PEPTIC ULCER
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND "Helicobacter pylori"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer:
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is an excoriated defect in the mucosa of the stomach or duodenum caused by the digestive action of gastric acid and pepsin. The name "peptic" suggests a pepsin association, but acid is the critical factor - in the absence of acid, peptic ulcers do not occur. Nearly all peptic ulcers can be healed by proton pump inhibitors (PPIs), which render a patient virtually achlorhydric.
- Guyton and Hall Textbook of Medical Physiology, p. 825
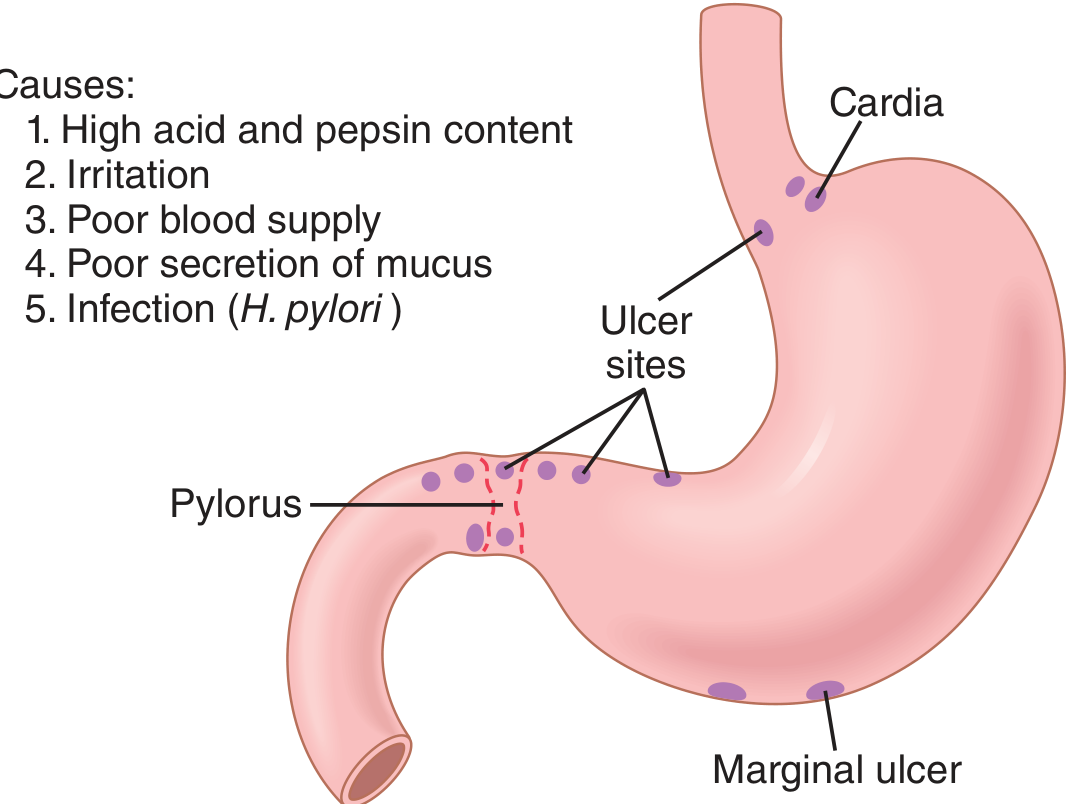
Sites of Occurrence
The most common locations are:
- First part of the duodenum (most frequent)
- Lesser curvature of the gastric antrum
- Stomal/marginal ulcers (at anastomoses after gastric surgery)
- Lower esophagus (in GERD or ectopic gastric mucosa)
- A Meckel's diverticulum (containing ectopic gastric epithelium)
- Rarely, the jejunum (in Zollinger-Ellison syndrome)
Ulcers generally occur at the junction between different epithelial types, in the epithelium least resistant to acid damage.
Epidemiology
-
Affects >4 million individuals in the US each year
-
Lifetime risk: ~10% in males, ~4% in females
-
Duodenal ulcers are more common than gastric ulcers
-
Previously, peptic ulcer accounted for ~50% of upper GI bleeds and ~100,000 hospitalizations/year in the US
-
The incidence of H. pylori-related ulcers is declining in the West; NSAID-related ulcers are becoming proportionally more common
-
Robbins & Kumar Basic Pathology, p. 3903
Pathogenesis
Core Concept: Imbalance of Offense vs. Defense
PUD results from an imbalance between aggressive (acid/pepsin) and defensive (mucosal barrier) forces:
Defensive mechanisms:
- Mucus secretion (surface mucous cells, Brunner's glands)
- Bicarbonate secretion (pancreatic juice, liver bile)
- Mucosal blood flow and prostaglandins
- Feedback inhibition of acid when duodenal pH drops (secretin release, enterogastrone hormones)
Offensive disruption causes:
1. Helicobacter pylori (H. pylori)
- Responsible for >70% of PUD cases
- A gram-negative spiral bacterium that colonizes under the mucus layer of the gastric antrum
- Breaks down the mucosal barrier via: urease (produces ammonia that damages mucosa), proteases, vacuolating cytotoxin (VacA), and CagA virulence factor
- Stimulates excessive gastrin secretion and thus acid hypersecretion
- Causes mucosal inflammation (chronic active gastritis), particularly in the antrum, which when extensive impairs protective mechanisms
- Only 5-10% of infected individuals develop ulcers - host factors and bacterial strain variation matter
- H. pylori eradication eliminates ulcer recurrence (recurrence rate falls from ~80% to ~2%)
2. NSAIDs (including aspirin)
- Inhibit COX-1 and COX-2, reducing prostaglandin synthesis
- Prostaglandins normally stimulate mucus and bicarbonate secretion, maintain mucosal blood flow, and promote epithelial repair
- NSAID-related ulcers tend to be gastric and occur in older populations
- In the US, NSAID use is becoming the most common cause of gastric ulcers as H. pylori rates fall
3. Acid Hypersecretion
- Direct cause in Zollinger-Ellison syndrome (gastrinoma) - multiple ulcers, often in unusual sites (distal duodenum, jejunum)
- Parietal cell hyperplasia
- Excessive secretory responses to stimulation
- Hypercalcemia (hyperparathyroidism, CRF) stimulates gastrin and acid
4. Other Risk Factors
-
Cigarette smoking - reduces mucosal blood flow, impairs healing, increases relapse rate
-
Corticosteroids (high-dose) - suppress prostaglandin synthesis
-
Alcohol-related cirrhosis, COPD, chronic renal failure, hyperparathyroidism
-
Psychological stress (physiological stress ulcers in ICU patients)
-
Robbins Basic Pathology; Bailey & Love Surgery; Guyton & Hall
Morphology (Pathology)
- Ulcers are typically solitary, round to oval, sharply "punched-out" defects with nearly vertical walls
- The base is clean and smooth (unlike carcinoma, which is necrotic and irregular)
- Size: usually <2 cm diameter for duodenal; gastric ulcers may be larger
- Chronic ulcers penetrate into the muscularis propria and may reach the serosa
- Healing leads to residual mucosal scarring; fibrosis can cause pyloric stenosis
- "Kissing ulcers" = both anterior and posterior duodenal ulcers coexisting
- Anterior duodenal ulcers tend to perforate; posterior duodenal ulcers tend to bleed (eroding the gastroduodenal artery)
Microscopy:
- Active ulcer base shows: necrotic fibrinoid debris (surface), inflammatory exudate, granulation tissue, fibrous scar (deepest layer)
- Adjacent mucosa shows features of chronic gastritis if H. pylori is the cause
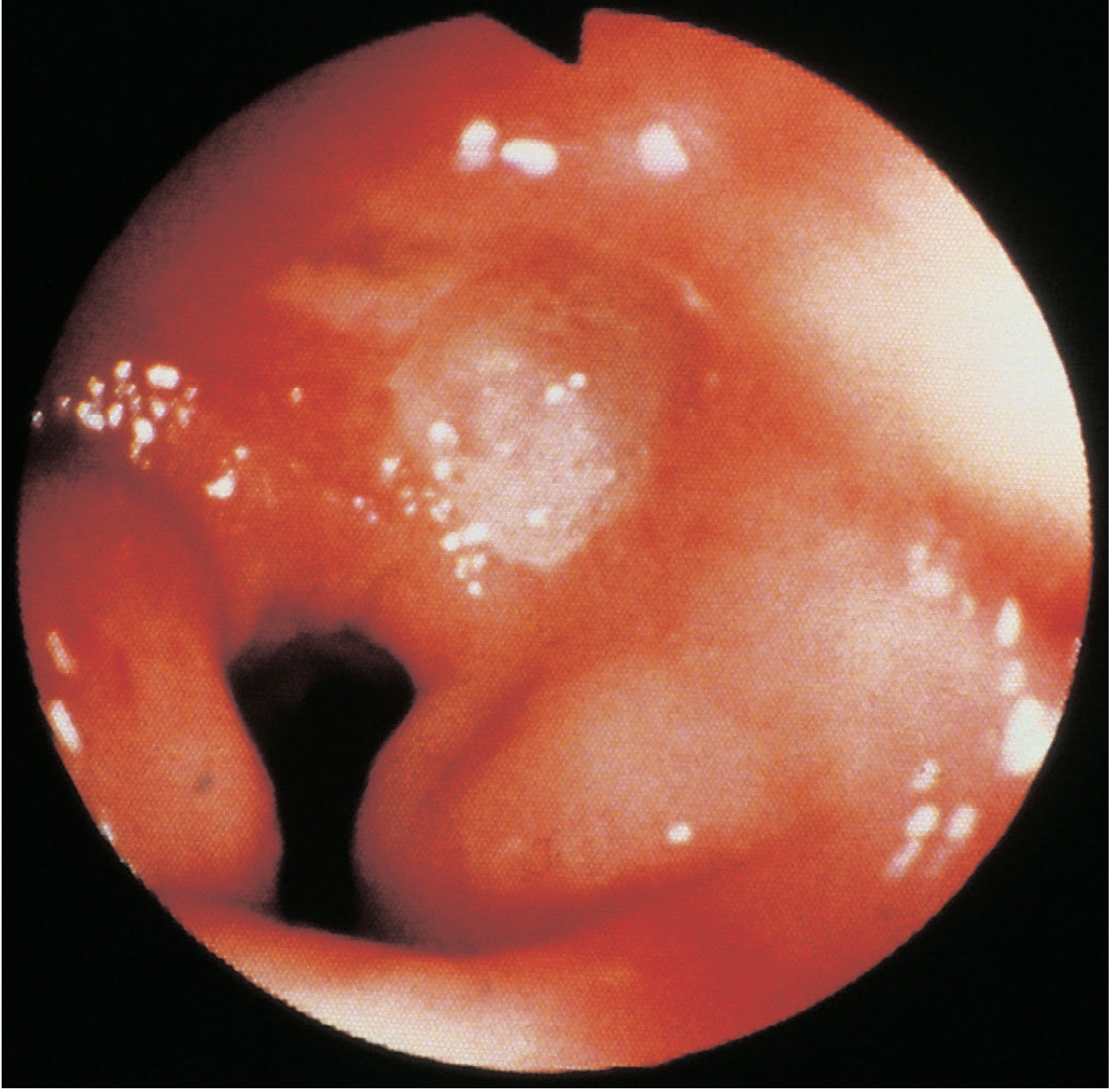
Endoscopic Appearance
Clinical Features
Gastric and duodenal ulcers cannot be reliably distinguished by symptoms alone.
| Feature | Description |
|---|---|
| Pain | Epigastric, gnawing or burning, may radiate to the back |
| Pattern | Episodic with spontaneous remissions ("periodicity") |
| Relation to food | Eating may relieve discomfort (especially DU), or worsen it |
| Nocturnal pain | Common in DU; wakes patients at night |
| Vomiting | Not prominent unless stenosis |
| Weight | May lose weight (especially GU); may gain (food relieves DU pain) |
| Bleeding | Hematemesis or melena; may be occult |
Investigations
Non-invasive H. pylori Tests
- Urea breath test (UBT) - gold standard non-invasive test for active infection; avoid PPIs 2 weeks before
- Stool antigen test - reliable, useful for follow-up confirmation of eradication
- Serology - detects antibodies (IgG); cannot distinguish active from past infection; not reliable for post-treatment confirmation
Invasive (Endoscopic Biopsy)
- Rapid urease test (CLO test) - biopsy-based, rapid
- Histology - gold standard for confirmation and assessment of gastritis pattern
- Culture - for antibiotic sensitivity testing
Endoscopy (OGD/EGD)
- Direct visualization, localization, biopsy
- All gastric ulcers must be biopsied (at least 6-10 targeted biopsies) to exclude malignancy - gastric cancer can mimic benign ulcer, and PPIs can heal the ulceration without treating the underlying malignancy
- Repeat endoscopy with biopsy after treatment to confirm healing of gastric ulcers
Imaging
- Barium meal (upper GI series): historically used; ulcer shown as a niche/crater; largely superseded by endoscopy for most cases
Treatment
1. NSAID-Associated PUD
- Stop the NSAID if possible (or switch to a selective COX-2 inhibitor with a PPI)
- PPI (e.g., omeprazole) for 4-8 weeks - heals most ulcers
- Test for H. pylori and eradicate if co-present
2. H. pylori Eradication
Indications for eradication (ACG/Maastricht VI guidelines):
- Documented PUD (active or historical) - regardless of whether NSAIDs are also used
- Gastric MALT lymphoma (60-90% achieve complete remission with eradication alone)
- After endoscopic resection of early gastric cancer
- Uninvestigated dyspepsia in patients <60 years (test-and-treat if local prevalence >20%)
- Pre-NSAID therapy (reduces GI bleeding risk)
- Unexplained iron-deficiency anemia or ITP
First-Line Regimens (14-day courses preferred):
| Regimen | Drugs | When to Use |
|---|---|---|
| Standard Triple Therapy | PPI + clarithromycin + amoxicillin | No penicillin allergy, no prior macrolide, local clarithromycin resistance <15% |
| Bismuth Quadruple Therapy | PPI + bismuth + tetracycline + metronidazole | Prior macrolide exposure, clarithromycin resistance >15%, or penicillin allergy with recent metronidazole |
| Concomitant Therapy | PPI + clarithromycin + amoxicillin + nitroimidazole | Alternative first-line option |
| Levofloxacin Triple | PPI + levofloxacin + amoxicillin | Second-line or penicillin-allergy alternatives |
- Eradication rates with initial therapy: ~80-90%; ~20-30% fail due to antibiotic resistance (especially clarithromycin and metronidazole resistance)
- Confirm eradication with UBT or stool antigen 4-6 weeks after completing therapy (wait 2 weeks off PPI)
- Sabiston Textbook of Surgery; Harrison's Principles of Internal Medicine 22E
3. Acid Suppression Alone (Maintenance)
- H. pylori-negative, non-NSAID ulcers - long-term PPI therapy
- Zollinger-Ellison syndrome - high-dose PPI indefinitely (unless tumor resectable)
Complications
The three classic complications: Bleeding, Perforation, Stenosis (obstruction)
1. Bleeding (Most Common)
- Most common complication; accounts for ~50% of upper GI bleeds
- Posterior DU may erode the gastroduodenal artery (catastrophic hemorrhage)
- Presents as hematemesis, melena, or hemodynamic instability
- Rockall Score stratifies risk of rebleeding and mortality:
| Score | Rebleeding Rate | Mortality |
|---|---|---|
| 0-1 | <5% | 0% |
| 3-4 | ~11-14% | 3-5% |
| 5 | 24% | 11% |
| ≥7 | ~43% | 27-41% |
- Management: resuscitation, urgent OGD, endoscopic hemostasis (injection, thermal, clips); H. pylori eradication postoperatively reduces recurrence from 20% to near zero
- Sleisenger and Fordtran's GI and Liver Disease
2. Perforation
- Anterior DU perforates most often (into the peritoneal cavity)
- Classic presentation: sudden severe epigastric pain, board-like rigid abdomen, free air under the diaphragm on erect CXR
- Treatment primarily surgical (oversewing of perforation + peritoneal lavage); conservative management (Teylor's method) in selected patients
- Perforated gastric ulcer must be excised and sent for histology to exclude malignancy
3. Pyloric Stenosis / Gastric Outlet Obstruction
- Results from chronic scarring and fibrosis from repeated ulcer healing
- Presents with: large volume vomiting, succussion splash, visible peristalsis, hypochloraemic hypokalaemic metabolic alkalosis
- Most commonly associated with longstanding PUD or gastric cancer
- Treatment: nasogastric decompression, IV fluid/electrolyte correction, then definitive endoscopic or surgical intervention
Surgery (Now Rarely Done Electively)
Elective acid-reducing surgery is now essentially obsolete due to PPIs and H. pylori eradication. Operations are reserved for emergencies:
- Billroth I (distal gastrectomy with gastroduodenostomy)
- Billroth II / Pólya (distal gastrectomy with gastrojejunostomy)
- Highly selective vagotomy (preserves gastric emptying)
- Long-term complications of gastric surgery: dumping syndrome, bile reflux gastritis, B12 deficiency, iron-deficiency anaemia, stomal/marginal ulcers
Differential Diagnosis
- Acute cholecystitis / cholelithiasis
- Pancreatitis
- Gastric carcinoma (must always be excluded in gastric ulcers)
- GERD / esophagitis
- Functional dyspepsia
- Appendicitis (atypical presentations)
- Ischemic bowel disease (elderly)
- IBD (Crohn's disease can involve upper GI tract)
Key Clinical Pearls
- No acid = no ulcer: PPIs are the backbone of both healing and maintenance therapy
- All gastric ulcers must be biopsied: malignancy cannot be excluded on appearance alone, and PPIs can heal the surface without treating the cancer
- H. pylori eradication changes natural history: reduces recurrence from ~80% to ~2%
- Posterior DU bleeds; anterior DU perforates - relates to anatomical proximity to the gastroduodenal artery
- NSAID ulcers are increasing as a proportion in developed countries as H. pylori prevalence declines; often silent until a complication occurs
- Zollinger-Ellison should be suspected in H. pylori-negative, non-NSAID refractory ulcers - check fasting serum gastrin
- Eradication confirmation is mandatory (UBT or stool antigen 4-6 weeks post-treatment)
Sources: Bailey & Love's Short Practice of Surgery 28e | Robbins & Kumar Basic Pathology | Guyton & Hall Medical Physiology | Harrison's Principles of Internal Medicine 22E (2025) | Sabiston Textbook of Surgery | Sleisenger & Fordtran's GI and Liver Disease | Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.