What Hemopoiesis define it
Reading File
Finding Sources
Searching the Web
hemopoiesis definition medical
Reading File
Reading File
Reading File
Loading Image
Hemopoiesis (Hematopoiesis)
Hemopoiesis (also spelled hematopoiesis) is the continuous biological process by which all formed elements of the blood — red blood cells, white blood cells, and platelets — are produced, developed, and maintained throughout life.
Definition
Hemopoiesis is the process of blood cell formation arising from hematopoietic stem cells (HSCs) — pluripotent, self-renewing cells that sit at the apex of a hierarchy of bone marrow progenitors. A single HSC can generate every type of mature blood cell (pluripotency), while ensuring that at least one daughter cell is retained as a stem cell (self-renewal).
"All formed elements of blood — red cells, granulocytes, monocytes, platelets, and lymphocytes — have a common origin from HSCs, pluripotent cells that sit at the apex of a hierarchy of bone marrow progenitors." — Robbins, Cotran & Kumar: Pathologic Basis of Disease
Sites of Hemopoiesis Through Life
| Stage | Primary Site |
|---|---|
| 3rd week of embryo | Yolk sac (transient, mainly embryonic RBCs) |
| 3rd month of embryo | Liver (chief site until near birth) |
| Fetal period | Spleen and placenta |
| 4th month onward | Bone marrow (definitive) |
| After puberty | Axial skeleton only (vertebrae, sternum, ribs, pelvis) |
| Normal adult | ~50% of marrow space hematopoietically active |
Cell Hierarchy
The diagram below shows the full differentiation pathway from HSC to all mature blood cells:
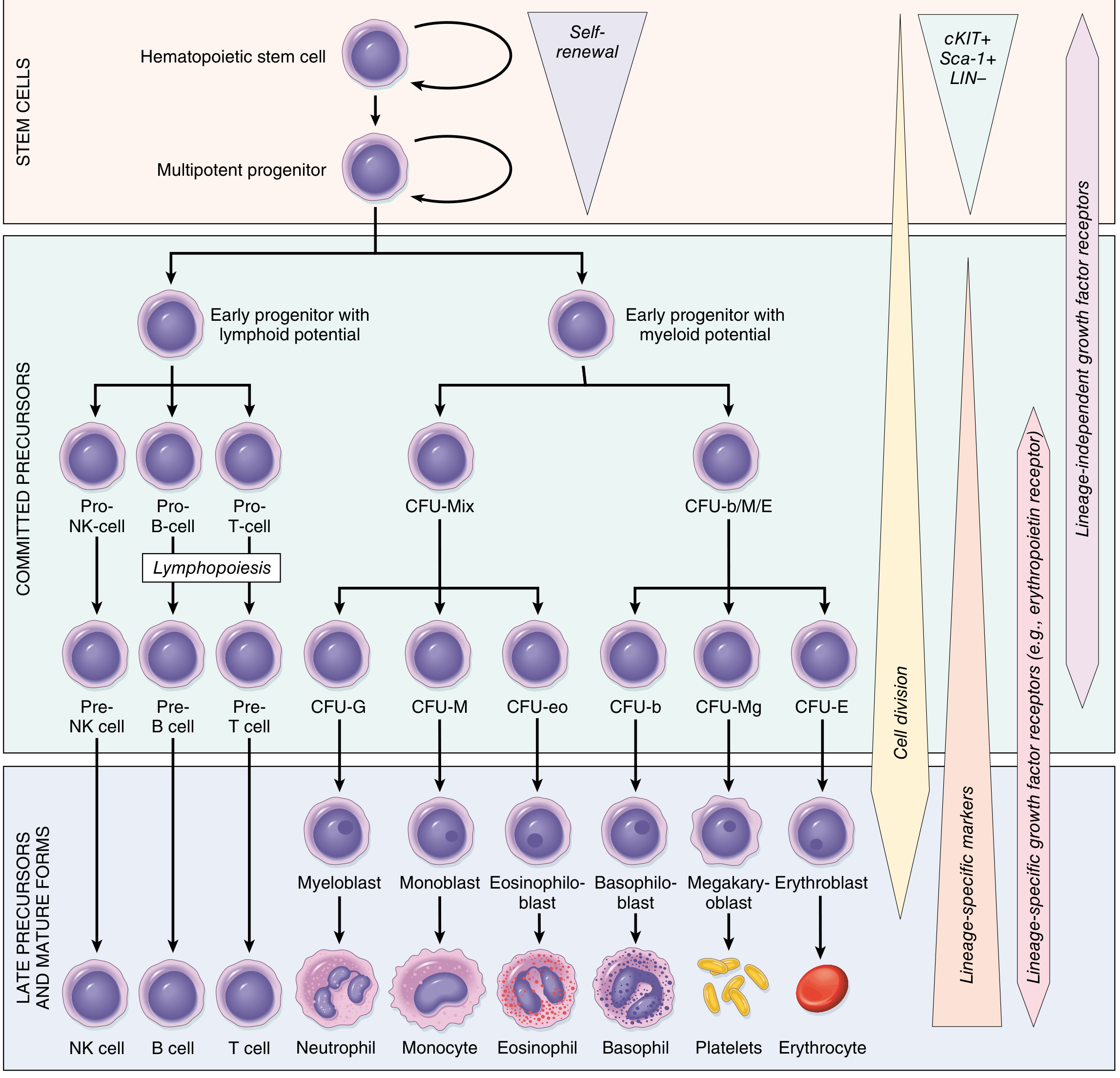
The HSC differentiates through two major lineages:
- Lymphoid lineage → B cells, T cells, NK cells
- Myeloid lineage → Neutrophils, Monocytes, Eosinophils, Basophils, Megakaryocytes (→Platelets), Erythrocytes
Each step involves progressively committed progenitors called colony-forming units (CFUs) (e.g., CFU-G for granulocytes, CFU-E for erythrocytes), ultimately producing morphologically recognizable precursors (myeloblasts, proerythroblasts, megakaryoblasts).
Regulation of Hemopoiesis
Hemopoiesis is tightly regulated by cytokines and growth factors produced in the bone marrow microenvironment:
| Factor | Source | Target |
|---|---|---|
| Erythropoietin (EPO) | Kidney, Liver | Erythroid progenitors |
| Thrombopoietin (TPO) | Liver, Kidney | Megakaryocyte progenitors |
| GM-CSF | T cells, endothelial cells | Multiple myeloid progenitors |
| G-CSF | Endothelial cells, monocytes | Granulocyte progenitors |
| M-CSF | Macrophages, endothelial cells | Monocyte/macrophage progenitors |
| IL-3 | T lymphocytes | Most progenitor cells |
These factors bind receptors on progenitor cells, activating transcription factors that drive gene expression along specific differentiation pathways.
Two Essential Properties of HSCs
- Pluripotency — ability to generate all mature blood cell types
- Self-renewal — at least one daughter cell must remain a stem cell to prevent HSC depletion
The normal adult marrow contains an estimated 50,000–200,000 HSCs, responsible for maintaining blood cell production throughout life.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Histology: A Text and Atlas (Mescher); Goodman & Gilman's Pharmacological Basis of Therapeutics
Explain the specific growth factors that regulate erythropoiesis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive explanation of the specific growth factors that regulate erythropoiesis, drawn from authoritative textbooks.
Growth Factors Regulating Erythropoiesis
Erythropoiesis is regulated by a hierarchy of growth factors acting at different stages — from the pluripotent stem cell down to the mature red blood cell. These can be divided into early-acting (multilineage) factors and late-acting (lineage-specific) factors.
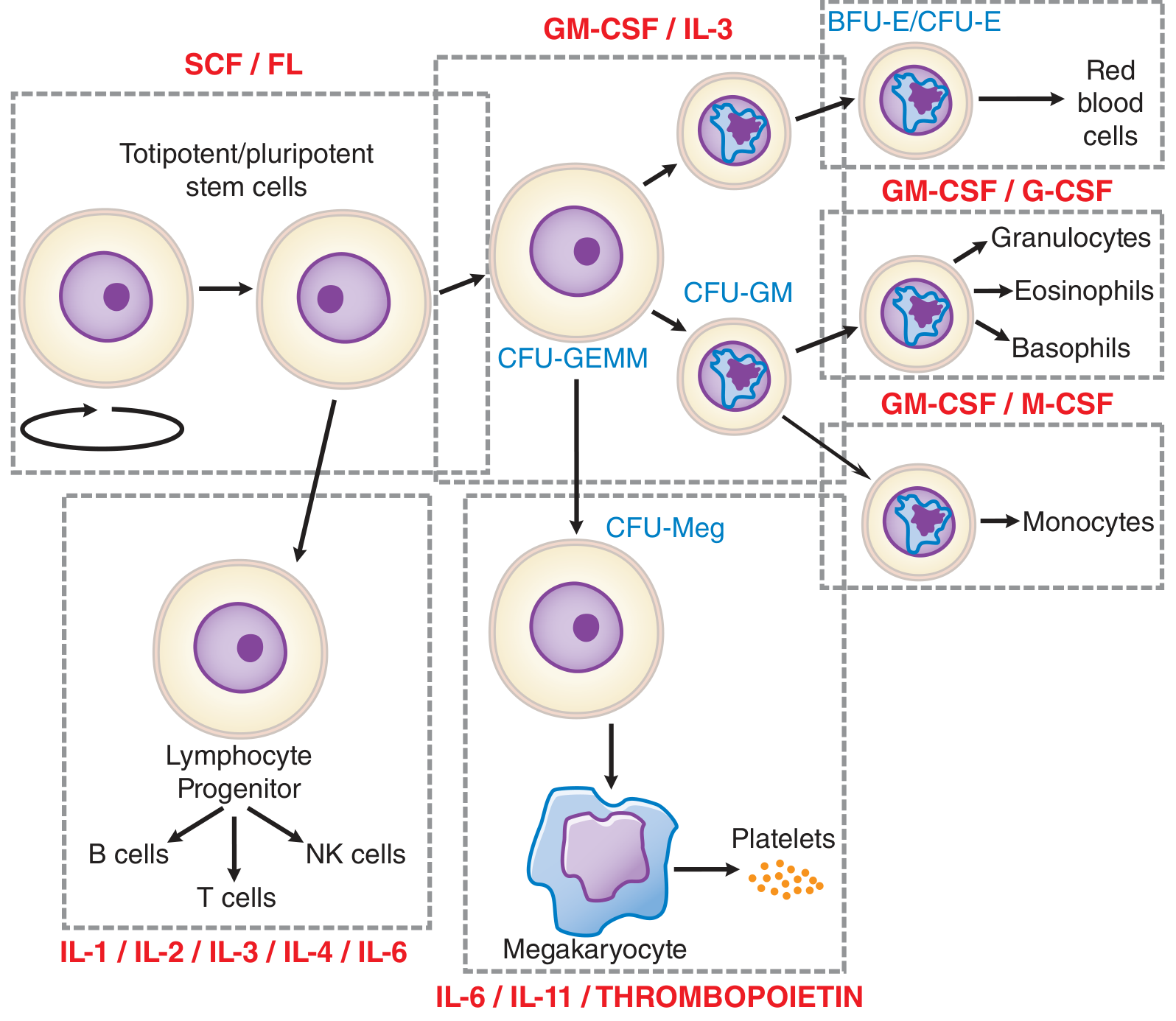
Stage 1 — Early / Multilineage Factors (act on stem cells and early progenitors)
These factors stimulate stem cells to form early progenitor pools including BFU-E (burst-forming unit–erythroid), the earliest committed erythroid progenitor.
1. Stem Cell Factor (SCF) / c-Kit Ligand
- Acts as a mitogen for all hematopoietic progenitor cells, including the earliest erythroid progenitors (BFU-E)
- Produced by stromal cells of the bone marrow
- Works synergistically with EPO to expand the erythroid progenitor pool
- Binds the c-Kit receptor on stem cells
2. FLT3 Ligand (FL)
- Works alongside SCF at the stem cell level
- Promotes survival and expansion of multipotent progenitors before lineage commitment
- Acts on CFU-GEMM (mixed myeloid progenitors that include erythroid potential)
3. Interleukin-3 (IL-3)
- A broad-acting cytokine produced by T lymphocytes
- Stimulates proliferation of most progenitor cells, including early erythroid progenitors (BFU-E and CFU-GEMM)
- Synergizes with EPO at early stages; its effect diminishes at the CFU-E stage
- Does not directly drive terminal erythroid differentiation
4. GM-CSF (Granulocyte-Macrophage Colony-Stimulating Factor)
- Produced by T cells, endothelial cells, and fibroblasts
- Stimulates early multipotent progenitors including CFU-GEMM and early BFU-E
- Acts synergistically with EPO at early stages
- Less specific than EPO — also promotes granulocyte and monocyte lineages
Stage 2 — Late / Lineage-Specific Factor (acts on committed erythroid progenitors)
5. Erythropoietin (EPO) ⭐ — The Primary Regulator
"Erythropoietin is the most important regulator of the proliferation of committed erythroid progenitors (CFU-E) and their immediate progeny." — Goodman & Gilman's Pharmacological Basis of Therapeutics
| Property | Detail |
|---|---|
| Type | 30.4 kDa glycoprotein hormone, 193 amino acids (27 cleaved on secretion), heavily glycosylated |
| Primary source | Peritubular interstitial fibroblasts of the renal cortex (~90%) |
| Secondary source | Liver hepatocytes (~10%), important in fetal life |
| Receptor | EPO-R on surface of CFU-E and proerythroblasts |
| Action | Promotes survival, proliferation, and maturation of committed erythroid progenitors; prevents apoptosis of CFU-E |
| Stimulus for release | Hypoxia (↓ tissue O₂ delivery) |
| Amplification | With anemia or hypoxemia, EPO synthesis increases up to 100-fold |
Molecular mechanism of EPO regulation — The HIF Pathway:
Under normoxia:
- Prolyl hydroxylases hydroxylate HIF-1α (hypoxia-inducible factor)
- VHL (von Hippel-Lindau) protein recognizes hydroxylated HIF-1α → targets it for polyubiquitination and proteasomal degradation
- EPO gene expression is suppressed
Under hypoxia:
- Prolyl hydroxylases are inactive (require O₂)
- HIF-1α accumulates and dimerizes with HIF-1β
- HIF complex translocates to nucleus → binds hypoxia-response elements → activates EPO gene transcription
- A second isoform, HIF-2α, is also a critical regulator of EPO expression and iron absorption genes
Clinical relevance: Mutations causing constitutive HIF-1α or HIF-2α accumulation (e.g., VHL loss-of-function) → chronically elevated EPO → polycythemia vera-like erythrocytosis.
Summary: Growth Factors by Stage
| Growth Factor | Stage of Action | Source | Effect on Erythropoiesis |
|---|---|---|---|
| SCF | Stem cell → BFU-E | Bone marrow stroma | Mitogen for all progenitors; synergizes with EPO |
| FLT3 Ligand | Stem cell level | Stroma | Survival/expansion of early multipotent progenitors |
| IL-3 | BFU-E, CFU-GEMM | T lymphocytes | Broad early stimulation of erythroid + other lineages |
| GM-CSF | BFU-E, CFU-GEMM | T cells, endothelium | Early erythroid + myeloid stimulation; synergizes with EPO |
| EPO | CFU-E → reticulocyte | Kidney (peritubular fibroblasts) | Primary lineage-specific driver of erythroid proliferation, differentiation, and survival |
Negative Regulators of Erythropoiesis
Erythropoiesis is also inhibited by inflammatory cytokines, particularly:
- TGF-β (Transforming Growth Factor-β) — suppresses erythroid progenitor proliferation
- IFN-γ and TNF-α — suppress EPO secretion and progenitor proliferation (mechanism of anemia of chronic disease/inflammation)
- Hepcidin — produced by the liver in response to inflammation; blocks iron release from macrophages and enterocytes, reducing iron availability for erythropoiesis
Nutritional Cofactors (Required for Erythropoiesis)
Even with adequate EPO and growth factor signaling, erythropoiesis requires:
- Iron — for hemoglobin synthesis
- Vitamin B12 and Folate — for DNA synthesis (deficiency → megaloblastic anemia)
- Vitamin B6 (Pyridoxine) — for heme synthesis
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Brenner & Rector's The Kidney; Histology: A Text and Atlas (Mescher); Basic Medical Biochemistry (Lieberman & Marks)
Thymus and it's role in body
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
The Thymus and Its Role in the Body
What Is the Thymus?
The thymus is a primary lymphoid organ — a bilobed, lymphoepithelial structure situated in the superior anterior mediastinum, just behind the sternum. It is the site where T lymphocytes (T cells) are produced and matured.
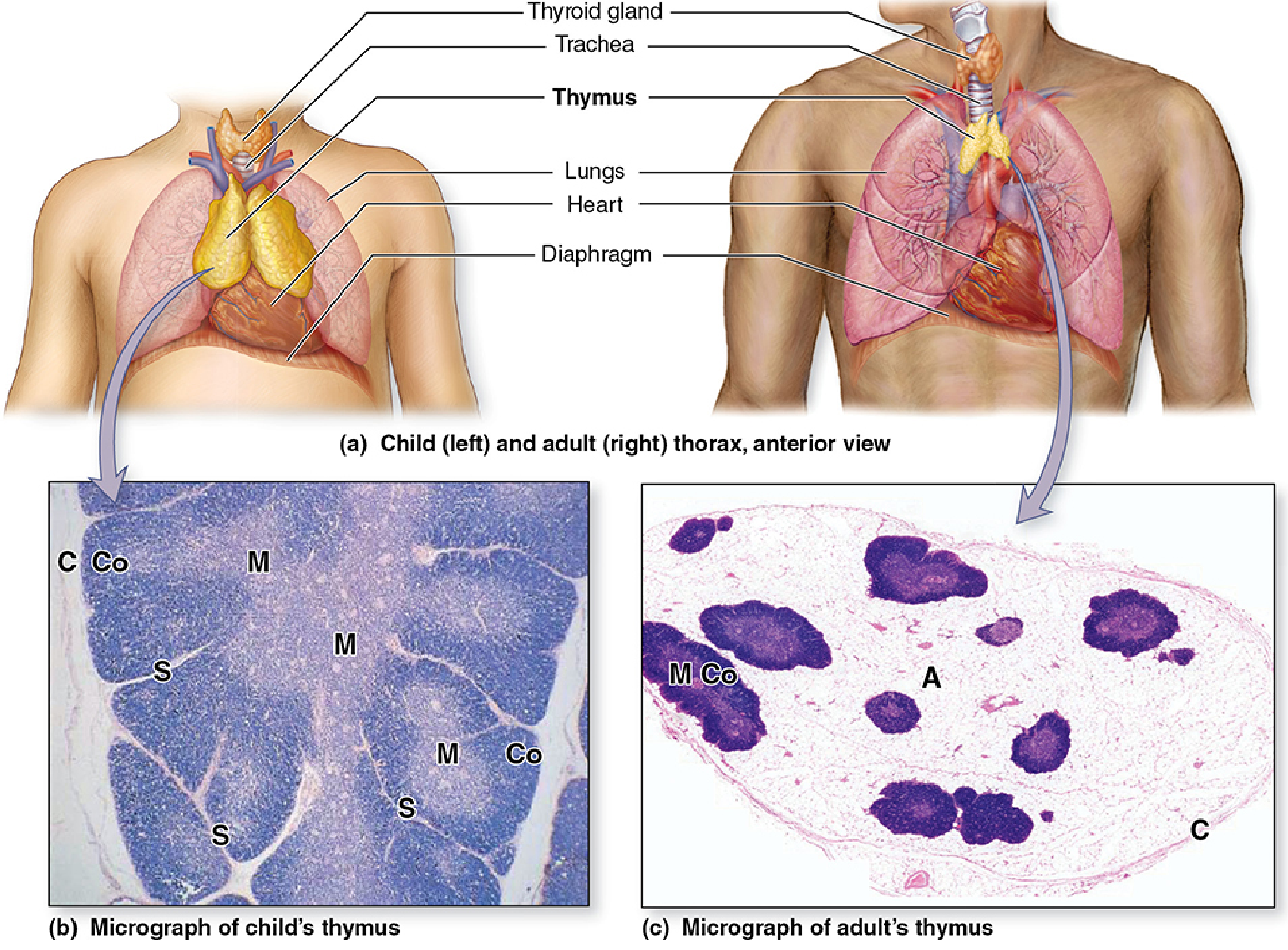
Development and Involution
| Life Stage | Status |
|---|---|
| Embryonic origin | Third (± fourth) pair of pharyngeal pouches (endoderm) |
| Weight at birth | 10–35 g |
| Maximum size | 20–50 g at puberty |
| After puberty | Progressive involution → replaced by adipose tissue; ~5–15 g in older adults |
| Old age | Only small islands of lymphoid tissue remain in adipose tissue |
Age-related thymic involution reduces the output of naïve T cells and may contribute to the decline of immune function in the elderly.
Gross and Microscopic Structure
The thymus is divided by fibrous septa into lobules, each with two distinct zones:
Cortex (outer, darkly staining)
- Densely packed with thymocytes (immature T lymphocytes) — the most proliferative zone
- Contains thymic epithelial cells (TECs) that form a cytoreticulum (meshwork scaffold)
- Cortical TECs act as antigen-presenting cells (APCs), expressing both MHC class I and II molecules
- Cortical TECs secrete IL-7 — required early in T cell development
- Surrounded by squamous TECs that form the blood-thymus barrier, preventing unregulated antigen exposure during T cell education
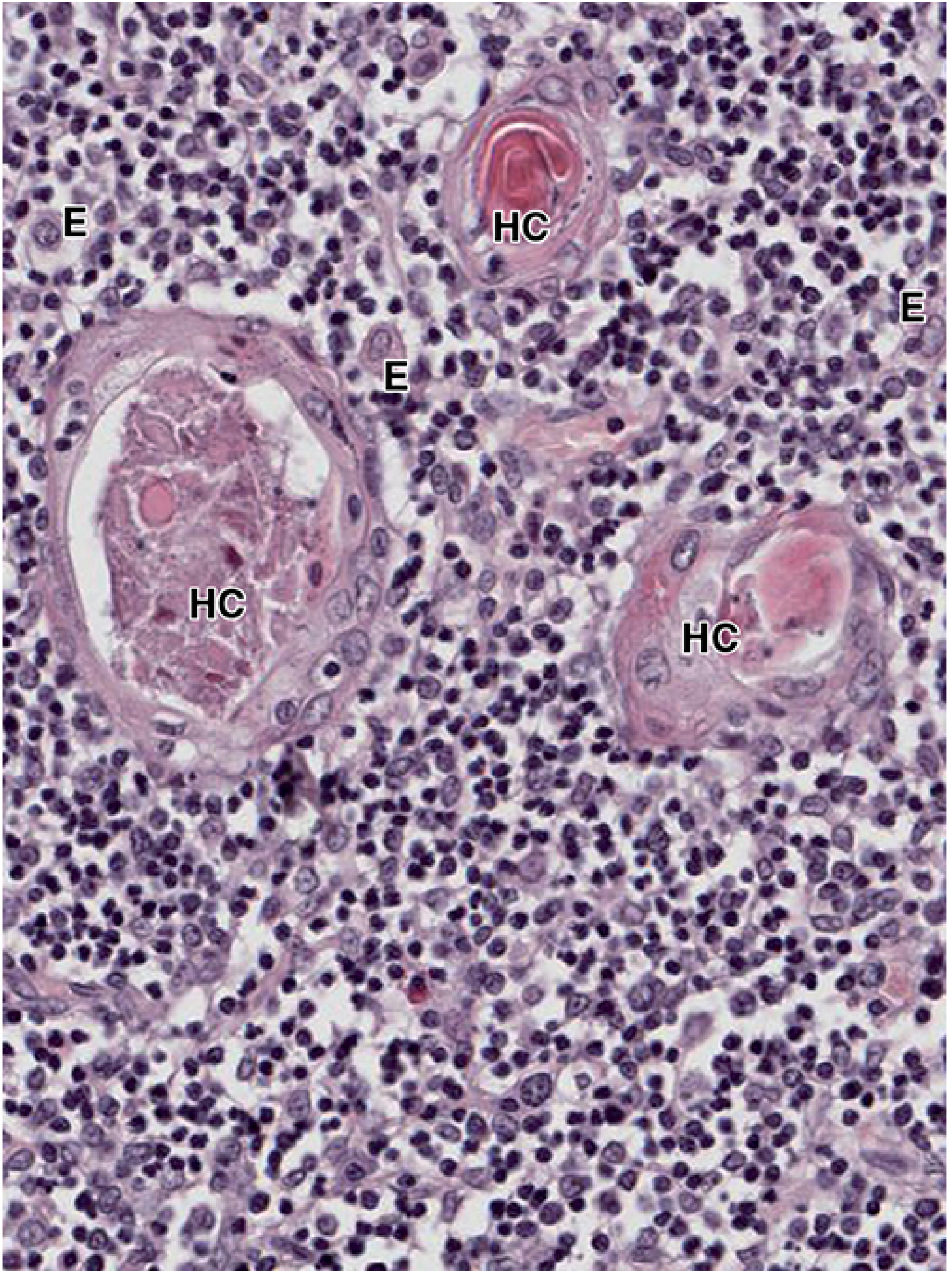
Medulla (inner, lightly staining)
- Contains fewer, more mature lymphocytes
- Contains medullary TECs (MTECs) — express tissue-specific antigens from other organs → drive negative selection
- Contains the hallmark structure: Hassall's corpuscles (thymic corpuscles)
Hassall's Corpuscles
Whorls of concentrically arranged, degenerated medullary epithelial cells (up to 100 µm in diameter). They secrete cytokines that control dendritic cell activity and promote development of regulatory T cells (Tregs) for peripheral tolerance.
Primary Role: T Cell Maturation and Education
The thymus is often called the "thymic university" — T cells enter as immature progenitors from the bone marrow and graduate as mature, self-tolerant T cells.
The process proceeds in three stages:
Stage 1 — Entry and Early Proliferation
- Immature T cell progenitors (thymocytes) enter the thymus via blood vessels
- They begin maturation in the cortex, proliferating under the influence of IL-7 from cortical TECs
- Double-negative (CD4⁻CD8⁻) → Double-positive (CD4⁺CD8⁺) thymocytes
Stage 2 — Positive Selection (Cortex)
- Thymocytes whose T cell receptors (TCRs) can recognize self-MHC molecules survive
- Those that cannot recognize self-MHC → die by apoptosis (death by neglect)
- Ensures that all mature T cells can interact with MHC molecules (MHC restriction)
- Result: CD4⁺ or CD8⁺ single-positive T cells
Stage 3 — Negative Selection (Medulla)
- Thymocytes whose TCRs bind too strongly to self-antigens presented on MTECs and dendritic cells → clonal deletion (apoptosis)
- MTECs express the AIRE gene (autoimmune regulator), allowing expression of tissue-specific antigens (e.g., insulin, thyroid antigens) in the thymic medulla
- Eliminates self-reactive T cells → central tolerance = prevention of autoimmunity
"T cells undergo differentiation and a two-stage selection process (positive and negative selection) that leads to the development of immune tolerance by eliminating all T cells directed against the body's own tissues." — Histology: A Text and Atlas (Mescher)
Only ~2–5% of thymocytes survive both selection processes and exit as mature, naïve T cells into the blood and peripheral lymphoid organs.
Summary of the Thymus's Roles
| Function | Mechanism |
|---|---|
| T cell production | Provides the microenvironment for differentiation of bone marrow progenitors into T cells |
| MHC restriction | Positive selection ensures T cells recognize self-MHC |
| Central tolerance | Negative selection eliminates self-reactive T cells (via AIRE) |
| Regulatory T cell generation | Hassall's corpuscles promote Treg development for peripheral tolerance |
| Endocrine function | Secretes thymulin, thymosin, thymopoietin — hormones that influence T cell maturation |
| Immune surveillance | Exports naïve T cells throughout life to populate peripheral lymphoid tissues |
Clinical Relevance
| Condition | Thymic Involvement |
|---|---|
| DiGeorge syndrome | Failure of pharyngeal pouch development → thymic aplasia/hypoplasia → severe T cell deficiency, recurrent infections |
| Myasthenia gravis | Thymic follicular hyperplasia (65–75% of cases); myoid cells in thymus may trigger anti-AChR autoimmunity |
| Thymoma | Neoplasm of thymic epithelial cells; associated with myasthenia gravis and other paraneoplastic syndromes |
| HIV infection | Can cause premature thymic involution, accelerating immunodeficiency |
| Age-related immunosenescence | Thymic involution → reduced naïve T cell output → impaired responses to new antigens and vaccines |
Sources: Cellular and Molecular Immunology (Abbas & Lichtman); Junqueira's Basic Histology; Histology: A Text and Atlas (Mescher); Robbins, Cotran & Kumar Pathologic Basis of Disease
Histology of thymus
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.