How to put rules tube aspiration
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent! I now have all the information needed for a complete, well-illustrated answer. Here is the full guide:
Ryle's Tube (Nasogastric Tube) Insertion and Aspiration
A Ryle's tube is a non-vented, single-lumen nasogastric (NG) tube used primarily for gastric decompression and aspiration. It is named after Dr. John Alfred Ryle. The vented equivalent is the Salem sump tube (double-lumen). Both pass through the nose into the stomach.
Indications
- Gastric decompression (bowel obstruction, ileus)
- Prevention of aspiration before/after surgery
- Monitoring and evaluation of upper GI bleeding
- Administration of medications or feeds when the patient cannot swallow
- Gastric lavage in poisoning
Contraindications
- Midface injury or basilar skull fracture (use orogastric route instead)
- Severe coagulopathy (relative)
- History of gastric bypass or lap banding
- Esophageal strictures or alkali injury
Equipment Needed
- Ryle's tube (appropriate size - 14-18 Fr for adults)
- Topical vasoconstrictor (phenylephrine 0.5% or oxymetazoline 0.05% spray)
- Topical anesthetic (2% lidocaine gel or nebulized 4-10% lidocaine)
- Lubricant (viscous lidocaine 2% or water-soluble gel)
- Cup of water with a straw
- Catheter-tipped syringe (20-60 mL)
- Tape for securing
- pH paper or stethoscope for confirmation
- Gloves, gown, kidney dish
Step-by-Step Procedure
1. Patient Preparation
- Sit the patient upright at 45-90 degrees (semi-Fowler's or fully upright if possible)
- Explain the procedure to the patient
- Check for and remove dentures if present
- Place a kidney dish and tissue near the patient
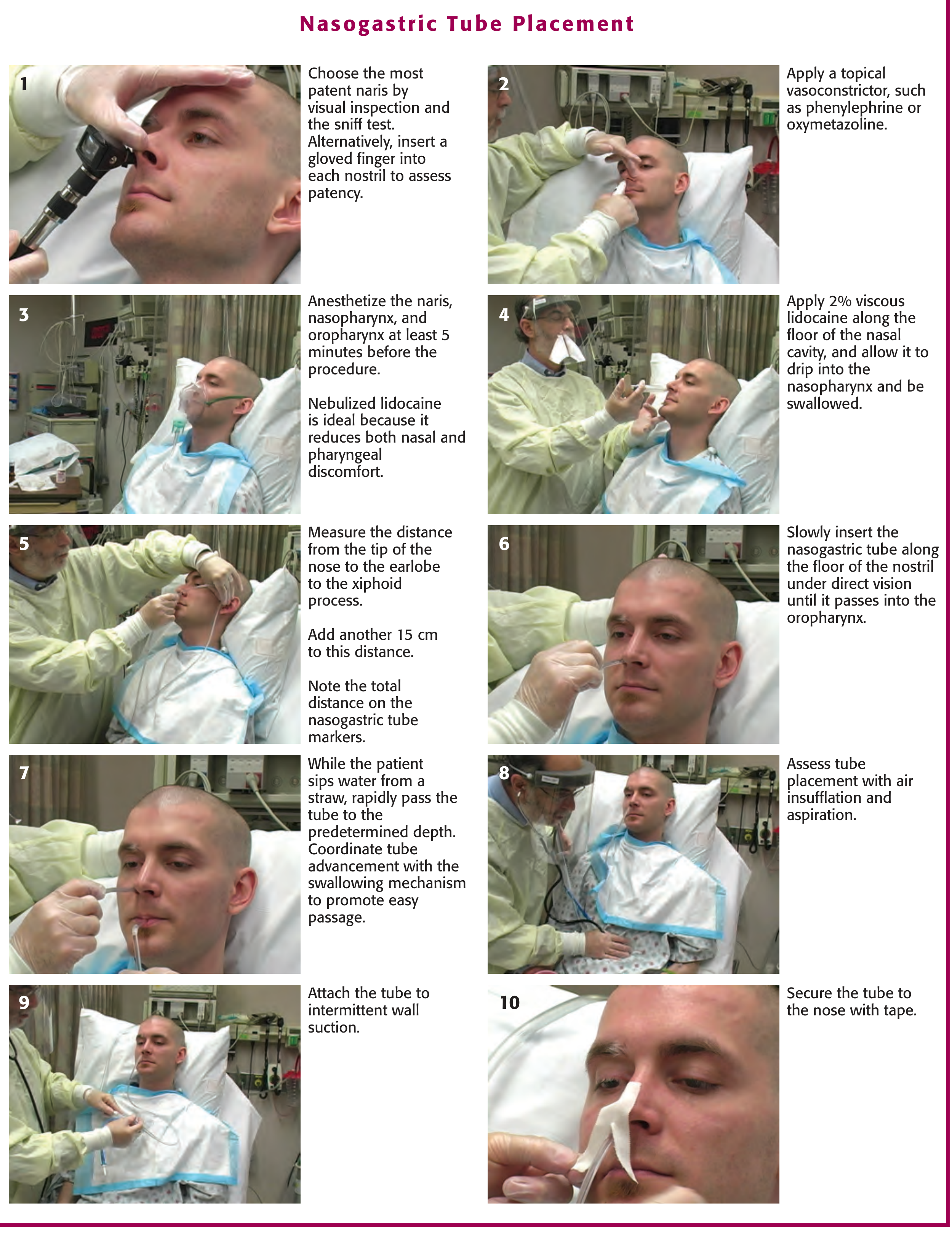
2. Choose the Nostril (Step 1)
- Inspect both nostrils and ask the patient to sniff through each
- Choose the most patent naris - insert a gloved finger gently to assess patency
- Avoid any nostril with recent trauma or nasal polyps
3. Apply Vasoconstrictor (Step 2)
- Spray a topical vasoconstrictor (phenylephrine 0.5% or oxymetazoline) into both nares
- This reduces nasal mucosal congestion and minimizes bleeding
4. Anesthetize (Step 3 & 4)
- Anesthetize the naris, nasopharynx, and oropharynx at least 5 minutes before proceeding
- Nebulized lidocaine (4 mL of 10% solution) is the most effective method - reduces both nasal and pharyngeal discomfort
- Apply 2% viscous lidocaine along the floor of the nasal cavity and allow it to drip into the nasopharynx to be swallowed
5. Measure the Insertion Depth (Step 5)
- Measure from the tip of the nose → earlobe → xiphoid process
- Add an additional 15 cm to this distance
- Mark this total depth on the tube (Ryle's tubes have depth markings)
6. Lubricate the Tube
- Coat the first 15-20 cm of the tube liberally with 2% lidocaine gel or water-soluble lubricant
- Do not rely only on the lubricant for anesthesia - it must be pre-applied to the mucosa first
7. Insert the Tube (Step 6 & 7)
- With the patient's head in neutral or slightly flexed position, slowly insert the tube along the floor of the nostril (aim horizontally backward toward the ear, NOT upward)
- Pass it gently into the oropharynx under direct vision
- Once it reaches the oropharynx (~15 cm), ask the patient to sip water through a straw and swallow repeatedly
- Rapidly advance the tube to the predetermined depth while the patient is swallowing - this coordinates tube advancement with the swallowing mechanism
Key tip: If resistance is met, withdraw slightly, rotate the tube, and retry. If the patient coughs, chokes, or cannot speak - stop immediately and withdraw as the tube may be in the airway.
8. Confirm Placement (Step 8)
Use more than one method:
| Method | Detail |
|---|---|
| Air insufflation + auscultation | Inject 10-20 mL of air rapidly via syringe; auscultate over the epigastrium for a whooshing sound. Quick but not fully reliable |
| Aspiration + pH testing | Aspirate gastric contents; pH <4 = ~95% chance of correct gastric placement. More reliable |
| Patient speech | Ask the patient to speak - inability to speak suggests tracheal placement |
| Chest X-ray | Gold standard, especially in unconscious/obtunded patients. Tube should be seen passing below the diaphragm, tip at or below the gastroesophageal junction |
| Ultrasound | Highly reliable when successful |
9. Attach to Suction (Step 9)
- Connect the tube to intermittent wall suction (or leave on free drainage)
- For a Ryle's tube used for gastric aspiration: place on free drainage with 4-hourly aspiration or connect to continuous/intermittent suction as clinically needed
10. Secure the Tube (Step 10)
- Clean the nose and tube with tincture of benzoin (if available)
- Tape the tube to the nose using a butterfly/split-tape technique - ensure no pressure on the nostril margins to prevent necrosis
- Also secure the tube to the patient's gown to prevent accidental traction on the nose
Ongoing Aspiration Management
- For decompression (e.g., bowel obstruction): place on free drainage with 4-hourly aspiration or continuous suction
- Record the volume, color, and character of aspirate each time
- For the Salem sump tube: keep the blue pigtail (air vent) above the level of stomach fluid at all times to prevent siphoning
Confirming and Monitoring
- Inspect the aspirate: gastric contents are typically pale/yellow; bilious if the tube is past the pylorus; frank blood if upper GI bleeding
- Re-confirm position by X-ray if the patient's condition changes or placement is uncertain
- Replace the nose tape and reapply benzoin if the tape loosens
Complications to Watch For
| Complication | Watch for |
|---|---|
| Pulmonary misplacement | Coughing, cyanosis, inability to speak |
| Intracranial placement | Only in head trauma with basilar skull fracture |
| Epistaxis | Common - minimize with vasoconstrictor and gentle technique |
| Sinusitis | With prolonged tube placement |
| Aspiration pneumonia | If tube is misplaced or patient vomits around tube |
| Nasal necrosis | From poorly secured, tight-fitting tube |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 40 - Nasogastric Tube Placement (pp. 961-965)
- Current Surgical Therapy, 14th Edition - Nasogastric Tube chapter (p. 162)
- Bailey and Love's Short Practice of Surgery, 28th Edition - Supportive Management / Ryle's tube for bowel decompression (p. 1407)
This is a shared conversation. Sign in to Orris to start your own chat.