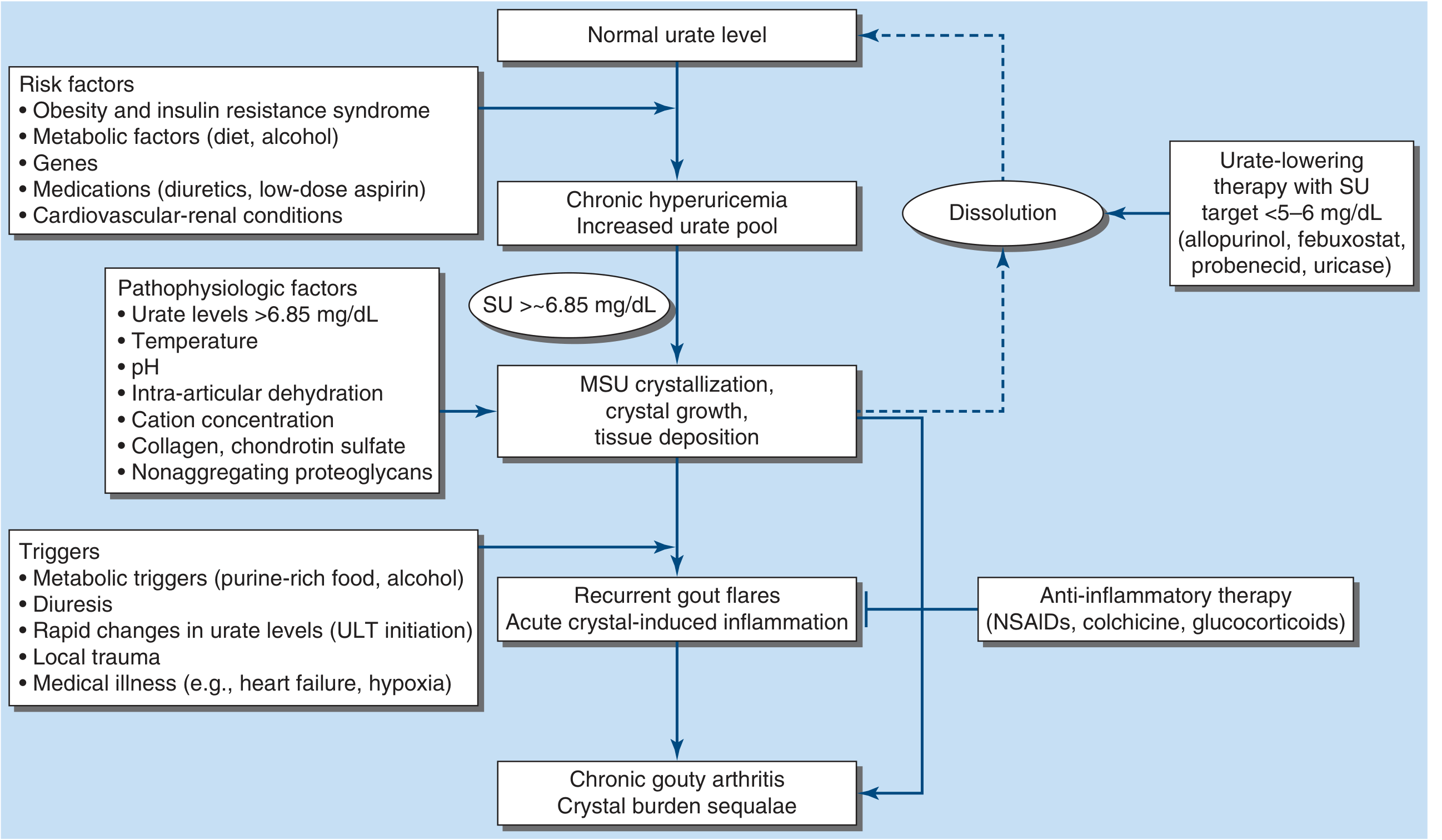
The progression follows this sequence:
- Risk factors (obesity, purine-rich diet, alcohol, diuretics, cardiovascular-renal disease, genetics) lead to...
- Chronic hyperuricemia - serum urate >6.8 mg/dL (>400 μmol/L)
- When serum urate exceeds ~6.85 mg/dL, MSU crystals form, grow, and deposit in joints/tissues
- Acute gout flare - triggered by purine-rich food, alcohol, diuresis, trauma, or illness (e.g., heart failure). Crystals shed from tophi and trigger massive neutrophil recruitment
- Chronic gouty arthritis with tophi if untreated
Why Is It Called "Rich Man's Disease"?
Historically, gout was associated with wealthy individuals who could afford rich foods (red meat, organ meats, shellfish, alcohol - especially beer and wine), all of which are high in purines that break down into uric acid. Kings and aristocrats were commonly afflicted, hence the nickname.
The Inflammatory Mechanism of a Gout Flare
When MSU crystals are shed into the joint cavity:
- Resident synovial cells and phagocytes recognize the crystals
- They secrete chemokines and cytokines, recruiting neutrophils into the joint
- The NLRP3 inflammasome is activated by the crystals, releasing IL-1β - this is the central mediator of the intense pain and swelling
- The flare is self-limiting (days to weeks), regulated by macrophage differentiation and neutrophil extracellular traps (NETs) that degrade pro-inflammatory cytokines
(Rheumatology, 2-Volume Set, Elsevier 2022)
Classic Clinical Features
- Acute gout flare: sudden-onset severe joint pain, swelling, warmth, redness - classically the first MTP joint (big toe = podagra), but also affects ankles, knees, wrists, and fingers (as seen in the image)
- Tophi: chalky white deposits of urate crystals visible under skin - common on ears, elbows, fingers
- Intercritical gout: asymptomatic periods between flares
- Chronic tophaceous gout: persistent joint destruction with tophi visible on imaging
- Lab: elevated serum uric acid, elevated ESR/CRP during flares, negatively birefringent needle-shaped crystals on joint fluid microscopy (gold standard for diagnosis)
Treatment
Acute flare (anti-inflammatory):
- NSAIDs (e.g., indomethacin, naproxen)
- Colchicine (most specific - blocks neutrophil recruitment)
- Glucocorticoids (for those who cannot take NSAIDs/colchicine)
Long-term urate-lowering therapy (ULT) - target serum urate <5-6 mg/dL:
- Allopurinol (xanthine oxidase inhibitor - first line; caution: screen for HLA-B*5801 in Southeast Asian, Pacific Islander, and Black patients before starting - risk of Stevens-Johnson syndrome)
- Febuxostat (another xanthine oxidase inhibitor, useful in CKD or HLA-B*5801 carriers)
- Probenecid (uricosuric - increases renal urate excretion; second-line)
- Pegloticase (pegylated uricase - for refractory cases)
- SGLT2 inhibitors (e.g., empagliflozin) also lower urate and treat common comorbidities
Note: Urate-lowering drugs should NOT be started during an active flare - wait until it resolves, then start ULT with anti-inflammatory prophylaxis (colchicine 0.6 mg daily) for 3-6 months to prevent paradoxical flares.
(Harrison's Principles of Internal Medicine 22E, p. 3000)
Summary: The swollen hands + hyperuricemia hint = Gout. It results from urate crystal deposition in joints, triggering severe inflammation via the NLRP3/IL-1β pathway. Management targets both acute inflammation (colchicine/NSAIDs) and the underlying hyperuricemia (allopurinol/febuxostat).
Tell me abou herpes virus
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have enough rich textbook content to give a thorough answer. Here it is:
The Herpesvirus Family (Herpesviridae)
The name "herpes" comes from the Greek word meaning "to creep" - reflecting how these viruses quietly establish lifelong infections and periodically resurface. Cold sores were described in antiquity; their viral origin was confirmed in 1919. (Medical Microbiology 9e)
Structure - What All Herpesviruses Share
All members of the Herpesviridae family share the same architecture:
- Double-stranded DNA genome (large, ~125,000-230,000 bp)
- Icosahedral nucleocapsid (protein shell surrounding the DNA)
- Tegument layer (proteins between capsid and envelope)
- Lipid envelope studded with glycoproteins
- Total diameter: ~150-200 nm
Because they are enveloped, herpesviruses are fragile outside the body - easily killed by drying, detergents, and heat. This is why transmission requires close direct contact.
The 8 Human Herpesviruses
| Virus | Common Name | Subfamily | Latency Site | Key Disease |
|---|---|---|---|---|
| HHV-1 (HSV-1) | Herpes Simplex 1 | Alpha | Trigeminal ganglion | Cold sores, oral herpes, encephalitis |
| HHV-2 (HSV-2) | Herpes Simplex 2 | Alpha | Sacral ganglion | Genital herpes, neonatal herpes |
| HHV-3 (VZV) | Varicella-Zoster | Alpha | Dorsal root ganglia | Chickenpox (1°), Shingles (reactivation) |
| HHV-4 (EBV) | Epstein-Barr Virus | Gamma | B lymphocytes | Infectious mononucleosis, Burkitt lymphoma, NPC |
| HHV-5 (CMV) | Cytomegalovirus | Beta | Monocytes/macrophages | Congenital CMV, disease in immunocompromised |
| HHV-6 | - | Beta | T lymphocytes | Roseola infantum (exanthem subitum) |
| HHV-7 | - | Beta | T lymphocytes | Roseola (rare) |
| HHV-8 (KSHV) | Kaposi Sarcoma HV | Gamma | B lymphocytes | Kaposi sarcoma (in AIDS patients) |
The Defining Feature: Latency and Reactivation
This is what makes herpesviruses so unique and clinically important. The cycle works like this:
1. Primary Infection
The virus enters through mucous membranes or breaks in the skin, replicates at the entry site, and causes the initial illness (e.g., cold sore, chickenpox).
2. Neuronal Invasion and Latency
The virus travels by retrograde axonal transport to the sensory neuron ganglia:
- HSV-1 → trigeminal ganglia (face/oral region)
- HSV-2 → sacral ganglia (genital region)
- VZV → dorsal root ganglia (any dermatome)
In the neuron, viral DNA persists in the nucleus. Only latency-associated transcripts (LATs) are made - no viral proteins are produced, so the immune system cannot "see" the virus. LATs inhibit cell death (apoptosis) and silence lytic gene expression through epigenetic silencing (heterochromatin formation). (Robbins Pathologic Basis of Disease)
3. Reactivation Triggers
- Physical stress, fever, UV light (sunlight)
- Emotional stress
- Immunosuppression (HIV, chemotherapy, steroids)
- Trauma
- Menstruation
On reactivation, the virus travels back down the axon to the same skin territory (same dermatome/location every time) and causes recurrent disease - usually milder than the primary episode because memory immune responses are already in place. (Medical Microbiology 9e)
Key Viruses in Detail
HSV-1 and HSV-2
- HSV-1 and HSV-2 are genetically very similar (~50% DNA homology) and cause overlapping diseases
- Distinguished by antibodies against glycoprotein G (type-specific)
- HSV genome encodes ~80 proteins - only half needed for replication; the rest help the virus evade immunity
- The virus encodes its own thymidine kinase - this is the key target for acyclovir therapy (see below)
HSV-1 diseases:
- Orolabial herpes (cold sores / fever blisters) - most common
- Herpetic gingivostomatitis - severe primary infection in children
- Herpes keratitis - leading infectious cause of corneal blindness in the US
- Herpes encephalitis - most common cause of fatal sporadic encephalitis; typically affects temporal lobes
- Herpetic whitlow (finger infection), herpes gladiatorum (wrestlers)
HSV-2 diseases:
- Genital herpes (though HSV-1 now accounts for ~50% of new genital cases)
- Neonatal herpes - acquired during delivery through infected birth canal; devastating, can cause encephalitis/disseminated disease
- HSV-2 increases HIV transmission risk 4-fold by causing ulcers and suppressing local immunity
Pathology on biopsy/smear:
- Cowdry type A intranuclear inclusions (large pink-purple inclusion bodies)
- Multinucleated syncytia (giant cells with multiple nuclei) - seen on Tzanck smear
- These histological findings are classic for all herpesviruses
VZV (HHV-3) - Varicella-Zoster Virus
Primary infection = Chickenpox (Varicella)
- Highly contagious - attack rate >90% in seronegative individuals
- Transmission by respiratory droplets (aerosol)
- Diffuse centripetal vesicular rash (starts on trunk, spreads outward) in crops at different stages
- Incubation: 10-21 days
Reactivation = Shingles (Herpes Zoster)
- Virus reactivates in dorsal root ganglia after decades of latency
- Increased risk with age (after 60), immunosuppression
- Presents as dermatomal vesicular rash (painful blisters along a single nerve territory - one side of the body)
- Postherpetic neuralgia - severe, burning nerve pain persisting after the rash heals; can be debilitating
- Zoster can affect cranial nerves: Ramsay Hunt syndrome (facial nerve - ear blisters + facial palsy), herpes zoster ophthalmicus (V1 - risk of blindness) (Harrison's 22E)
Immune Evasion - Why Herpesviruses Are So Persistent
These viruses are masters of immune evasion:
- Block MHC class I presentation - plug the TAP transporter so viral peptides can't be presented to CD8 T cells
- Express Fc receptors (gE/gI) - bind the constant part of antibodies to block antibody-dependent killing
- Express complement receptors (gC) - bind C3 to accelerate complement decay
- Spread cell-to-cell directly - bypass circulating antibodies
- Hide in neurons - no viral proteins during latency means nothing for the immune system to target (Medical Microbiology 9e)
CD8 T cells and interferon-gamma (IFN-γ) are critical for maintaining latency.
Treatment
The cornerstone of antiviral therapy is targeting the virus's own thymidine kinase (TK):
| Drug | Mechanism | Uses |
|---|---|---|
| Acyclovir | Acyclovir is phosphorylated by viral TK (not cellular TK) → gets trapped in infected cells → inhibits viral DNA polymerase | HSV-1, HSV-2, VZV |
| Valacyclovir | Oral prodrug of acyclovir with better bioavailability | Same as acyclovir - more convenient |
| Famciclovir | Prodrug of penciclovir | HSV, VZV |
| Ganciclovir | CMV (uses different kinase - UL97) | CMV retinitis, CMV in immunocompromised |
| Foscarnet | Direct viral DNA polymerase inhibitor (no TK needed) | Acyclovir-resistant HSV/VZV |
Key principle: Treating the initial herpes episode does NOT reduce future recurrences - because the virus establishes latency within hours of infection, days before symptoms even appear. (Fitzpatrick's Dermatology)
For suppressive therapy (to reduce recurrence frequency): acyclovir 400 mg twice daily or valacyclovir 500 mg once daily long-term.
Herpes and Cancer
Two herpesviruses are directly oncogenic:
- EBV (HHV-4): Burkitt lymphoma, Hodgkin lymphoma, nasopharyngeal carcinoma, gastric cancer
- HHV-8 (KSHV): Kaposi sarcoma (especially in AIDS patients), primary effusion lymphoma
Quick Summary
Herpesviruses are enveloped dsDNA viruses that uniquely establish lifelong latency in neurons or lymphocytes and reactivate when immunity dips. There are 8 human members causing diseases from cold sores to cancer. Their thymidine kinase makes them selectively targetable by drugs like acyclovir. The immune system normally keeps them suppressed - which is why immunocompromised patients (HIV, transplant recipients, chemotherapy) suffer the most severe herpesvirus disease.
Hsv1
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Here is a focused, detailed breakdown of HSV-1:
Herpes Simplex Virus Type 1 (HSV-1)
Classification and Basic Facts
- Family: Herpesviridae, subfamily Alphaherpesvirinae
- Large double-stranded DNA virus with ~80 encoded proteins
- Enveloped - killed easily by drying, detergents, soap
- Exclusively a human pathogen; worldwide distribution, no seasonality
-
700,000 new HSV-1 infections per year in the US alone
- Most people are infected in childhood - most infections are subclinical (Medical Microbiology 9e)
Structure and Key Proteins
The HSV-1 genome encodes:
- DNA polymerase (viral-specific - targeted by antivirals)
- Thymidine kinase (TK) - phosphorylates nucleosides to provide substrates for replication; this is the key target for acyclovir
- Ribonucleotide reductase - converts ribonucleotides to deoxyribonucleotides
- At least 10 glycoproteins on the envelope surface:
- gB, gC, gD - attachment and entry into host cells
- gB, gH/gL - membrane fusion
- gC, gE, gI - immune escape (complement evasion, antibody Fc binding)
HSV-1 enters cells by first binding heparan sulfate on the cell surface, then locking onto nectin-1 (an adhesion molecule found on most cells and neurons) to trigger membrane fusion and inject its capsid into the cytoplasm. (Medical Microbiology 9e)
Transmission
- Primary route: oral contact - kissing, sharing utensils, toothbrushes, cups
- Direct inoculation into cuts or abraded skin
- Autoinoculation - touching an active sore then touching the eye or fingers
- HSV-1 now accounts for ~50% of new genital herpes cases (from oral sex)
- HSV-1 can infect healthcare workers through oral secretions → herpetic whitlow (finger infection); dentists and nurses are particularly at risk
- Asymptomatic viral shedding makes the infected person a lifelong source of contagion (Medical Microbiology 9e)
Pathogenesis - The Full Cycle
Step 1: Primary Infection
HSV-1 enters through oral mucosa or skin abrasions. It replicates in epithelial cells and fibroblasts at the entry site, producing the classic vesicular lesion: a clear blister on a red base ("dewdrop on a rose petal"), which progresses to pustules → ulcers → crusted lesions.
Step 2: Neuroinvasion
The virus travels by retrograde axonal transport from the oral/facial mucosa up to the trigeminal ganglion, where it establishes lifelong latency.
Step 3: Latency
Inside the neuron:
- Viral DNA sits in the nucleus but does not replicate
- Only latency-associated transcripts (LATs) are made - no viral proteins are produced
- LATs block apoptosis, silence lytic genes via heterochromatin formation, and encode microRNAs that suppress lytic gene expression
- The immune system cannot detect the virus → true latency
Step 4: Reactivation
Triggers include: fever, UV light (sunlight), emotional stress, trauma, immunosuppression, menstruation
On reactivation, the virus travels back down the trigeminal nerve to the same site (usually the lips/perioral region) and causes recurrent disease. Recurrences are generally milder because memory T cells and antibodies are already present. (Robbins & Cotran Pathologic Basis of Disease)
Clinical Diseases - All Caused by HSV-1
1. Orolabial Herpes (Cold Sores / Fever Blisters)
- Most common manifestation
- Vesicles appear at the vermillion border of the lips or perioral skin
- Prodrome of tingling/burning for 1-2 days before blisters appear
- Self-limited in immunocompetent: heals in 7-10 days
- Same location recurs every time (reactivation from trigeminal ganglion)
2. Primary Herpetic Gingivostomatitis
- Severe primary infection in young children
- Widespread painful vesicles and ulcers throughout the mouth (palate, gums, buccal mucosa, tongue), high fever, drooling, lymphadenopathy
- More extensive than a recurrence; can prevent eating/drinking
- Resolves in 2-3 weeks
3. Herpes Keratitis (Eye)
- HSV-1 is the most common infectious cause of corneal blindness in developed countries
- Up to 60% of corneal ulcers in developing countries are due to HSV
- ~10 million people worldwide have herpetic eye disease
- About 10% of those with any history of herpes simplex keratitis (HSK) eventually reach visual acuity <6/60 (legal blindness)
- Presents as: dendritic corneal ulcer (branching ulcer visible with fluorescein staining) - pathognomonic
- Repeated episodes → corneal scarring → permanent visual loss (Kanski's Clinical Ophthalmology)
4. Herpes Encephalitis
- Most serious complication
- Most common cause of fatal sporadic encephalitis in the US - ~1-2 cases per 500,000 per year
- >90% of adult cases are caused by HSV-1
- The virus reaches the brain via the trigeminal tracts or olfactory nerves → hemorrhagic necrosis of the temporal lobe (and orbital frontal gyri)
- Classic symptoms: fever + headache + altered consciousness + behavioral changes + aphasia + seizures (temporal lobe signs)
- MRI: T2 signal abnormality in the temporal lobe (unilateral early, can spread bilateral)
- CSF: lymphocytic pleocytosis, mildly elevated protein, normal glucose; PCR for HSV DNA in CSF is the gold-standard diagnostic test
- Without treatment: mortality >70%, <10% return to normal
- With IV acyclovir (10 mg/kg q8h for 14-21 days): mortality drops to 10-25%, ~40-55% can resume daily activities (Goldman-Cecil Medicine)
5. Herpetic Whitlow
- HSV-1 infection of the finger/hand via inoculation through a cut
- Common in dentists, nurses, physicians - anyone with unprotected exposure to oral secretions
- Painful vesicles on the finger, often with red streak (lymphangitis)
6. Herpes Gladiatorum
- Cutaneous HSV-1 in wrestlers/contact sport athletes from direct skin-to-skin contact
7. Eczema Herpeticum
- Widespread, potentially life-threatening HSV spread across the skin of patients with atopic dermatitis (eczema)
- The disrupted skin barrier allows massive viral spread
8. Neonatal Herpes (HSV-1 or HSV-2)
- Usually HSV-2 (70%), but HSV-1 accounts for ~30% of cases
- Acquired during vaginal delivery through an infected birth canal
- Three forms: skin-eye-mouth (SEM), CNS disease, disseminated disease
- C-section is recommended for mothers with active genital HSV lesions at delivery
- Treatment: IV acyclovir (Medical Microbiology 9e)
Diagnosis
| Method | Details |
|---|---|
| PCR (gold standard) | HSV DNA detection in CSF, vesicle fluid, swabs - most sensitive and specific |
| Viral culture | From vesicle fluid/swabs - slower (2-5 days), used for genotyping |
| Tzanck smear | Scraping from base of vesicle - shows multinucleated giant cells (Cowdry type A inclusions) - fast but NOT type-specific |
| Serology (IgG) | Type-specific antibodies against glycoprotein G - useful to confirm past exposure, not acute diagnosis |
| Biopsy | Eosinophilic intranuclear inclusions + multinucleated syncytia |
Treatment
| Indication | Drug and Dose |
|---|---|
| Orolabial herpes (episodic) | Acyclovir 400 mg 3x/day OR valacyclovir 2g twice a day for 1 day (high-dose short course) |
| Genital herpes (episodic) | Acyclovir 400 mg 3x/day x 5 days OR valacyclovir 500 mg twice daily x 3 days |
| Suppressive therapy | Acyclovir 400 mg twice daily OR valacyclovir 500-1000 mg once daily (long-term) |
| Herpes keratitis | Topical acyclovir ointment; topical antivirals (trifluridine); avoid steroids alone |
| Herpes encephalitis | IV acyclovir 10 mg/kg q8h x 14-21 days |
| Neonatal herpes | IV acyclovir 60 mg/kg/day x 14-21 days |
| Acyclovir-resistant HSV | Foscarnet (bypasses thymidine kinase) |
How acyclovir works: Acyclovir is selectively phosphorylated by the viral thymidine kinase (not human TK) in infected cells. This traps the active form inside infected cells. The activated drug then inhibits the viral DNA polymerase, chain-terminating viral DNA replication. Because normal cells lack viral TK, acyclovir has very low toxicity to the host.
Key point: Treating a herpes episode does NOT prevent future recurrences - because the virus enters latency within hours of infection, long before symptoms even appear. (Fitzpatrick's Dermatology)
Summary
HSV-1 is an Alpha-herpesvirus with worldwide prevalence, acquired mostly in childhood via oral contact. It establishes lifelong latency in the trigeminal ganglion and reactivates to cause cold sores, keratitis, and encephalitis. Clinically, the most dangerous manifestations are encephalitis (temporal lobe destruction - treat immediately with IV acyclovir) and corneal blindness (from recurrent keratitis). Acyclovir and its prodrugs are safe and effective, exploiting the virus's own thymidine kinase for selective activation.
This is a shared conversation. Sign in to Orris to start your own chat.