77 year male having hypercalcemia renal dysfunction anaemia multiple fractures over bone plasma cell 33 percent on flow cytometry what is the diagnosis as per guidelines
Reading File
Finding Sources
Searching PubMed
"multiple myeloma" AND "diagnostic criteria" AND "IMWG"
Finding Sources
Searching PubMed
"multiple myeloma" AND "diagnosis"
Reading File
Reading File
Reading Article
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed to provide a thorough, guideline-based answer.
Diagnosis: Multiple Myeloma (Symptomatic)
This patient's presentation maps perfectly to the IMWG (International Myeloma Working Group) 2014 diagnostic criteria for symptomatic multiple myeloma, as published in Goldman-Cecil Medicine and confirmed by Rajkumar SV (Am J Hematol 2024).
Applying the IMWG Diagnostic Criteria
Step 1 - Clonal bone marrow plasma cells:
The patient has 33% plasma cells on flow cytometry - this meets the requirement of ≥10% clonal bone marrow plasma cells.
Step 2 - Myeloma-Defining Events (MDE):
At least one MDE must be present. This patient has ALL FOUR "CRAB" criteria:
| CRAB Feature | Patient | Threshold |
|---|---|---|
| C - Hypercalcemia | ✅ Present | Serum Ca >11 mg/dL or >1 mg/dL above upper limit of normal |
| R - Renal dysfunction | ✅ Present | Creatinine clearance <40 mL/min or serum Cr ≥2 mg/dL |
| A - Anemia | ✅ Present | Hb <10 g/dL or ≥2 g/dL below lower limit of normal |
| B - Bone lesions | ✅ Multiple fractures | ≥1 osteolytic lesion on X-ray, CT, or PET-CT |
Conclusion: Both criteria are met → Diagnosis = Symptomatic Multiple Myeloma
Why NOT Smoldering Myeloma or MGUS?
- MGUS requires: <10% plasma cells AND absence of CRAB - ruled out (patient has 33% cells + full CRAB)
- Smoldering MM requires: ≥10% plasma cells BUT no CRAB events and no MDE - ruled out (patient has all four CRAB features)
- Symptomatic MM is confirmed when CRAB or biomarker MDEs are attributable to the plasma cell disorder
Pathophysiologic Explanation of Findings
Each finding in this patient is mechanistically explained by myeloma:
-
Hypercalcemia: Myeloma cells upregulate RANKL on bone marrow stromal cells, activating osteoclasts and increasing bone resorption, releasing calcium into the blood. (Robbins & Kumar Basic Pathology)
-
Renal dysfunction: Caused by obstructive Bence Jones protein casts in distal convoluted tubules/collecting ducts, hypercalcemia-induced dehydration/nephrocalcinosis, and light chain deposition in glomeruli or interstitium. (Robbins & Kumar; Comprehensive Clinical Nephrology 7e)
-
Anemia: Plasma cell replacement of normal marrow suppresses erythropoiesis. Cytokines, renal failure, and inflammatory changes compound this.
-
Multiple fractures / bone lesions: Lytic lesions from osteoclast activation + osteoblast inhibition. Most common sites are vertebral column, ribs, skull, pelvis, and femur. (Robbins & Kumar Basic Pathology)
-
33% plasma cells: This is a high plasma cell burden, well above the 10% threshold.
Additional Biomarker MDEs (Beyond CRAB) to Check
Even without CRAB, any ONE of these also qualifies for MDE:
- Clonal plasma cells ≥60% (patient has 33% - does not meet this alone)
- Serum FLC ratio ≥100 (with involved FLC ≥100 mg/L)
- >1 focal lesion on MRI (≥5 mm)
Key Epidemiologic Note
Multiple myeloma has a median age at diagnosis of 70 years, making this 77-year-old patient squarely within the typical demographic. It is also more common in males. (Robbins & Kumar Basic Pathology)
Summary Statement
This patient meets the IMWG 2014 criteria for symptomatic multiple myeloma: clonal bone marrow plasma cells ≥10% (33% on flow cytometry) PLUS at least one myeloma-defining event (in this case, all four CRAB criteria are present).
Source references:
- Goldman-Cecil Medicine, Table 173-2: Criteria for the Diagnosis of Plasma Cell Disorders
- Comprehensive Clinical Nephrology 7e (IMWG 2014 criteria summary)
- Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol 2024. [PMID: 38943315]
What is MGUS
Finding Sources
Searching PubMed
"monoclonal gammopathy of undetermined significance" AND "progression"
Reading File
Reading Article
Reading File
Loading Image
Here is a complete, guideline-based overview of MGUS:
MGUS - Monoclonal Gammopathy of Undetermined Significance
Definition
MGUS (formerly called "benign monoclonal gammopathy") is a premalignant clonal plasma cell disorder characterized by the presence of a serum M protein (monoclonal immunoglobulin) in persons who lack evidence of multiple myeloma, macroglobulinemia, amyloidosis, or other related diseases.
Think of it as the "silent precursor" on the spectrum of plasma cell disorders - the clone exists, but has not yet caused any organ damage.
Diagnostic Criteria (IMWG)
ALL THREE of the following must be present:
| Criterion | Threshold |
|---|---|
| Serum M protein (non-IgM type) | < 3 g/dL |
| Clonal bone marrow plasma cells | < 10% |
| No CRAB features (hypercalcemia, renal failure, anemia, bone lesions) | Absent |
The moment any CRAB feature appears, or plasma cells exceed 10%, the diagnosis escalates beyond MGUS.
Three Subtypes of MGUS
| Type | Plasma Cell % | M Protein | Progression Risk |
|---|---|---|---|
| Non-IgM MGUS | <10% | IgG/IgA <3 g/dL | → Multiple myeloma / AL amyloidosis |
| IgM MGUS | <10% lymphoplasmacytic | IgM >3 g/dL | → Waldenström macroglobulinemia |
| Light chain MGUS | <10% | No heavy chain; abnormal FLC ratio | → Light chain myeloma / AL amyloidosis |
(Goldman-Cecil Medicine, Table 173-2)
Epidemiology
- Prevalence rises sharply with age: ~1% in persons aged 50-60 years → >5% in those over 70 years
- More common in males than females
- Twice as prevalent in Blacks compared to Whites
- Nearly 5% of adults overall have MGUS (JAMA Internal Medicine, 2025)
- Often detected incidentally on routine serum protein electrophoresis (SPEP)
The Spectrum - How MGUS Fits In
MGUS → Smoldering Myeloma → Symptomatic Multiple Myeloma
(no CRAB) (no CRAB, higher burden) (CRAB + ≥10% plasma cells)
Risk of Progression
The key clinical concern with MGUS is its fixed, lifelong progression rate of ~1% per year to myeloma or a related malignancy. Risk stratification uses three factors (Mayo Clinic model):
| Risk Factor | Adverse Feature |
|---|---|
| M protein level | ≥1.5 g/dL |
| Immunoglobulin subtype | Non-IgG (IgA or IgM) |
| Free light chain (FLC) ratio | Abnormal (<0.26 or >1.65) |
| Risk Group | Cumulative Progression at 20 yrs |
|---|---|
| Low risk (0 factors) | 5% |
| Low-intermediate (1 factor abnormal) | 21% |
| High-intermediate (2 factors abnormal) | 37% |
| High risk (all 3 abnormal) | 58% |
(Goldman-Cecil Medicine, Table 173-3; Rajkumar et al., Blood 2005)
Pathobiology
- Etiology is unknown; risk factors include: age, male sex, family history, immunosuppression, certain pesticide exposures
- ~40% have IgH translocations (chromosome 14q32) involving partners like CCND1, FGFR3, c-maf
- ~40% show trisomies of odd-numbered chromosomes (hyperdiploid pattern)
- On flow cytometry: normal polyclonal plasma cells coexist alongside the clonal cells - this distinguishes it from myeloma where normal plasma cells are displaced
Diagnosis and Management Approach
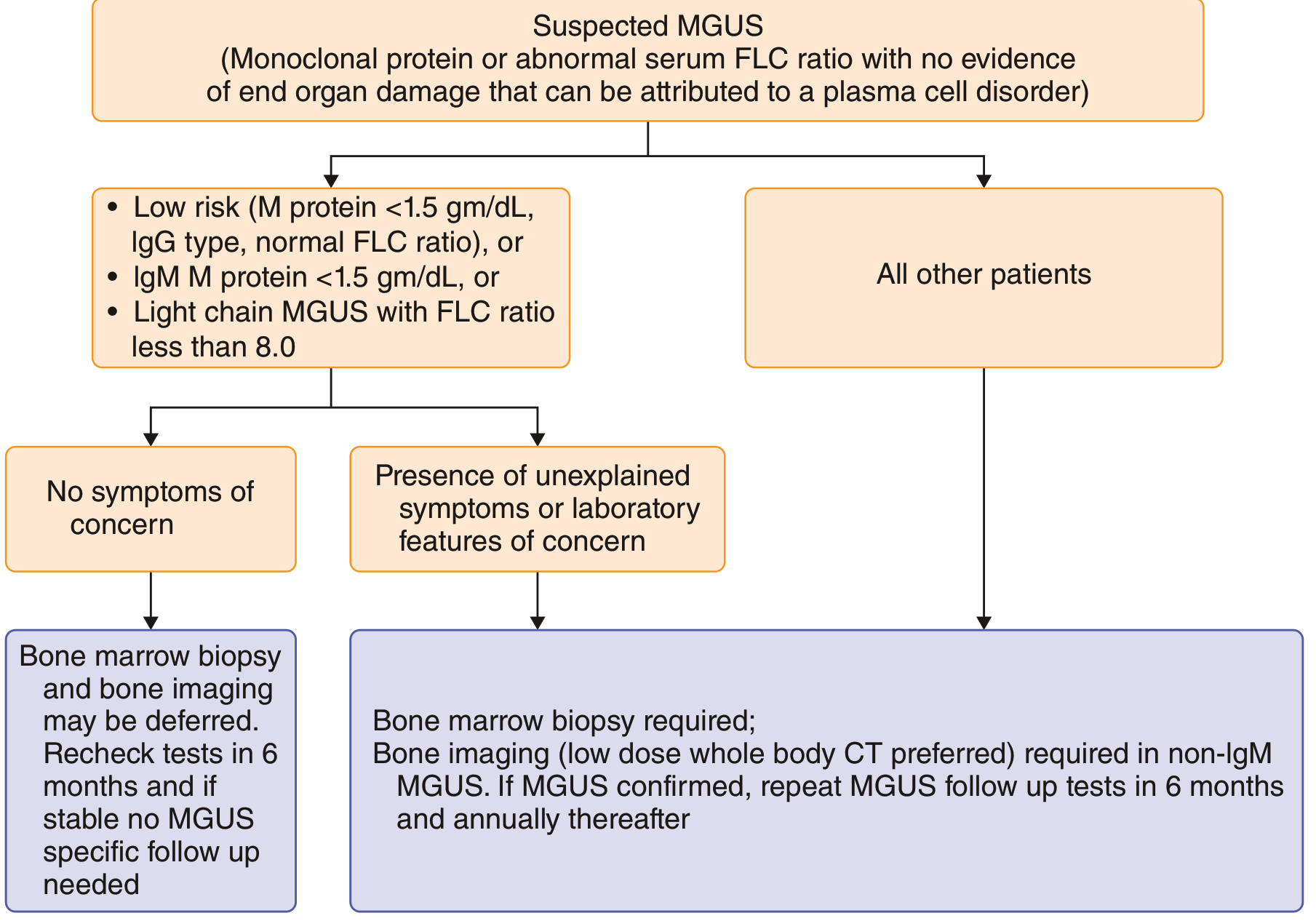
Goldman-Cecil Medicine - Approach to diagnosis and management of MGUS
- Low-risk MGUS (IgG, M protein <1.5 g/dL, normal FLC ratio, no symptoms): bone marrow biopsy and imaging may be deferred; recheck labs in 6 months, then no specific follow-up if stable
- All other MGUS: bone marrow biopsy required; bone imaging (low-dose whole-body CT preferred) for non-IgM MGUS; repeat follow-up at 6 months then annually
No treatment is indicated for MGUS itself. Management is monitoring only, with attention to signs of progression.
Key Contrast: MGUS vs Previous Patient's Diagnosis
| Feature | MGUS | Symptomatic MM (Previous Patient) |
|---|---|---|
| Plasma cells | <10% | 33% (≥10%) |
| M protein | <3 g/dL | Can be ≥3 g/dL |
| Hypercalcemia | Absent | Present |
| Renal dysfunction | Absent | Present |
| Anemia | Absent | Present |
| Bone lesions/fractures | Absent | Present (multiple) |
The previous patient clearly had none of the MGUS-defining limits - he had crossed into full symptomatic multiple myeloma.
Sources:
- Goldman-Cecil Medicine, Chapter 173 (Plasma Cell Proliferative Disorders)
- Liu Y, Parks AL. Diagnosis and Management of MGUS: A Review. JAMA Intern Med. 2025. [PMID: 39960681]
This is a shared conversation. Sign in to Orris to start your own chat.