teach me Tracheostomy with all concepts
Reading File
Finding Sources
Searching the Web
tracheostomy indications procedure complications nursing care comprehensive review
Searching PubMed
tracheostomy indications complications management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from 6 authoritative textbooks. Let me compile the complete teaching guide on tracheostomy.
Tracheostomy: Complete Teaching Guide
1. Definition & Historical Background
A tracheostomy is the creation of an opening (stoma) in the anterior wall of the trachea through which a tube is inserted to establish or maintain an airway. The term is sometimes confused with tracheotomy (the surgical incision only); "tracheostomy" refers to the full procedure including the stoma and tube placement.
Historical highlights:
- First recorded open tracheostomy: >3,500 years ago (Egyptian dynasty stone slabs)
- Fabricius described the first tracheal cannula in 1617
- Sanctorio Sanctorius: first percutaneous tracheostomy in 1626, using a "ripping needle" to place a silver cannula
- First cuffed tracheostomy tube: 1869, by Trendelenburg
- Modern standardization: early 20th century by American surgeon Chevalier Jackson
- PDT via Seldinger guidewire: Toye & Weinstein (late 1960s)
- Current single-dilator PDT: Pasquale Ciaglia, 1985
Source: Current Surgical Therapy 14e
2. Relevant Anatomy
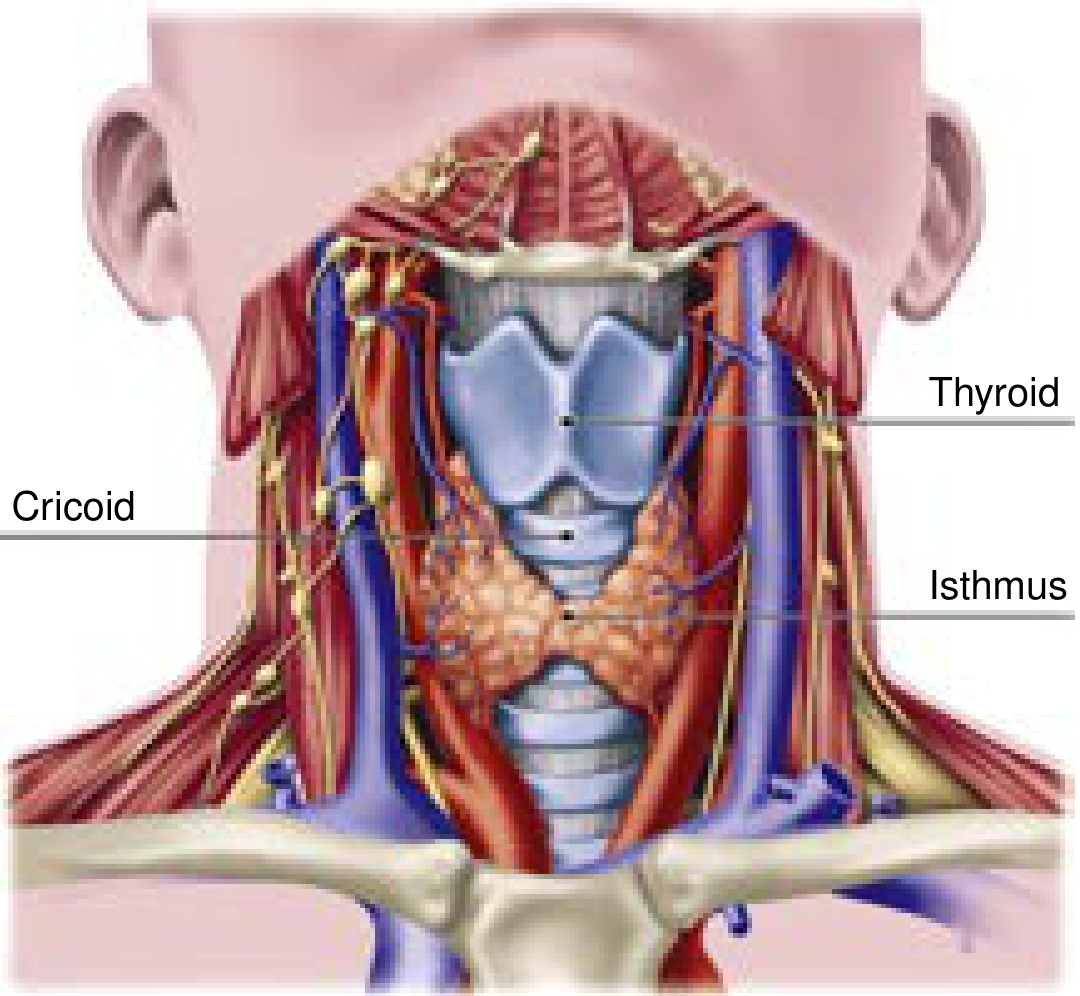
Tracheal anatomy - Current Surgical Therapy 14e, p.1591
Key anatomical facts:
| Structure | Detail |
|---|---|
| Tracheal length | 10-12 cm (avg 11 ± 1 cm males, 10 ± 1 cm females) |
| Cartilaginous rings | 18-22 incomplete semicircular rings (posterior wall = fibroelastic membrane) |
| Tracheal diameter | 12-25 mm; varies by sex (2.5-2.7 mm men, 2.1-2.3 mm women) |
| Cricoid cartilage | Only complete cartilaginous ring; attached to 1st tracheal ring below and thyroid cartilage above |
| Ideal tracheostomy site | Between 2nd-3rd tracheal rings (sometimes 1st-2nd) |
| Innominate (brachiocephalic) artery | Courses anterior to the trachea - tracheostomy too low = risk of tracheo-innominate fistula |
| Thyroid isthmus | Overlies tracheal rings 2-4 (must be divided or retracted) |
| Posterior tracheal wall | Shared wall with the esophagus - key risk for perforation |
The lower respiratory tract begins at the vocal cords. The subglottic space (1.5-2 cm) lies between the cords and the cricoid cartilage. The cricothyroid membrane lies between the thyroid and cricoid cartilages - the landmark for emergency cricothyrotomy.
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Current Surgical Therapy 14e
3. Indications
Indications fall into three broad categories:
A. Upper Airway Obstruction
- Head and neck tumors (laryngeal, hypopharyngeal, thyroid)
- Severe maxillofacial trauma
- Angioedema (hereditary or allergic)
- Bilateral vocal cord paralysis
- Foreign body not removable endoscopically
- Epiglottitis with impending obstruction
- Burns/inhalation injury with anticipated swelling
B. Prolonged Mechanical Ventilation
- Most common indication in the ICU
- Considered when ventilation >10-14 days without near-term extubation prospect
- Advantages over prolonged translaryngeal intubation:
- Reduced sedation requirements (no glottic stimulation)
- Reduced work of breathing and tube resistance
- Improved mouth care and oral hygiene
- Easier bronchopulmonary toilet
- Facilitates weaning by reducing dead space and resistance
- Better patient comfort and ability to communicate
C. Neurological Conditions Preventing Safe Extubation
- Severe traumatic brain injury (acute or progressive)
- Spinal cord injury (including patients in halo fixation)
- Prolonged altered mental status
- Severe agitation or delirium
- High aspiration risk with absent gag/cough
Source: Sabiston Textbook of Surgery; Scott-Brown's Otorhinolaryngology
4. Contraindications
All contraindications are relative (not absolute), and most are temporary:
| Contraindication | Reason |
|---|---|
| Recent anterior neck surgery (<7 days) | Distorted anatomy, friable tissue |
| FiO2 >50%, PEEP >10 cmH2O | Risk of catastrophic airway loss during procedure |
| Elevated intracranial pressure | Procedure can cause dangerous ICP spikes |
| Hemodynamic instability | Procedure risk outweighs benefit |
| Significant bleeding risk / coagulopathy | Need PT/PTT <1.5x control, platelets >50,000 |
| Local infection or malignancy at proposed site | Spread of infection, poor healing |
| Predicted early mortality | Futility of intervention |
| Advanced ventilator modes | Difficult to maintain oxygenation during procedure |
Tip: Uremic patients can have PDT performed safely if pretreated with DDAVP to improve platelet function.
Source: Sabiston Textbook of Surgery, p.960
5. Types of Tracheostomy
A. Open (Surgical) Tracheostomy (OST)
- Performed in the operating room (occasionally bedside)
- Direct visualization of tracheal rings
- A vertical incision is made between rings 2-4, then dilated; tube inserted under direct vision
- Neck extended; 2-3 cm incision ~2 cm above sternal notch through platysma and strap muscles
- Thyroid isthmus elevated or divided
- Stoma sutured to skin edges (matured tract in ~4-5 days)
- Preferred when: obesity with inaccessible landmarks, prior anterior neck surgery, severe coagulopathy, abnormal neck anatomy (goitre)
B. Percutaneous Dilatational Tracheostomy (PDT)
- Bedside procedure; standard of care in many ICUs
- Based on Seldinger technique:
- ETT withdrawn proximally under bronchoscopic control
- Needle inserted between rings 2-3 percutaneously
- Guidewire threaded through needle
- Serial dilations or single-dilator over guidewire
- Tracheostomy tube advanced over dilator/wire
- Bronchoscopic guidance is standard practice
- Cost-effective, no OR wait time needed
- Meta-analysis evidence: PDT has fewer wound infections and bleeding compared to OST; rates of serious complications are similar
C. Emergency Cricothyrotomy
- Not a true tracheostomy, but the emergency airway of last resort
- Incision through cricothyroid membrane (palpated below thyroid notch)
- Transverse incision to lateral borders of thyroid cartilage → rapid dilation → tube insertion
- Must be converted to formal tracheostomy within 24-72 hours (risk of subglottic stenosis)
Source: Mulholland and Greenfield's Surgery 7e; Current Surgical Therapy 14e
6. Tracheostomy Tubes: Types and Components
Basic Components of a Tracheostomy Tube
- Outer cannula - the main tube inserted into the trachea
- Inner cannula - removable, can be cleaned or replaced (critical for maintaining airway patency)
- Obturator - blunt-tipped guide inserted during tube placement; removed immediately after insertion
- Flange (neck plate) - holds the tube in position at skin surface; secured with tracheostomy ties
- Cuff (in cuffed tubes) - inflatable balloon that seals the trachea for positive-pressure ventilation
Types of Tubes
| Type | Key Feature | Use |
|---|---|---|
| Cuffed | Inflatable cuff seals airway | Mechanical ventilation, aspiration protection |
| Uncuffed | No cuff | Weaning, long-term use in non-ventilated patients |
| Fenestrated | Opening on dorsal surface of outer cannula | Allows air to pass through vocal cords → enables phonation and assessment of swallowing |
| Single cannula | No inner cannula | Smaller profile but cannot be cleared as easily |
| Double cannula | Removable inner cannula | Standard for most patients; inner cannula cleared regularly |
| Extended length | Longer shaft (proximal or distal) | Obese patients, large necks, abnormal anatomy |
| Metal (silver/stainless steel) | No cuff, no 15-mm connector | Long-term use, cannot be connected to ventilator |
| PVC (polyvinyl chloride) | Softens at body temperature | Most common |
| Silicone | Naturally soft | Biocompatible, less mucosal irritation |
Cuff Management
- High-volume, low-pressure cuffs are standard (pressure <25 mmHg / <34 cmH2O)
- High cuff pressures impair mucosal blood flow → pressure necrosis → tracheal stenosis
- Cuff pressure should be checked with a manometer regularly
- Minimal occlusive volume technique: inflate until no air leak, then check pressure
Tube Sizing (Common Sizes)
| Shiley Jackson Size | Inner Diameter (mm) | Outer Diameter (mm) | Length (mm) |
|---|---|---|---|
| 4 | 5.0 | 9.4 | 62 |
| 6 | 6.4 | 10.8 | 74 |
| 8 | 7.6 | 12.2 | 79 |
| 10 | 8.9 | 13.8 | 79 |
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, p.211
7. Timing of Tracheostomy in ICU Patients
This remains controversial:
- Early tracheostomy (≤7 days or even ≤4 days) vs. late tracheostomy (>10-14 days)
- Most large studies (including the TracMan trial, UK, 900+ patients across 72 ICUs) found:
- No difference in 30-day or 2-year mortality
- No difference in pneumonia rates, ICU length of stay, or antibiotic use
- Over 50% of patients randomized to late tracheostomy did not require it at all (liberated from ventilation before the procedure was needed)
- One randomized trial (medical ICU) found early tracheostomy at 48h vs 14-16 days significantly reduced mortality (32% vs 62%), pneumonia (5% vs 25%), and ICU stay - but this is not consistently replicated
- Practical takeaway: Consider tracheostomy when expected MV duration >14 days. When risk of extubation failure resulting in death >1:1000, proceed with tracheostomy.
Source: Sabiston Textbook of Surgery; Scott-Brown's Otorhinolaryngology
8. The PDT Procedure - Step by Step
- Preprocedure: Review history, respiratory status, neck anatomy. Review imaging for high-riding innominate artery or aberrant vessels. Ultrasound of neck to mark vessels.
- Labs: Platelet count, PT/PTT, BUN
- Team: Proceduralist (bedside), anesthesiologist/airway-trained physician at head of bed, nurse
- Positioning: Shoulder roll to extend the neck
- Prep: FiO2 increased to 1.0, sterile field, local anesthetic (1.5% lidocaine with epinephrine) infiltrated
- Identify landmarks: Thyroid cartilage → cricoid cartilage → 1st, 2nd, 3rd tracheal rings
- Bronchoscopy: Scope positioned at distal end of ETT; ETT withdrawn to just above ideal entry point under bronchoscopic visualization
- Needle insertion: 1-1.5 cm horizontal/vertical incision, blunt dissection to tracheal rings, needle inserted between rings 1-2 or 2-3 with bronchoscopic transillumination confirmation
- Guidewire placement: Through needle into tracheal lumen
- Dilation: Serial dilators or single-step Ciaglia Blue Rhino dilator advanced over wire
- Tube insertion: Tracheostomy tube advanced over dilator/wire; dilator removed
- Confirmation: CO2 detection, capnography (class I AHA recommendation), equal chest rise, bilateral breath sounds, bronchoscopic visualization of tracheal rings
- Secure: Tracheostomy ties, sutures to neck plate
Source: Current Surgical Therapy 14e, p.1593
9. Complications
Classified by Timing
| Timing | Complication |
|---|---|
| Immediate (intraoperative) | Hemorrhage (anterior jugular veins, thyroid isthmus), false tract / extraluminal placement, posterior tracheal wall injury / esophageal perforation, loss of airway, failure of procedure, subcutaneous emphysema, pneumothorax, pneumomediastinum, cardiac arrest |
| Early (days-weeks) | Hemorrhage, tube displacement/dislodgement, pneumothorax, wound infection, tube obstruction (mucus plugging), subcutaneous emphysema |
| Late (weeks-months) | Tracheal stenosis, granulation tissue formation, tracheomalacia, tracheoesophageal (TE) fistula, tracheo-innominate artery fistula, stoma infection, persistent stoma, dysphagia |
Source: Mulholland and Greenfield's Surgery 7e; Roberts and Hedges'
Key Complications in Detail
Tracheal Stenosis
- Most common late complication
- Mechanism: high cuff pressure → mucosal ischemia → necrosis → loss of cartilage → fibrous narrowing
- Prevention: low-pressure cuffs (keep <25 mmHg), regular cuff pressure monitoring
- Treatment: bronchoscopy + dilation; if severe, tracheal resection and reconstruction
Tracheo-Innominate Artery (TI) Fistula
- Life-threatening (reported mortality >80%)
- Mechanism: tube erodes into innominate artery, especially with tubes placed too low (below ring 3) or in patients with high-riding innominate artery
- Presentation: sentinel bleed (small herald hemorrhage) followed by massive hemorrhage
- Emergency management: overinflate cuff, digital pressure through stoma, immediate OR for vessel repair or ligation
Tracheoesophageal Fistula
- Mechanism: erosion of posterior tracheal wall (membranous portion) into esophagus, often by overinflated cuff or low-pressure high-volume cuff against rigid NG tube
- Features: food/fluid coming through tracheostomy, recurrent aspiration pneumonia, air in stomach on X-ray
- Treatment: surgical repair
Tube Obstruction
- Most common complication in the ED (30% of respiratory ED visits)
- Causes: dried secretions (most common), blood, aspirated material, granulation tissue, cuff herniation
- Management: remove and clean inner cannula first; if not improved, attempt suctioning; if still obstructed, change outer cannula
Tube Dislodgement
- Occurs most often in early post-op period (before tract maturation ~4-5 days)
- Emergency: if <72h post-op, do NOT blindly attempt re-insertion; cover stoma, bag-mask via mouth, call for surgical backup
- If tract mature: can re-insert with obturator using neck extended, then confirm with capnography
10. Tracheostomy Tube Change
First change timing: Usually 5-7 days post-op (once tract mature) or per manufacturer recommendation (~30 days for routine change)
Equipment needed:
- Tracheostomy tube of same size (and one size smaller as backup)
- Cuff syringe, suction, oxygen source, Ambu bag
- Lubricating jelly, forceps
- Capnography if available
Procedure:
- Preoxygenate with 100% O2
- Suction trachea and oropharynx
- Deflate cuff (if cuffed)
- Remove old tube while patient breathes normally
- Insert new tube with obturator in place at 90° angle, sweep downward
- Remove obturator, insert inner cannula, inflate cuff
- Confirm placement: capnography, chest auscultation, direct visualization
For difficult tract or high-risk patient: Advance over a guide catheter (e.g., red rubber suction catheter) as a Seldinger-style guide (see figure 7.8 technique in Roberts & Hedges).
11. Post-Operative & Ongoing Care
Routine Care
- Suctioning: As needed (not on a fixed schedule); use appropriate catheter size (no larger than 1/2 the inner diameter of the tube); suction during withdrawal not insertion
- Inner cannula cleaning: Every 8 hours (or replace if disposable); prevents obstruction from dried secretions
- Stoma care: Clean with normal saline/water, change tracheostomy dressings daily; keep skin dry to prevent breakdown
- Humidification: Bypass of upper airway humidification requires external humidification (heated humidifier or HME filter) to prevent mucus plugging
- Cuff pressure monitoring: Check every 8-12 hours; maintain 20-25 mmHg (25-30 cmH2O)
- Tracheostomy ties/holder: Change daily; always keep one finger width between ties and neck
Nursing Assessment
- Assess breathing pattern, RR, SpO2, work of breathing
- Listen for upper airway sounds (stridor = possible obstruction or dislodged tube)
- Observe stoma site for infection, granulation tissue, skin breakdown
- Assess secretion character (amount, color, consistency) - purulent secretions suggest infection
- Always keep a spare tube (same size + one size smaller) and obturator at bedside
Communication
- Cuffed tube prevents speech (air does not pass through cords)
- Strategies: fenestrated tube (cuff deflated), speaking valve (Passy-Muir valve), writing, communication boards, electronic devices
- Passy-Muir Valve (PMV): One-way valve placed on tracheostomy hub; allows inspiration through tube but forces expiration up through cords → enables voice; requires cuff to be fully deflated when using PMV
Swallowing Assessment
- Aspiration risk is elevated with tracheostomy (altered laryngeal elevation, sensory changes)
- Bedside swallowing assessment, modified barium swallow, or FEES (flexible endoscopic evaluation of swallowing) recommended before oral feeding
12. Decannulation (Weaning from Tracheostomy)
Decannulation = removal of the tracheostomy tube once the indication has resolved.
Prerequisites for decannulation:
- Underlying cause resolved
- Adequate spontaneous ventilation (weaned from mechanical ventilation)
- Adequate cough and airway protection
- Secretion load manageable
- Patent upper airway (confirmed endoscopically)
- No significant aspiration
Weaning steps:
- Downsize the tube progressively
- Trial of capping (placing a cap over the tube opening) - patient breathes entirely around the tube
- Deflate cuff during waking hours, then 24 hours
- If patient tolerates capping for 24 hours without distress → decannulate
- Tracheal buttons (Montgomery button): maintain stoma patency during weaning in patients who need periodic suctioning but do not need mechanical ventilation; can be retained permanently if decannulation fails
Post-decannulation: Stoma usually closes spontaneously within days-weeks. Cover with occlusive dressing; patient instructed to press over stoma when speaking/coughing.
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Mulholland's Surgery
13. Special Situations
COVID-19 and Tracheostomy
- PDT is an aerosol-generating procedure requiring airborne + droplet precautions
- Evidence supports waiting 10-14 days of mechanical ventilation before tracheostomy in COVID-19 patients (associated with lower duration of MV and ICU stay without increased mortality)
- Tracheostomy on ECMO is feasible; complications higher (mainly bleeding) but no difference between PDT and OST
Pediatric Tracheostomy
- Softer cartilage, smaller anatomy - more technically demanding
- Highest risk period is the first weeks (accidental dislodgement before tract maturation)
- Staying sutures placed around tracheal rings to facilitate emergency re-insertion
- More common long-term complications: tracheal growth disturbance, suprastomal collapse
Obese Patients
- PDT may be done safely but requires appropriate (extended-length) kit
- Surgical approach may be preferred for class III obesity
- Ultrasound assessment of neck anatomy essential before PDT
14. Emergency Management of Tracheostomy Complications
Blocked Tube (Obstruction)
- Remove and inspect inner cannula → clean/replace
- Pass suction catheter → clear secretions
- If still obstructed → change the tube
- If unable to re-intubate stoma → oral intubation
Dislodged Tube
- Immature tract (<5 days): Do not blindly re-insert. Apply O2 to stoma, ventilate via mouth/nose, urgent surgical assistance
- Mature tract (>5 days): Replace with obturator in place; extend neck; confirm placement; if resistance, downsize the tube
Hemorrhage
- Minor: Usually from granulation tissue; direct pressure, silver nitrate cautery
- Massive (sentinel bleed scenario): Suspect TI fistula. Overinflate cuff; apply digital pressure through stoma anteriorly; immediate OR
Summary Table: Key Facts at a Glance
| Parameter | Value/Detail |
|---|---|
| Most common ICU procedure | Yes (for prolonged MV) |
| Ideal stoma site | Between tracheal rings 2-3 |
| PDT mortality risk | <0.1-0.2% |
| PDT major complication rate | ~0.15% |
| Early complication rate | 16-20% |
| Late complication rate | 6-8% |
| Cuff pressure target | <25 mmHg (20-25 mmHg) |
| First routine tube change | ~5-7 days (mature tract) |
| Manufacturer tube change interval | ~30 days |
| Tract maturation | ~4-5 days post-op |
Sources: Sabiston Textbook of Surgery; Current Surgical Therapy 14e; Scott-Brown's Otorhinolaryngology (Vol 1 & 2); Mulholland and Greenfield's Surgery 7e; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.