Avn of femoral head ,scaphoid and lunate bone
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive, textbook-based overview of AVN of the femoral head, scaphoid, and lunate.
Avascular Necrosis (AVN / Osteonecrosis) - Three Classic Sites
1. AVN of the Femoral Head
Why It Happens
The femoral head receives blood primarily via the medial circumflex femoral artery, whose branches run along the femoral neck. Any disruption - through fracture, sustained pressure, or systemic disease - cuts off this supply, leading to bone death, collapse, and eventual secondary osteoarthritis.
Aetiology
Primary (Idiopathic) - includes Perthes disease in children
Secondary causes (Bailey & Love, 28th ed):
| Category | Examples |
|---|---|
| Drugs | Corticosteroids (most common non-traumatic cause) |
| Toxins | Alcohol excess |
| Haematological | Sickle cell disease, other haemoglobinopathies |
| Metabolic | Hyperlipidaemia, Gaucher's disease, chronic liver disease |
| Vascular | Hypercoagulable states (protein C/S deficiency), antiphospholipid antibody syndrome |
| Systemic | SLE, HIV |
| Physical | Caisson disease ("the bends" - in divers), radiotherapy, chemotherapy |
Clinical Features
- Predominantly affects men aged 35-45; bilateral in >50% of patients
- Early stages: often asymptomatic - requiring high index of suspicion
- Progression: groin ache, limp, positive Thomas test, restricted range of motion
Imaging
X-ray (AP pelvis + lateral): Increased sclerosis early; crescent sign (subchondral resorption); late flattening and irregular femoral head
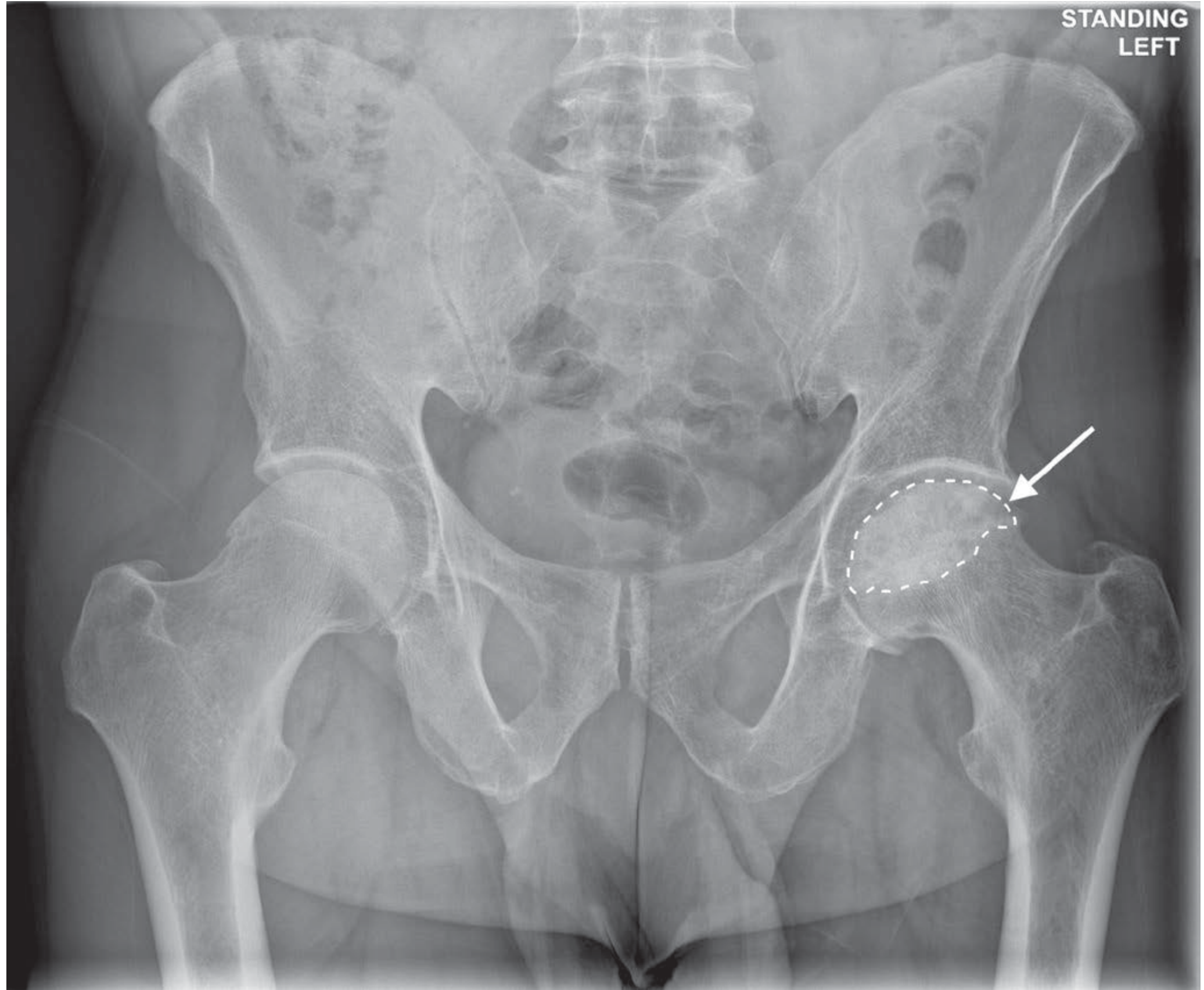
MRI is the most sensitive and specific modality - detects bone marrow changes before X-ray changes appear. Used to assess extent of femoral head involvement and guide prognosis.
Staging - Steinberg Classification (1995)
| Stage | Finding |
|---|---|
| 0 | Normal or non-diagnostic on X-ray, bone scan, and MRI |
| I | Normal X-ray, abnormal MRI or bone scan |
| II | Sclerosis and cysts |
| III | Subchondral collapse - crescent sign |
| IV | Flattening of head, normal acetabulum |
| V | Acetabular involvement |
| VI | Obliteration of joint space |
(Stages I-IV are subdivided A/B/C for mild/moderate/severe involvement)
The older Ficat classification (1985) used 5 stages (0-IV) based on radiographs alone.
Management
Conservative treatment gives poor outcomes in established disease.
| Stage | Approach |
|---|---|
| Pre-collapse (0-III) | Core decompression ± bone grafting, vascularised bone graft, bone marrow-derived cell therapy |
| Post-collapse (IV-VI) | Femoral osteotomy (to bring undamaged surface into weight-bearing zone), or total hip replacement if degenerative changes are present |
2. AVN of the Scaphoid (Proximal Pole)
Why It Happens - Key Anatomy
The scaphoid has a retrograde blood supply: the radial artery enters distally through the scaphoid tuberosity and travels proximally through the bone. This means the proximal pole has no direct arterial entry point. When a fracture crosses the waist of the scaphoid:
- The distal fragment retains its blood supply
- The proximal pole is entirely dependent on the already-tenuous intraosseous flow, which the fracture disrupts
In approximately 10% of individuals, the scaphoid has a sole blood supply from the radial artery, making these people most susceptible. More proximal fractures carry a higher incidence of AVN and nonunion than waist or distal fractures (Rosen's Emergency Medicine; Gray's Anatomy for Students).
Clinical Relevance
- Most common carpal fracture; classically from a fall on an outstretched hand (FOOSH)
- Tenderness in the anatomical snuffbox after trauma = scaphoid fracture until proven otherwise
- Displaced fractures and fractures left untreated are at highest risk for AVN
- AVN leads to chronic wrist pain and radiocarpal arthritis
Imaging
- Initial plain films may be normal - a negative X-ray does not exclude fracture
- MRI is the investigation of choice for early detection
- CT useful to delineate fracture pattern and displacement
Management
- Undisplaced fractures: thumb spica cast
- Displaced or proximal pole fractures: urgent orthopaedic referral, surgical fixation (headless compression screw)
- Established AVN with nonunion: vascularised bone grafting, proximal row carpectomy, or wrist arthrodesis
3. AVN of the Lunate - Kienböck's Disease
Why It Happens - Key Anatomy
Gelberman et al. described three patterns of vessels entering the lunate:
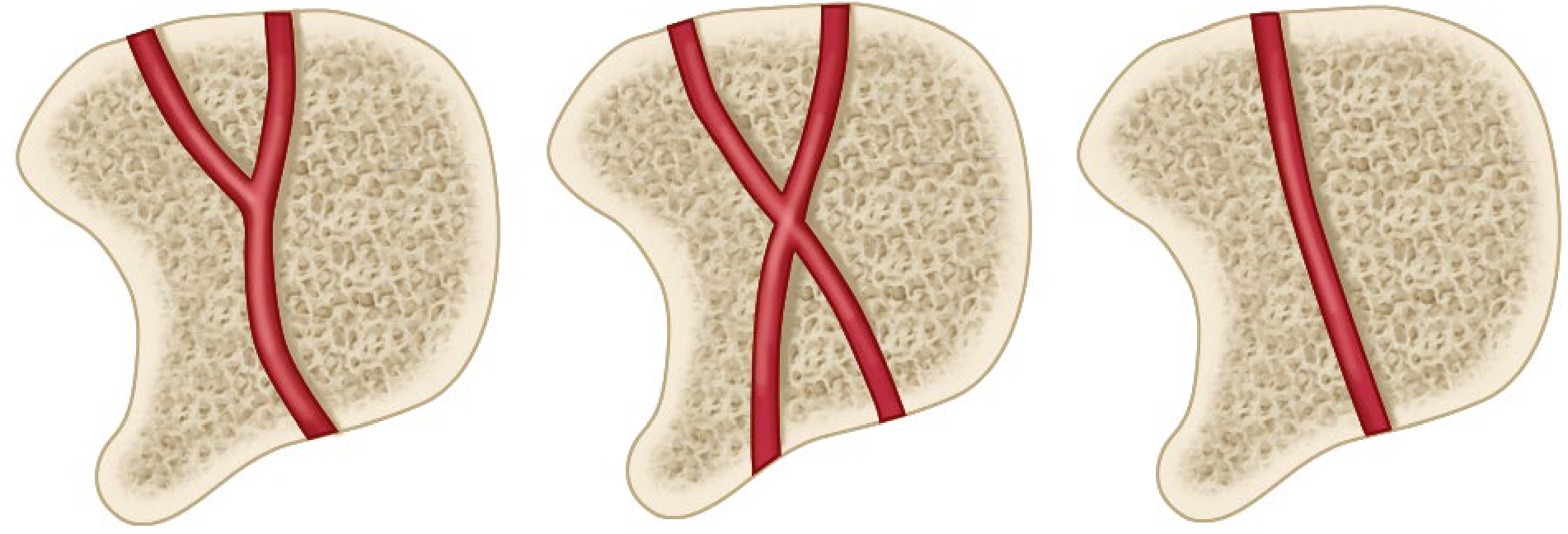
Lunates with a single arterial supply or one surface exposed to blood supply (~20%) are most vulnerable. Additional contributing factors (Miller's Review of Orthopaedics, 9th ed):
- Negative ulnar variance - the ulna is shorter than the radius, transmitting excess shear stress through the lunate
- Increased intraosseous pressure from venous stasis
- Decreased radial inclination
- Trauma (repetitive microtrauma or acute fracture)
Clinical Features
- Men aged 20-40 years, dominant wrist, manual labourers
- Dorsal wrist pain, mild swelling, limited motion, weakness
- Symptoms can precede radiographic changes by up to 18 months
- Rarely bilateral
Imaging
- Early: plain X-ray may be normal or show only a linear fracture
- Progressive: lunate sclerosis then collapse with proximal migration of the capitate
- MRI (investigation of choice for early disease): diffuse low signal on T1, high signal on T2 if revascularisation is occurring
- Negative ulnar variance on neutral PA X-ray is a supportive finding

Lichtman Classification
| Stage | Findings |
|---|---|
| I | Normal X-ray or linear fracture; bone scan/MRI abnormal |
| II | Lunate sclerosis; possible early collapse at radial border |
| IIIA | Lunate collapse, normal carpal alignment |
| IIIB | Lunate collapse, fixed scaphoid rotation (radioscaphoid angle >60°) |
| IV | Arthritic changes throughout the proximal carpal row |
Management (Based on Lichtman Stage + Ulnar Variance)
| Stage | Goal | Options |
|---|---|---|
| I | Salvage the lunate | Cast immobilisation (limited long-term success) |
| II-IIIA | Revascularise the lunate | Joint-levelling procedure (radial shortening osteotomy preferred if ulnar-negative; goal = neutral or +1 mm); vascularised bone graft |
| IIIB-IV | Salvage (lunate cannot be revascularised) | Proximal row carpectomy, intercarpal fusion, excision ± prosthetic replacement, wrist arthrodesis |
Comparison at a Glance
| Feature | Femoral Head AVN | Scaphoid Proximal Pole AVN | Lunate AVN (Kienböck) |
|---|---|---|---|
| Main cause | Steroids, alcohol, fracture | Scaphoid waist/proximal fracture | Idiopathic + negative ulnar variance |
| Blood supply issue | Disruption of medial circumflex femoral artery | Retrograde supply cut off at fracture | Single vessel entry (20% of people) |
| Demographics | Men 35-45 yrs | Young adults post-trauma | Men 20-40 yrs, manual labour |
| Early investigation | MRI | MRI | MRI (T1 low signal) |
| Key X-ray sign | Crescent sign, sclerosis | Sclerosis, nonunion | Lunate sclerosis, carpal collapse |
| Staging system | Steinberg (0-VI) | No standard staging | Lichtman (I-IV) |
| Pre-collapse surgery | Core decompression, vascularised graft | Headless screw fixation | Joint-levelling osteotomy |
| End-stage surgery | Total hip replacement | Wrist fusion / proximal row carpectomy | Wrist arthrodesis |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed; Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Rosen's Emergency Medicine; Gray's Anatomy for Students
Give details all this with talus
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - comprehensive textbook data gathered. Now I'll compile the full answer, adding the talus to the previous three bones as a complete comparison.
AVN of the Talus - Full Details (+ Complete 4-Bone Comparison)
4. AVN of the Talus (Talar Body)
Why the Talus Is Uniquely Vulnerable
The talus is one of the most AVN-prone bones in the body because of a combination of features:
- About 60-70% of its surface is covered by articular cartilage, leaving very few areas where blood vessels can enter
- It has no muscular attachments - tendons and muscles do not pass over it, so there is no periosteal blood supply from soft tissue
- Blood must enter through a small number of specific entry points, making it highly sensitive to disruption
Blood Supply to the Talar Body
The vascular supply (described by Mulfinger and Trueta, 1970) comes from four main sources (Campbell's Operative Orthopaedics, 15th Ed):
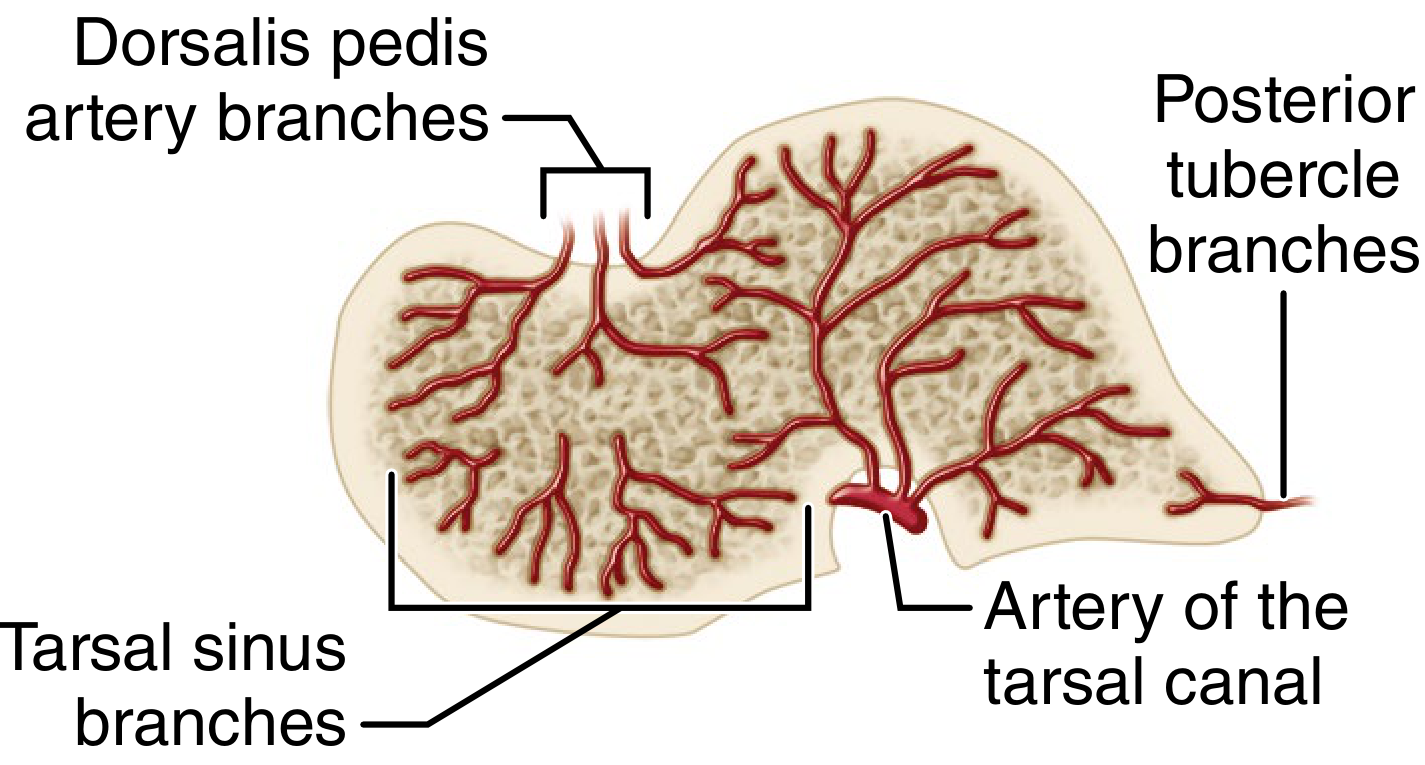
| Vessel | Origin | Territory |
|---|---|---|
| Artery of the tarsal canal (dominant) | Posterior tibial artery, ~1 cm proximal to its bifurcation | Sends 4-6 direct vessels into the talar body - supplies majority of the body |
| Deltoid artery | Branch of the artery of the tarsal canal | Medial 1/4 to 1/2 of talar body; has potential to supply more via intraosseous anastomoses |
| Artery of the sinus tarsi | Perforating peroneal artery / dorsalis pedis / anastomosis between them (variable) | Lateral 1/8 to 1/4 of talar body; anastomoses with tarsal canal artery |
| Posterior tubercle branches | Posterior tibial or peroneal artery | Posterior tubercle; supplies more via intraosseous anastomoses |
Key principle: A displaced fracture of the talar neck severs the artery of the tarsal canal and deltoid artery, cutting off the dominant blood supply to the body. The more displaced the fracture, the more vessels are disrupted, and the higher the AVN risk.
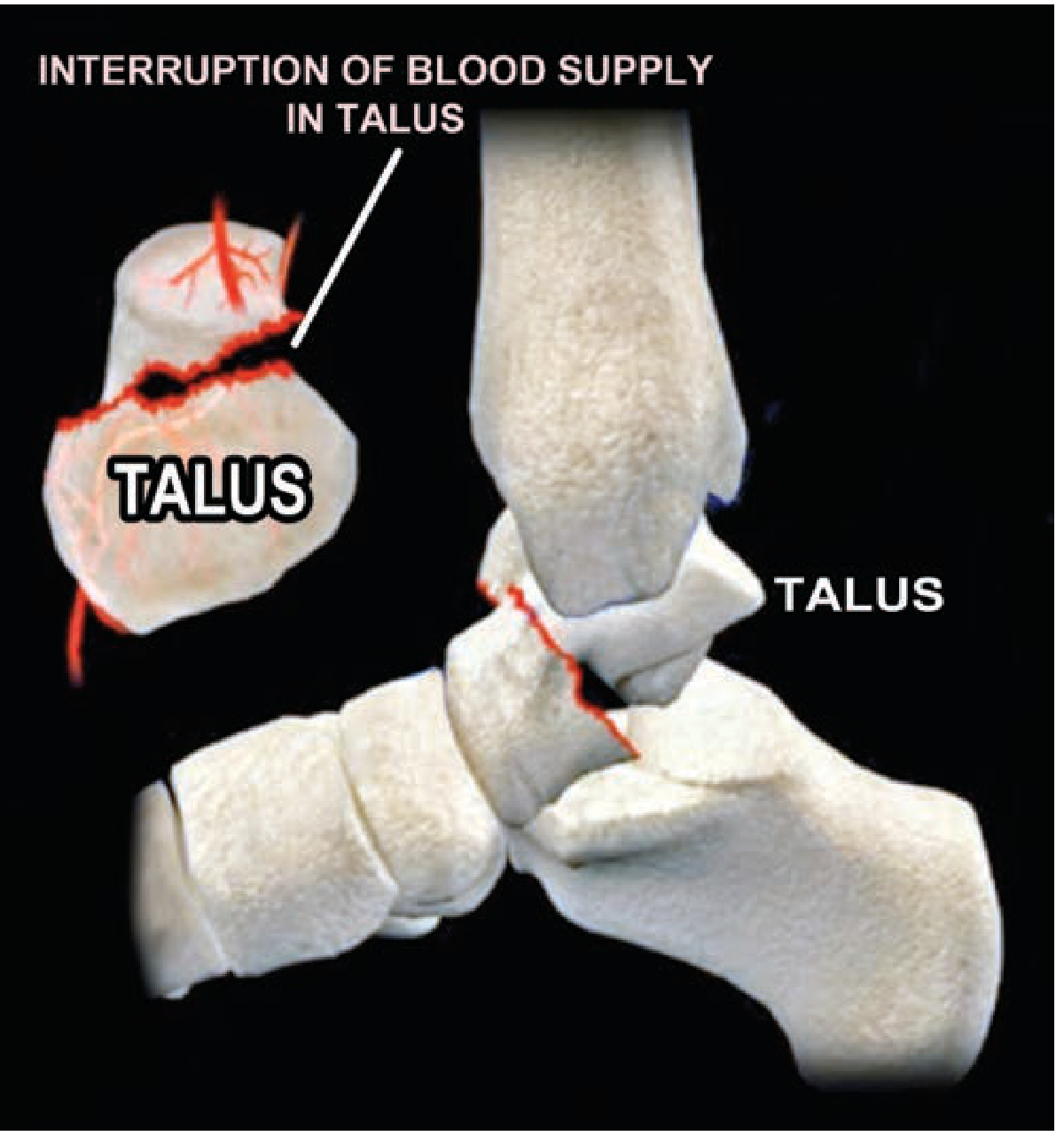
Mechanism / Aetiology
- The classic mechanism is forced dorsiflexion - the talar neck impacts against the anterior distal tibia (historically called "aviator's astragalus" from WW1/WW2 crash injuries)
- Degree of displacement is the single most important predictor of AVN
- High-energy trauma (MVA, falls from height) is the usual cause
Clinical Features
- Severe ankle pain and swelling following high-energy trauma
- Inability to bear weight
- In open dislocations (Type III/IV), the talar body may be visible extruded through the skin
- Late presentation: ankle/subtalar stiffness, chronic pain, collapse of the talar dome
Hawkins Classification of Talar Neck Fractures (most widely used; prognostic for AVN)
| Type | Description | AVN Risk |
|---|---|---|
| I | Nondisplaced talar neck fracture; only vessel entering through neck may be damaged | 0-15% |
| II | Subtalar joint subluxed/dislocated; at least 2 blood supply sources disrupted (neck vessels + tarsal canal/sinus tarsi) | 42-50% |
| III | Talar body dislocated from both tibia AND calcaneus; all 3 blood supply sources potentially disrupted | 91-100% |
| IV | Type III + dislocation of talar head from talonavicular joint | Near 100% |
(Type IV added by Canale & Kelly, Campbell's)
Hawkins' original series (1970): nondisplaced fractures - 0% AVN, all united; Type II - 42% AVN; Type III - 91% AVN and 75% fair/poor results. Presence of AVN correlated with fair/poor results in 88%.
Key Diagnostic Sign - Hawkins Sign
The Hawkins sign is a subchondral lucency (radiolucent line) seen on the mortise X-ray at 6-8 weeks after fracture. It indicates disuse osteopenia of the subchondral bone, which only occurs when there is an intact blood supply enabling bone resorption.
- Hawkins sign PRESENT = vascularity intact = AVN unlikely
- Hawkins sign ABSENT at 3 months = AVN likely - confirmed by MRI or bone scan
This is one of the most clinically important signs in foot and ankle trauma.
Investigations
| Modality | Findings |
|---|---|
| X-ray | Initial - may show fracture displacement; at 6-8 weeks check for Hawkins sign; late - sclerosis and collapse of talar dome |
| MRI | Gold standard for early AVN - decreased signal on T1, variable T2 signal |
| Bone scan | Decreased uptake in affected talar body (early); increased uptake with revascularisation |
| CT | Best for defining fracture pattern and displacement pre-operatively |
Management
| Type | Treatment | Rationale |
|---|---|---|
| Type I | Short leg cast, non-weight-bearing x 6-8 weeks | Low AVN risk; stable |
| Type II | ORIF (cannulated screws or small plates) via anteromedial/dual approach | Restore anatomy, reduce further vascular disruption |
| Type III/IV | Urgent ORIF (orthopaedic emergency) - reduce dislocation ASAP; screw fixation | Every hour of dislocation increases ischaemia and AVN risk; also risk of skin necrosis |
Post-operative:
- Early motion at ~2 weeks if fixation is secure
- Minimum 6 weeks non-weight-bearing
- Avoid varus malunion (reduces subtalar ROM and causes internal rotation gait)
If AVN develops:
- Protected weight-bearing with orthosis (some tali revascularise spontaneously, especially in children)
- Tibiotalar or tibiotalocalcaneal arthrodesis for established collapse
- Total ankle replacement in select cases
Complete 4-Bone AVN Comparison Table
| Feature | Femoral Head | Scaphoid (Proximal Pole) | Lunate (Kienböck) | Talus (Body) |
|---|---|---|---|---|
| Why vulnerable | Medial circumflex femoral a. runs along neck; easily disrupted | Retrograde blood supply - enters distally only | Single-vessel entry in 20%; negative ulnar variance increases stress | 60-70% cartilage surface; no muscle attachments; limited entry points |
| Main cause | Steroids, alcohol, fracture of neck, sickle cell | Scaphoid waist/proximal fracture | Idiopathic + negative ulnar variance + trauma | Displaced talar neck fracture (forced dorsiflexion) |
| Main vessel disrupted | Medial circumflex femoral artery | Distal to proximal intraosseous flow | Lunate's single vessel (Gelberman pattern) | Artery of tarsal canal + deltoid artery |
| Classic demographic | Men 35-45; bilateral >50% | Young adult post-trauma (FOOSH) | Men 20-40; manual labourers; dominant wrist | High-energy trauma (MVA, fall) |
| Key X-ray sign | Crescent sign; sclerosis; head flattening | Sclerosis of proximal pole; nonunion | Lunate sclerosis, collapse, carpal height loss | Absent Hawkins sign at 6-8 weeks |
| Best early investigation | MRI | MRI | MRI (T1 low signal diffusely) | MRI / bone scan; CT for fracture planning |
| Staging system | Steinberg (0-VI) | None standard | Lichtman (I-IV) | Hawkins (I-IV) - for fracture/AVN risk |
| Pre-collapse surgery | Core decompression ± vascularised graft | Headless compression screw fixation | Joint-levelling osteotomy (radial shortening) | ORIF - urgent reduction + screw fixation |
| End-stage surgery | Total hip replacement | Wrist fusion / proximal row carpectomy | Wrist arthrodesis | Tibiotalar / tibiotalocalcaneal arthrodesis |
| AVN rates by type | Depends on cause | ~15-30% proximal pole fractures | Progressive if untreated | Type I: 0-15%; Type II: ~42%; Type III: ~91%; Type IV: ~100% |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Schwartz's Principles of Surgery 11th Ed; Bailey & Love's Short Practice of Surgery 28th Ed; Miller's Review of Orthopaedics 9th Ed; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.