Liposarcoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
liposarcoma
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative textbooks. Let me compose the full answer.
Liposarcoma
Overview
Liposarcoma is a malignant tumor of adipose tissue and the most common soft tissue sarcoma (STS) of adulthood. It typically affects individuals in their 50s and 60s, presenting as a large, deep-seated, painless mass. It accounts for 45% of all retroperitoneal sarcomas. - Robbins & Kumar Pathologic Basis of Disease; Sabiston Textbook of Surgery
Subtypes and Pathogenesis
There are three major histologic subtypes, each with distinct genetics and behavior:
1. Well-Differentiated Liposarcoma (WDL) / Atypical Lipomatous Tumor (ALT)
- Most common subtype, listed in order of decreasing frequency (WDL/dedifferentiated > myxoid > pleomorphic).
- Genetics: Amplification of chromosome region 12q13-q15, including the MDM2 gene and CDK4. MDM2 acts as an oncoprotein by promoting p53 proteasomal degradation.
- The terms ALT (extremity/superficial trunk) and WDL (retroperitoneum, mediastinum, paratesticular) describe histologically identical tumors in different anatomic locations - the distinction exists because retroperitoneal tumors are harder to resect and more prone to recurrence.
- Dedifferentiated liposarcoma is a progression variant of WDL; it carries a higher risk of distant metastasis.
- IHC: MDM2 and CDK4 positivity helps distinguish from lipoma and other sarcomas.
2. Myxoid Liposarcoma
- Second most common subtype; ~5% of all soft tissue sarcomas in adults.
- More common in the extremities; tends to affect younger to middle-aged adults.
- Genetics: Translocation t(12;16)(q13;p11) → FUS::DDIT3 fusion gene (rarely EWSR1-DDIT3 from t(12;22)). This arrests adipocyte differentiation → proliferation of primitive mesenchymal cells. Activates MET, RET, and PI3K/Akt pathways.
- Intermediate local recurrence (~20%) and metastatic risk (~50%).
- Unique metastatic pattern: metastasizes to bone and retroperitoneum (unusual for soft tissue sarcomas; other STS metastasize mainly to lung).
- Myxoid liposarcoma is notably radiosensitive and chemosensitive; 10-year disease-specific survival ~87%.
- Round cell liposarcoma = poorly differentiated variant of myxoid liposarcoma; worse prognosis with distant metastasis rates up to 21%.
3. Pleomorphic Liposarcoma
- Least common but most aggressive subtype.
- Genetics: Complex karyotype without consistent/reproducible genetic abnormalities; no known targetable mutations.
- Sheets of anaplastic cells with bizarre nuclei admixed with lipoblasts.
- Predilection for the extremities of adults.
- Frequently metastasizes; poor prognosis.
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Sabiston Textbook of Surgery; Campbell's Operative Orthopaedics 15th Ed 2026
Histopathology
The sine qua non of liposarcoma is the presence of lipoblasts - immature fat cells with a hyperchromatic nucleus indented or scalloped by lipid vacuoles. - Dermatology 2-Volume Set 5e
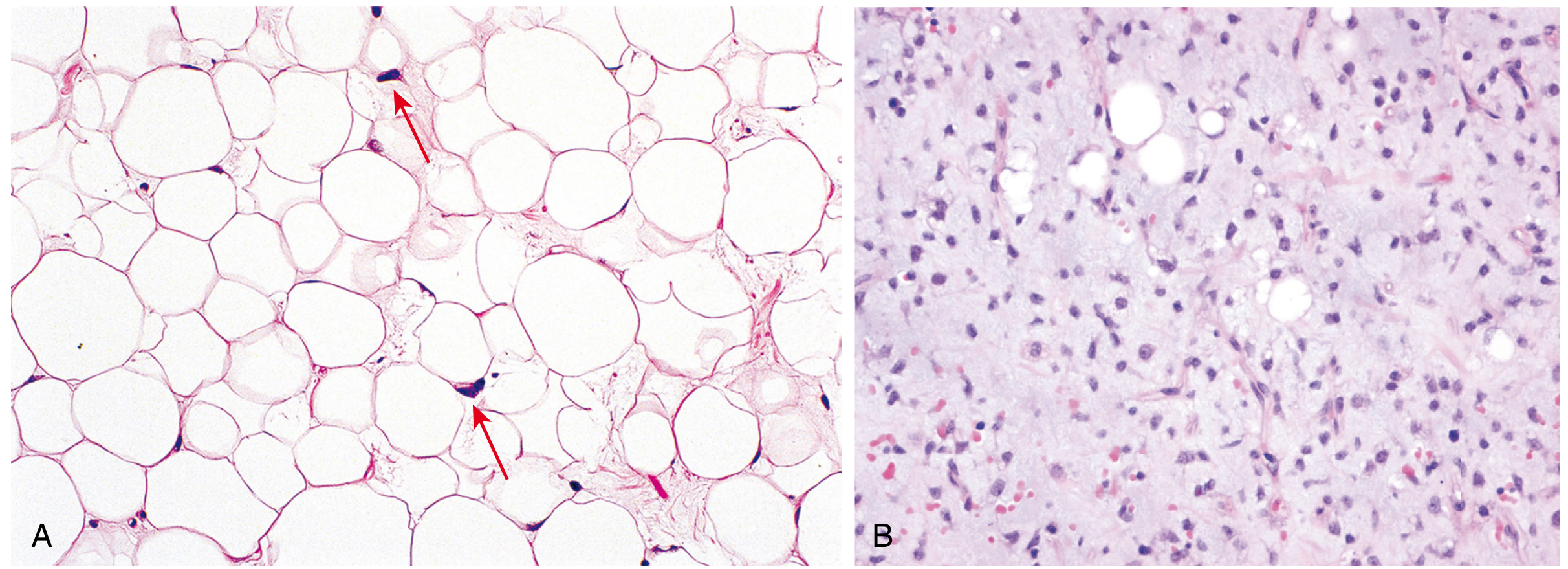
Fig. 26.42 Liposarcoma - Robbins & Kumar Pathologic Basis of Disease. (A) Well-differentiated: mature adipocytes + scattered atypical spindle cells with hyperchromatic nuclei. (B) Myxoid: abundant basophilic matrix, arborizing ("chicken-wire") capillaries, primitive cells resembling fetal fat.
| Subtype | Histology |
|---|---|
| Well-differentiated | Mature adipocytes + scattered atypical stromal cells |
| Myxoid | Basophilic matrix + arborizing capillaries + primitive adipocytes |
| Round cell | Hypercellular myxoid areas with round overlapping nuclei |
| Pleomorphic | Sheets of anaplastic cells + bizarre nuclei + lipoblasts |
| Dedifferentiated | Abrupt transition from WDL to high-grade non-lipogenic sarcoma |
Clinical Features and Location
| Feature | Well-Differentiated/Dedifferentiated | Myxoid/Round Cell | Pleomorphic |
|---|---|---|---|
| Common location | Retroperitoneum, mediastinum | Extremities (thigh) | Extremities |
| Typical age | 50s-60s | Younger adults | Adults |
| Local recurrence | Common (especially retroperitoneal) | Intermediate (~20%) | High |
| Metastatic risk | Low (WDL); higher (dediff.) | ~50%; to bone/retroperitoneum | Frequent |
| Prognosis | Good (extremity); guarded (retroperitoneal) | Intermediate (87% 10-yr DSS) | Poor |
Imaging
- Plain radiographs: Usually normal.
- MRI: Best modality. Well-differentiated tumors show characteristic fat signal. Features suggesting malignancy over lipoma: tumor >10 cm, thick septa (>2 mm), non-adipose areas, <75% adipose tissue.
- CT: Used for retroperitoneal tumors. Features suggesting dedifferentiation: hypervascularity, necrosis/cystic change, adjacent organ invasion, focal nodular or water-density areas.
- MRI/CT can distinguish WDL from dedifferentiated tumors but can be difficult in large, heterogeneous lesions.
- Sabiston Textbook of Surgery; Campbell's Operative Orthopaedics 15th Ed
Treatment
Surgery (Mainstay)
- Extremity tumors (ALT/WDL): Limb-sparing resection with negative margins. Limited resection is appropriate given low metastatic risk. Neoadjuvant/perioperative radiation reduces local recurrence risk.
- Retroperitoneal liposarcoma: Gross complete resection is the principal goal - incomplete resection increases mortality. Traditionally involves resection of contiguous organs. Some advocate complete compartmental resection (spleen, pancreas, diaphragm, adrenal, kidney resected in >50% of cases), though this remains debated. Out-of-compartment recurrences (~15%) would not be prevented by this approach.
- Recurrent retroperitoneal disease: Resection is favored when tumor growth rate is <0.9 cm/month.
Radiation Therapy
- Reduces local recurrence, especially for extremity tumors.
- Preferably given in the neoadjuvant (preoperative) setting.
- Myxoid liposarcoma is particularly radiosensitive.
Chemotherapy
- Role is controversial for most subtypes.
- Myxoid liposarcoma is uniquely chemosensitive (anthracycline-based regimens).
- High-grade tumors: standard first-line is anthracycline-based (doxorubicin ± ifosfamide).
- A 2025 systematic review (PMID: 40257618) evaluated immune checkpoint inhibitors + anthracyclines as a potential first-line regimen for dedifferentiated liposarcoma - emerging evidence for immunotherapy combinations.
- Sabiston Textbook of Surgery; Campbell's Operative Orthopaedics; Fischer's Mastery of Surgery
Poor Prognostic Indicators
- High histologic grade
- Large tumor size
- Proximal or deep location
- Presence of metastases
- Retroperitoneal location (vs. extremity)
- Dedifferentiated or pleomorphic histology
- Campbell's Operative Orthopaedics 15th Ed 2026
Key Genetic Summary Table
| Subtype | Genetic Abnormality | Key Oncogene |
|---|---|---|
| Well-differentiated / Dedifferentiated | Amplification 12q13-q15 | MDM2, CDK4 |
| Myxoid / Round cell | t(12;16) → FUS::DDIT3; rarely t(12;22) → EWSR1-DDIT3 | DDIT3 (CHOP) |
| Pleomorphic | Complex karyotype | No consistent target |
This is a shared conversation. Sign in to Orris to start your own chat.