EINC & NB Assesment Lec Clinics .. teach me this very clearly according to Nelson pediatrics.. make me to understand throughly about this topic step by step with images needed everything
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
newborn APGAR score assessment table
Reading File
Searching Images
Ballard score gestational age newborn neuromuscular physical maturity
Searching the Web
EINC Essential Intrapartum Newborn Care protocol Philippines WHO steps
Reading Web Page
EINC four core steps essential newborn care immediate drying skin to skin cord clamping breastfeeding
Searching Images
newborn physical examination head-to-toe neonatal reflexes Moro grasp rooting
Loading Image
Loading Image
Loading Image
Reading File
🍼 EINC & Newborn Assessment — Complete Lecture Notes
Based on Nelson Pediatrics & EINC/Unang Yakap Protocol
🔷 PART 1 — WHAT IS EINC?
EINC = Essential Intrapartum and Newborn Care (also called "Unang Yakap" in the Philippines)
This is a WHO-backed, evidence-based protocol adopted by the Philippine DOH (Admin Order 2009-0025) to reduce neonatal mortality. It emphasizes a time-bound sequence of actions in the immediate post-birth period.
📌 Key Concept: 82,000 Filipino children die annually — most could have been prevented. The Philippines is among the 42 countries accounting for 90% of global under-five mortality.
🔷 PART 2 — EINC: THE FOUR CORE STEPS ("Unang Yakap")
These 4 steps must be performed in sequence immediately after birth for every stable newborn.
STEP 1 — Immediate and Thorough Drying ⏱️ First 30 seconds
Why?
- Newborns lose heat rapidly (evaporation, radiation, conduction, convection)
- Hypothermia leads to increased oxygen consumption, hypoglycemia, acidosis, and death
How to do it:
- Dry the baby vigorously with a clean, warm, dry cloth
- Stimulates breathing by tactile stimulation
- Remove wet cloth and replace with a dry one immediately
- Keep the baby on the mother's abdomen (do not transfer to a cold surface)
- Room temperature must be 25–28°C, no drafts
⚠️ Do NOT do routine suctioning for a vigorous newborn with clear amniotic fluid — this is harmful and unnecessary.
STEP 2 — Skin-to-Skin Contact (SSC) 👩👧
When: Immediately after drying, before cord clamping in some protocols; at minimum within the first few minutes
How:
- Place baby prone on mother's chest (between the breasts), skin-to-skin
- Cover with a dry cloth (keep warm)
- SSC should last at least 90 minutes (ideally until after the first feed)
Why? (Physiological Benefits):
| Benefit | Mechanism |
|---|---|
| 🌡️ Thermoregulation | Mother's chest acts as a "biological incubator" — her skin temperature adapts to baby's need |
| 🍼 Breastfeeding | Triggers oxytocin, prolactin; baby self-attaches to nipple |
| 🧠 Brain development | Reduces cortisol; promotes bonding |
| 🛡️ Immunity | Transfer of maternal skin flora; reduces infection |
| ❤️ Cardiorespiratory stability | Improves O₂ saturation, reduces apnea |
STEP 3 — Properly Timed Cord Clamping ⏱️ 1–3 minutes after birth
Rule: Clamp the cord only after pulsations stop OR 1–3 minutes after birth — whichever is earlier.
Why delay cord clamping?
- Blood flow continues from placenta → baby for 1–3 minutes
- Baby receives 80–100 mL extra blood = ~30–35 mg/kg extra iron
- Prevents iron-deficiency anemia in the first year
- Improves hemoglobin, ferritin, and neurodevelopmental outcomes
⚠️ Do NOT clamp immediately — this deprives the baby of ~one-third of its blood volume!
⚠️ Do NOT do dry cord care with antiseptics (alcohol, povidone iodine) — dry cord care alone is recommended.
STEP 4 — Non-Separation of Mother and Baby for Early Breastfeeding 🤱
Goal: Baby should self-attach and latch within the first 90 minutes
The "Breast Crawl" Phenomenon:
- When placed skin-to-skin, the newborn will instinctively move toward the breast using smell and rooting reflex
- Allow this natural process — do NOT rush or forcefully latch
Why exclusive breastfeeding?
- Colostrum = "liquid gold" — rich in IgA, leukocytes, growth factors
- Reduces diarrhea, pneumonia, necrotizing enterocolitis (NEC)
- Protects against SIDS, allergies, obesity
⚠️ Harmful practices to AVOID:
- Prelacteals (glucose water, formula) — interfere with breastfeeding
- Early bathing — removes vernix, causes hypothermia
- Footprinting — unnecessary
- Routine suctioning of mouth/nares in vigorous newborn
- Immediate cord clamping
- Use of "bigkis" (abdominal binders)
🔷 PART 3 — EINC CHECKLIST (Timed Sequence)
| Time Period | Key Actions |
|---|---|
| Before delivery | Warm room (25–28°C), eliminate drafts, prepare clean dry towels, check resuscitation equipment |
| At delivery (0–30 sec) | Immediate thorough drying, remove wet cloth |
| 0–3 min | Skin-to-skin contact, cord clamping 1–3 min |
| 0–90 min | Non-separation, facilitate breastfeeding |
| Within 1–4 hrs | Eye prophylaxis (erythromycin ointment), Vitamin K IM |
| Within 6 hrs | Newborn physical examination, anthropometrics, weight |
| After 6 hrs | Bathing (optional), Hepatitis B vaccine, BCG vaccine |
🔷 PART 4 — NEWBORN ASSESSMENT (NB Assessment)
(Nelson Pediatrics, Chapter 18, Section III)
A. VITAL SIGNS & BIRTH WEIGHT
| Parameter | Normal Range |
|---|---|
| Heart Rate | 100–160 bpm |
| Respiratory Rate | 30–60 breaths/min |
| Temperature | 36.5–37.5°C (axillary) |
| Blood Pressure | Related to gestational age and birth weight |
| SpO₂ (target) | ≥94% after stabilization |
Birth Weight Categories (Nelson Pediatrics, p.644):
| Category | Weight |
|---|---|
| Extremely Low Birth Weight (ELBW) | < 1000 g |
| Very Low Birth Weight (VLBW) | < 1500 g |
| Low Birth Weight (LBW) | < 2500 g |
| Normal | 2500–4000 g |
| Small for Gestational Age (SGA) | < 10th percentile for GA |
| Large for Gestational Age (LGA) | > 90th percentile for GA |
| Appropriate for Gestational Age (AGA) | 10th–90th percentile |
B. APGAR SCORE
(Assessed at 1 minute and 5 minutes; repeat every 5 minutes if score <7)
Dr. Virginia Apgar introduced this scoring system in 1953.

| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (Color) | Blue/pale all over | Acrocyanosis (pink body, blue extremities) | Completely pink |
| Pulse (Heart Rate) | Absent | < 100 bpm | > 100 bpm |
| Grimace (Reflex Irritability) | No response | Grimace | Cough or sneeze |
| Activity (Muscle Tone) | Limp | Some flexion of extremities | Active motion |
| Respiration | Absent/irregular | Slow, weak cry | Good, strong cry |
Memory Aid: Appearance • Pulse • Grimace • Activity • Respiration = APGAR
Score Interpretation:
| Score | Interpretation | Action |
|---|---|---|
| 7–10 | Normal | Routine care |
| 4–6 | Moderate depression | Stimulate, supplemental O₂, reassess |
| 0–3 | Severe depression | Begin resuscitation immediately |
📌 Clinical Pearl: The APGAR score is a snapshot, NOT a predictor of long-term outcome. It helps guide immediate resuscitation decisions. A low 1-minute score alone does not indicate brain damage.
C. GESTATIONAL AGE ESTIMATION — NEW BALLARD SCORE
(Nelson Pediatrics, p. 644–645, eFig. 18.1)
When to use: When obstetric dating (ultrasound or LMP) is not available
Best time: Most accurate at ~24 hours of life
The Ballard Score has two components:
Part 1: Neuromuscular Maturity (6 signs, each scored –1 to 5)
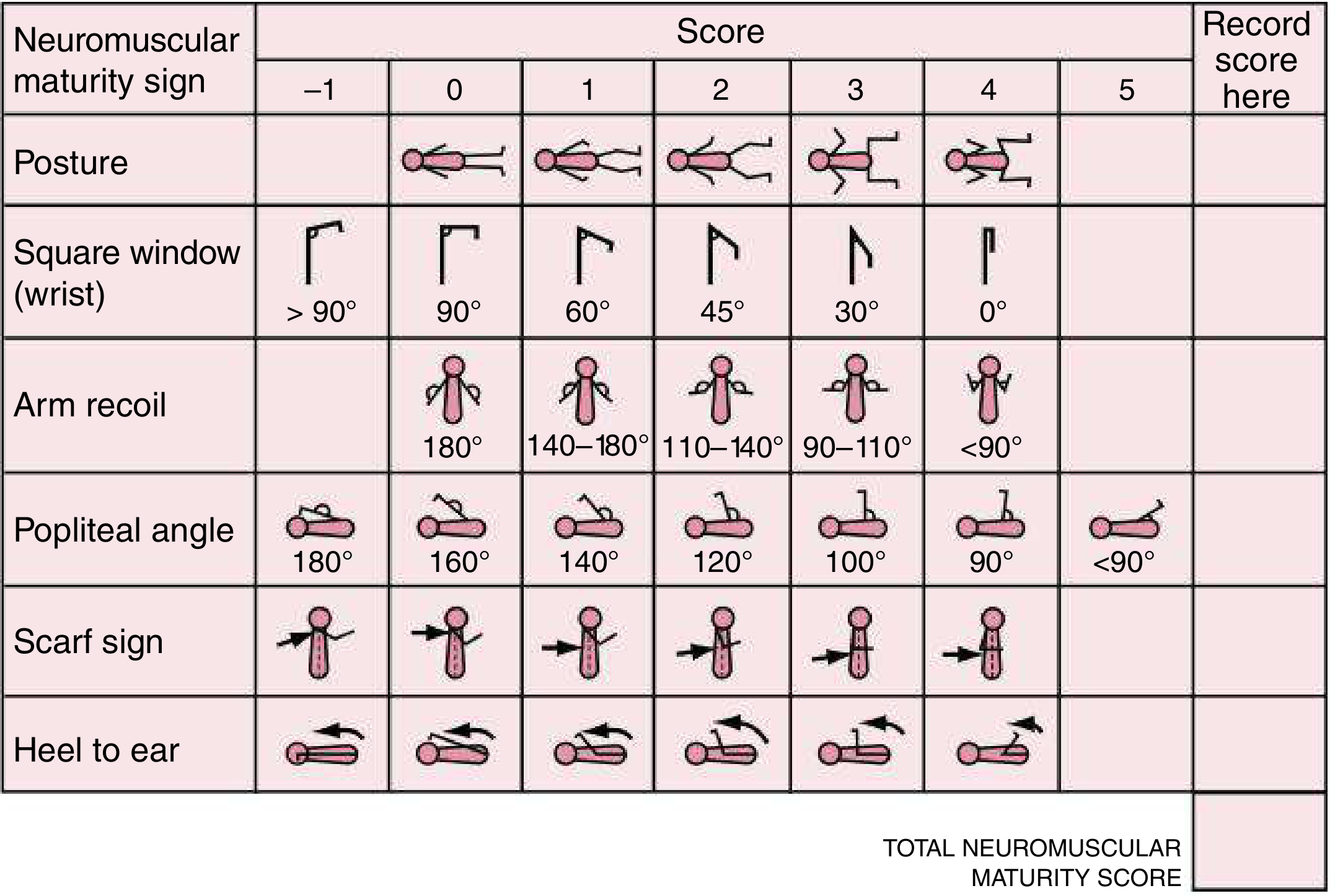
| Sign | How to Assess | Immature (premature) | Mature (term) |
|---|---|---|---|
| 1. Posture | Observe quiet, supine infant | Arms & legs extended (score 0) | Full flexion (score 4) |
| 2. Square Window | Flex wrist fully; measure wrist–forearm angle | >90° (score 0) | 0° (score 4) |
| 3. Arm Recoil | Flex for 5 sec → extend → release; measure recoil angle | 180° (no recoil, score 0) | <90° (brisk recoil, score 4) |
| 4. Popliteal Angle | Thigh to chest, extend leg; measure popliteal angle | 180° (score 0) | <90° (score 5) |
| 5. Scarf Sign | Pull hand across neck toward opposite shoulder | Elbow crosses midline (score 0) | Elbow cannot reach midline (score 3) |
| 6. Heel to Ear | Bring heel toward ear; observe resistance | Heel reaches ear easily (score 0) | Strong resistance (score 4) |
Part 2: Physical Maturity (6 signs, each scored –1 to 5)
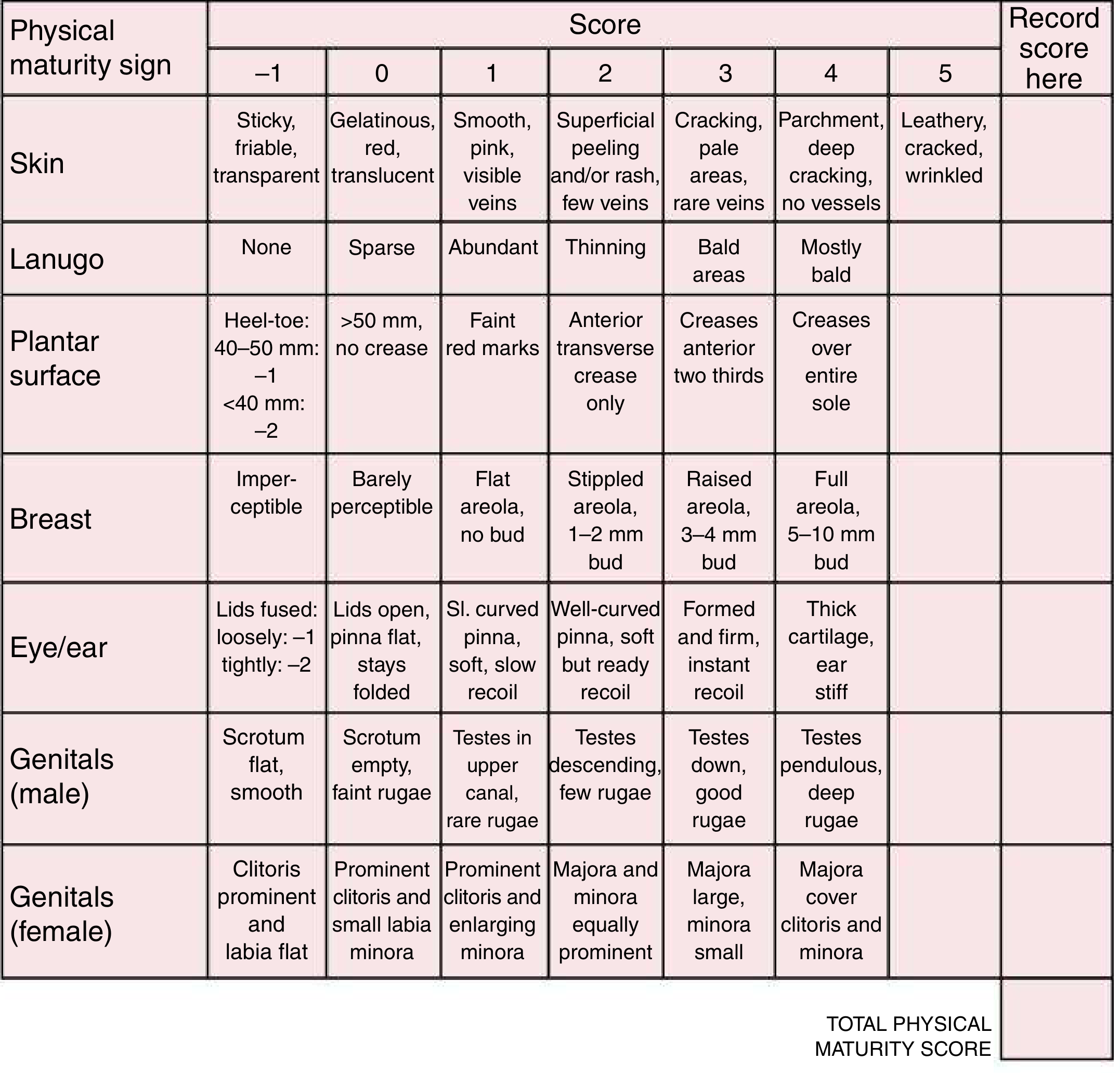
| Sign | Immature (preterm) | Term (mature) |
|---|---|---|
| Skin | Sticky, friable, transparent (score –1) → Gelatinous, red (score 0) | Leathery, cracked, wrinkled (score 5) |
| Lanugo | None (–1) → Sparse (0) → Abundant (1) | Mostly bald (4) |
| Plantar surface | Heel–toe < 40 mm (score –2) | Creases over entire sole (score 4) |
| Breast | Imperceptible (–1) | Full areola, 5–10 mm bud (score 5) |
| Eye/Ear | Lids fused tightly (–2) → Lids open, pinna flat (0) | Thick cartilage, ear stiff (score 4) |
| Genitals (Male) | Scrotum flat, smooth (–1) | Testes pendulous, deep rugae (score 5) |
| Genitals (Female) | Clitoris prominent, labia flat (–1) | Majora cover clitoris and minora (score 4) |
Scoring to Gestational Age Conversion:

| Total Score | Gestational Age |
|---|---|
| –10 | 20 weeks |
| –5 | 22 weeks |
| 0 | 24 weeks |
| 5 | 26 weeks |
| 10 | 28 weeks |
| 15 | 30 weeks |
| 20 | 32 weeks |
| 25 | 34 weeks |
| 30 | 36 weeks |
| 35 | 38 weeks |
| 40 | 40 weeks (term) |
| 45 | 42 weeks |
| 50 | 44 weeks |
Gestational Age Classification:
| Classification | GA |
|---|---|
| Extremely preterm | < 28 weeks |
| Very preterm | 28–32 weeks |
| Moderate-to-late preterm | 32–37 weeks |
| Term | 37–42 weeks |
| Post-term | > 42 weeks |
D. BIRTH TRAUMA — Extracranial Fluid Collections
(Nelson Pediatrics, Table 18.3 & Fig. 18.3)
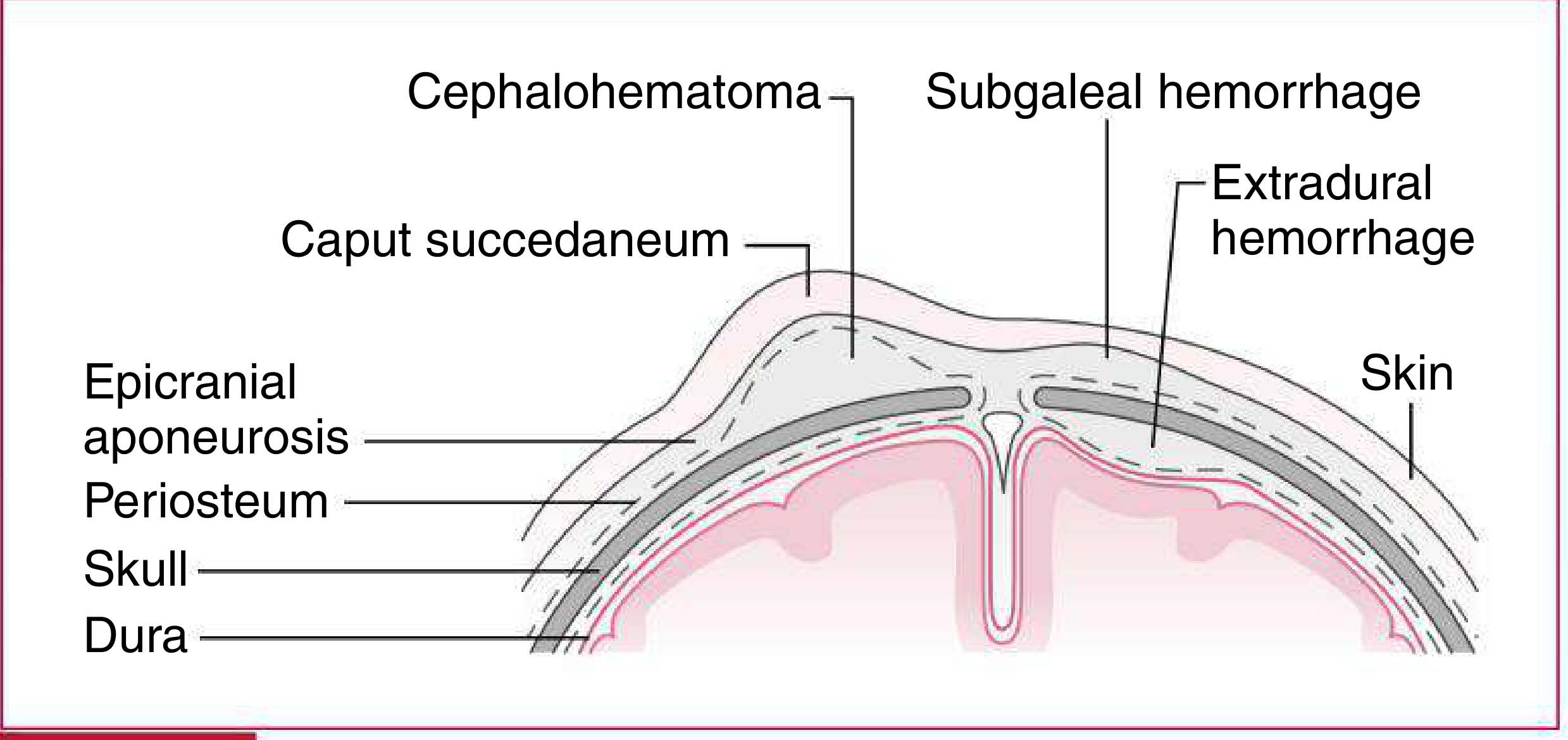
| Feature | Caput Succedaneum | Cephalohematoma | Subgaleal Hemorrhage |
|---|---|---|---|
| Location | At contact point; crosses sutures | Over parietal bones; does NOT cross sutures | Beneath epicranial aponeurosis; may extend to orbits or nape |
| Findings | Pitting edema, shifts with gravity, vague borders | Distinct firm margins; more fluctuant after 48 hr | Firm-to-fluctuant, ill-defined; crepitus or fluid waves |
| Timing | Maximal at birth; resolves in 48–72 hr | Increases 12–24 hr; resolves over weeks | Progressive; resolves over weeks |
| Severity | Minimal | Rarely severe | May be severe (especially with coagulopathy) ⚠️ |
🔑 Memory tip: Caput = "C" for Crosses sutures. Cephalo = "doesn't Cross." Subgaleal = most dangerous!
E. NEWBORN PHYSICAL EXAMINATION — Head to Toe
Perform within 6 hours of birth (EINC protocol).
1. General Appearance
- Posture, tone, cry, color, symmetry
- Normal: Flexed posture, vigorous cry, pink (may have acrocyanosis initially)
2. Head
- OFC (Occipitofrontal Circumference): Normal = 33–37 cm at term

- Fontanelles:
- Anterior (diamond-shaped): Closes at 9–18 months
- Posterior (triangular): Closes at 6–8 weeks
- Bulging = ↑ICP; Sunken = dehydration
- Cranial sutures: Check for premature fusion (craniosynostosis)
- Extracranial hemorrhages: See table above
3. Eyes
- Red reflex: Must be present bilaterally — absence suggests cataracts or retinoblastoma
- Check for subconjunctival hemorrhage (common, benign)
- Leukocoria = white reflex → refer urgently
4. Ears
- Check position: Low-set ears (below imaginary line through outer canthi) → associated with chromosomal syndromes

- Ear cartilage firmness used in Ballard scoring
5. Nose
- Obligate nasal breathers — check patency
- Choanal atresia: Cannot pass catheter through nostril
6. Mouth
- Epstein pearls = white keratin cysts on hard palate → normal, resolve spontaneously
- Ranula = retention cyst under tongue
- Check for cleft lip/palate
- Natal teeth (present at birth): remove if loose to prevent aspiration
7. Neck
- Check for masses: thyroglossal duct cyst (midline), branchial cleft cyst (lateral)
- Torticollis: Sternocleidomastoid (SCM) mass or spasm
8. Chest & Lungs
- Normal: Barrel-shaped, symmetric expansion
- Breath sounds: Clear bilaterally
- Gynecomastia in both sexes = normal (maternal estrogen effect)
- Accessory nipples (supernumerary) = benign variant
9. Heart
- Auscultate all 4 areas
- S1, S2 heard; split S2 normal
- Murmurs: Up to 50% of newborns have a transitional murmur (PDA closing)
- Pulse oximetry screening at 24–48 hr to detect critical CHD
10. Abdomen
- Liver normally palpable 2 cm below costal margin
- 3-vessel umbilical cord: 2 arteries + 1 vein — single umbilical artery associated with renal anomalies
- Omphalocele = abdominal contents herniate into umbilical base (covered by peritoneum)
- Gastroschisis = bowel herniates through abdominal wall defect to right of umbilicus (no covering)
11. Genitalia
Male:
- Testes should be descended bilaterally
- Hypospadias: Urethral meatus on ventral surface of penis
- Epispadias: Urethral meatus on dorsal surface
- Hydrocele: Transilluminates; usually resolves by 1 year
- Phimosis: Physiologic — foreskin non-retractile until 3–5 years old
Female:
- Vaginal discharge/spotting = normal (maternal estrogen withdrawal)
- Ambiguous genitalia → urgent evaluation (may be CAH)
12. Spine
- Check for dimples, tufts of hair, masses over spine → spina bifida occulta/meningocele
- Sacral dimple > 5 mm or > 2.5 cm from anal verge → ultrasound required
13. Extremities
- Polydactyly: Extra digits (autosomal dominant variant common in African descent)
- Syndactyly: Fused digits
- Check for congenital hip dysplasia (DDH):
- Ortolani test: Gentle abduction — clunk = dislocated hip reducing ✅
- Barlow test: Adduction with posterior pressure — clunk = dislocatable hip ✅
14. Neurological Examination — Primitive Reflexes
| Reflex | How to Elicit | Normal Response | Disappears by |
|---|---|---|---|
| Moro (Startle) | Sudden extension/drop of head | Arms abduct, extend, then flex and adduct ("embrace") | 3–6 months |
| Rooting | Stroke corner of mouth | Turns head toward stimulus, opens mouth | 3–4 months |
| Sucking | Place object in mouth | Rhythmic sucking | 3–4 months |
| Palmar Grasp | Place finger in palm | Baby grasps firmly | 3–6 months |
| Plantar Grasp | Press thumb on plantar surface | Plantar flexion of toes | 8–15 months |
| Babinski | Stroke lateral sole | Dorsiflexion of great toe + fanning of others | 12–24 months |
| Stepping/Walking | Hold upright, soles touch surface | Alternating stepping movements | 2–3 months |
| Tonic Neck (ATNR) | Turn head to one side | "Fencing posture" — extension of limbs on face side, flexion on skull side | 4–6 months |

📌 Absence of primitive reflexes = neurological depression. Persistence beyond expected age = neurological abnormality.
🔷 PART 5 — IMPORTANT CONGENITAL ASSOCIATIONS TO KNOW
(Nelson Pediatrics, Chapter 18)
| Syndrome | Mnemonic | Key Features |
|---|---|---|
| VACTERL | Vertebral, Anal atresia, Cardiac, TracheoEsophageal fistula, Renal, Limb | Multiple organ systems; no tracheo-esophageal fistula without VACTERL workup |
| CHARGE | Coloboma, Heart disease, choanal Atresia, Retarded growth, Genital anomalies, Ear abnormalities | Caused by CHD7 mutation |
| IDM (Infant of Diabetic Mother) | — | Hypoglycemia, polycythemia, TTN, sacral agenesis, cardiac defects, cardiomegaly |
🔷 PART 6 — ROUTINE NEWBORN PROCEDURES (EINC Timed Sequence)
| Procedure | Timing | Purpose |
|---|---|---|
| Eye Prophylaxis (erythromycin 0.5% ointment) | Within 1–4 hours | Prevent ophthalmia neonatorum (GC, Chlamydia) |
| Vitamin K₁ (phytonadione) IM | Within 1–4 hours | Prevent Hemorrhagic Disease of Newborn (HDN/VKDB) |
| Hepatitis B Vaccine | Within 12–24 hours (birth dose) | Prevent perinatal HBV transmission |
| BCG Vaccine | Within 24 hours | Prevent TB meningitis and miliary TB |
| Newborn Screening | 48–72 hours | Screen for congenital hypothyroidism, PKU, G6PD, galactosemia, CAH, etc. |
| Hearing Screening (OAE/AABR) | Before discharge | Detect sensorineural hearing loss |
| Critical CHD Pulse Oximetry | 24–48 hours | Detect CCHD (duct-dependent lesions) |
🔷 PART 7 — CLINICAL REVIEW: "WHAT TO DO" vs. "WHAT NOT TO DO"
✅ DO:
- Dry immediately and thoroughly
- Skin-to-skin for 90+ minutes
- Clamp cord at 1–3 min
- Facilitate breast crawl and latching
- Give Vitamin K within 1–4 hr
- Perform complete head-to-toe exam within 6 hr
❌ DO NOT:
| Harmful Practice | Why It's Harmful |
|---|---|
| Routine oropharyngeal suctioning (vigorous baby) | Causes apnea, bradycardia, mucosal injury |
| Immediate cord clamping | Deprives baby of iron-rich blood |
| Early bathing (<6 hrs) | Hypothermia, removes vernix protection |
| Prelacteals (glucose water, formula) | Disrupts breastfeeding, unnecessary |
| Cord care with antiseptics | Delays cord separation, damages tissue |
| Use of "bigkis" (belly binders) | Compresses abdominal organs |
| Footprinting | Unnecessary, no clinical benefit |
🔷 QUICK REFERENCE SUMMARY TABLE
| Topic | Key Points |
|---|---|
| EINC 4 Core Steps | Dry → SSC → Cord clamp (1–3 min) → Don't separate |
| APGAR | 1 & 5 min; 7–10 normal; 4–6 moderate; 0–3 severe |
| APGAR letters | A-P-G-A-R = Appearance, Pulse, Grimace, Activity, Respiration |
| Ballard Score | Neuromuscular (6) + Physical (6) signs; most accurate at 24 hr |
| Total Ballard score 40 | = 40 weeks' gestation (term) |
| Caput vs Cephalo | Caput crosses sutures; Cephalo does NOT |
| Dangerous head bleed | Subgaleal hemorrhage — can be life-threatening |
| Cord vessels | 2 arteries + 1 vein; single artery → check kidneys |
| DDH tests | Ortolani (reduce) + Barlow (dislocate) |
| Moro disappears | 3–6 months; absence = neurological problem |
| Routine Vit K | IM, within 1–4 hr — prevents VKDB/HDN |
Sources:
- Nelson Pediatrics Formulary (2023), Chapter 18 — Neonatology, pp. 643–649
- EINC/Unang Yakap Protocol, Philippine DOH Administrative Order 2009-0025 / PhilHealth EINC Checklist (revised 2022)
- PAFP EINC Module — Four Core Steps
This is a shared conversation. Sign in to Orris to start your own chat.