Acute GI Bleeding
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastrointestinal bleeding" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-grounded overview of Acute GI Bleeding.
Acute Gastrointestinal Bleeding
1. Classification by Location
GI bleeding is divided anatomically:
| Category | Location | Typical Presentation |
|---|---|---|
| Upper GI (UGI) | Proximal to ligament of Treitz | Hematemesis, melena, coffee-ground emesis |
| Mid-GI | Small bowel (jejunum/ileum) | Occult bleeding, intermittent melena or hematochezia |
| Lower GI (LGI) | Colon, rectum, anus | Hematochezia (bright red or maroon stool) |
2. Etiology
Upper GI Bleeding (most common causes in adults)
- Peptic ulcer disease - historically 50% of UGI bleeds; epigastric pain + hematemesis, especially in NSAID/aspirin users
- Esophagogastric varices - painless massive bleeding in a cirrhotic patient
- Mallory-Weiss tear - vomiting/retching followed by hematemesis
- Erosive gastritis/esophagitis - GERD, heavy alcohol use, odynophagia
- Dieulafoy's lesion - large submucosal artery eroding through mucosa
- Gastric antral vascular ectasia (GAVE) - "watermelon stomach," associated with scleroderma
- Aortoenteric fistula - GI bleeding in a patient with prior aortic aneurysm repair (herald bleed)
Mid-GI Bleeding
- Angioectasias - recurrent bleeding in elderly patients with chronic renal failure or aortic stenosis
- Meckel diverticulum - painless large-volume bleeding in a child or young adult
- NSAID enteropathy, Crohn's disease, small bowel tumors
Lower GI Bleeding
- Diverticulosis - painless, intermittent large-volume hematochezia (most common cause in adults)
- Internal hemorrhoids - intermittent low-volume bright red blood on tissue or dripping into toilet water
- Colon ischemia - abdominal pain + hematochezia in elderly patient with cardiovascular disease
- Angiodysplasia
- Colorectal neoplasms
- Inflammatory bowel disease
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Table 65.2
3. Initial Assessment
History
Ask about: medications (NSAIDs, anticoagulants, antiplatelet agents), prior GI surgeries, alcohol use, liver disease, hemoptysis vs. hematemesis, prior GI procedures.
Physical Examination
- Vital signs - tachycardia (HR >100), hypotension, orthostasis indicate significant blood loss
- Signs of hypovolemic shock - cool clammy skin, mottled skin, flat JVP, oliguria
- Stigmata of chronic liver disease - telangiectasias, palmar erythema, gynecomastia, ascites, splenomegaly, caput medusae
- Skin findings - purpura (Henoch-Schonlein purpura), pigmented lip lesions (Peutz-Jeghers), acanthosis nigricans (malignancy)
- Clinical findings most predictive of severe UGI bleeding: bright red blood in NG lavage, HR >100, hemoglobin <8 g/dL
Investigations
- CBC with platelet count
- Electrolytes, BUN/creatinine (elevated BUN:creatinine ratio suggests UGI bleeding)
- Liver function tests + coagulation profile (INR, PT)
- Type and crossmatch
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 297
4. Risk Stratification
Three major scoring tools for upper GI bleeding:
| Score | Key Variables | Best For |
|---|---|---|
| Glasgow-Blatchford (GBS) | BP, HR, Hgb, BUN, melena, syncope, liver/cardiac failure | Predicting need for intervention or death; GBS ≤1 = safe discharge; GBS ≥7 = needs endoscopic therapy |
| Rockall Score | Age, shock, comorbidities + endoscopic findings | Post-endoscopy mortality prediction |
| AIMS65 | Albumin <3, INR >1.5, altered mental status, SBP <90, age >65 | Mortality, length of stay, cost |
The GBS is superior at predicting the combined endpoint of hospital-based intervention or death and is endorsed by ESGE, the International Consensus Group, and the Asia-Pacific Working Group.
For lower GI bleeding, no universally accepted tool exists. The Oakland Score predicts safe discharge from the emergency department.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 3203-3205
5. Resuscitation
Management Algorithm for Severe UGI Bleeding
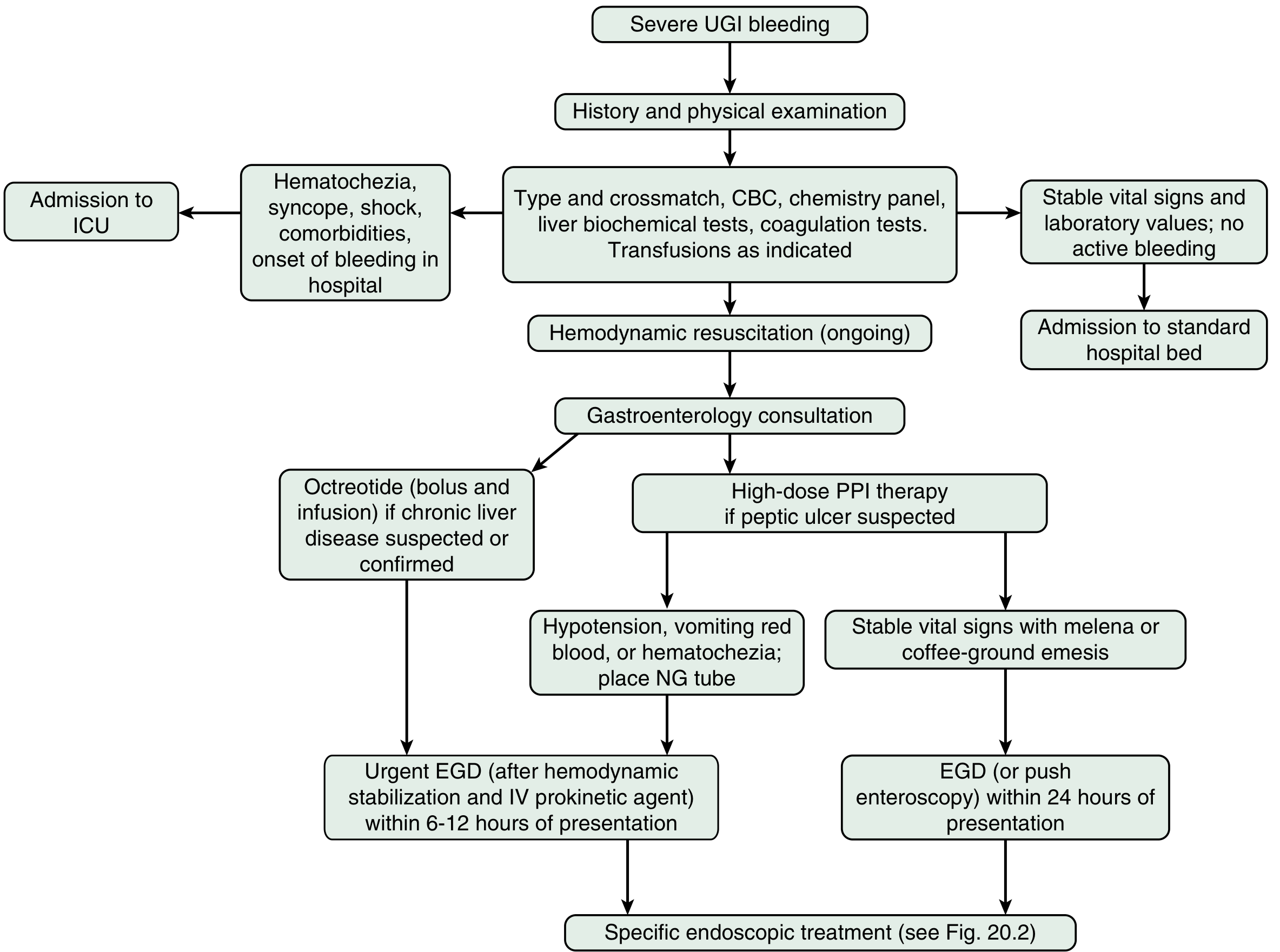
Step-by-step:
-
Airway - Prophylactic endotracheal intubation ONLY if the patient cannot protect the airway or is inadequately ventilating (routine prophylactic intubation is NOT indicated - associated with increased cardiopulmonary complications).
-
IV Access + Volume - Two large-bore IV catheters in antecubital veins; start isotonic saline.
-
Blood Transfusion:
- Restrictive strategy: transfuse PRBCs when Hgb < 7 g/dL (supported by multiple RCTs and guidelines)
- Higher threshold (Hgb 8-10 g/dL) for patients with ischemic cardiac disease
- Massive hemorrhage: balanced resuscitation - 1:1:1 ratio of PRBCs : FFP : platelets
-
Hemodynamic monitoring - ICU admission for active bleeding, significant blood loss, or high-risk features: hematochezia, syncope, shock, comorbidities, or in-hospital onset. Place urinary catheter; monitor HR, BP, SpO2, urine output, mental status.
-
Nasogastric tube - Controversial; useful to detect bright red blood (increases likelihood of severe UGI source), but does not affect mortality, LOS, or transfusion need.
Management of Antithrombotic Drugs
- 29-44% of severe GI bleeds occur in patients on antithrombotic agents
- Vitamin K antagonists (warfarin) with life-threatening bleeding: reverse with 4-factor prothrombin complex concentrate (PCC) + vitamin K (FFP if PCC unavailable); do NOT delay endoscopy to await reversal
- Manage all antithrombotic agents in consultation with cardiology
6. Pharmacotherapy
Proton Pump Inhibitors (Non-variceal UGI Bleeding)
- Pre-endoscopy: Start high-dose IV PPI if peptic ulcer suspected - reduces stigmata of recent hemorrhage at endoscopy
- Post-endoscopy (high-risk stigmata): High-dose PPI bolus + continuous infusion for 72 hours
Octreotide (Variceal Bleeding)
- Drug of choice if endoscopy cannot be performed urgently
- Adult dose: 50 mcg IV bolus then 25-50 mcg/hr continuous infusion
- Pediatric dose: 1-2 mcg/kg bolus (max 50 mcg), then 1-2 mcg/kg/hr infusion (max 4 mcg/kg/hr)
- Main adverse effect: hyperglycemia
Vasopressin
- Alternative to octreotide for variceal bleeding (limited by peripheral/central vasoconstriction)
- Pediatric: 0.002-0.005 unit/kg/min, max 0.01 unit/kg/min
7. Endoscopy
Upper GI Bleeding
- Urgent EGD (within 6-12 hours): for hypotension, vomiting red blood, hematochezia, or suspected variceal bleeding
- EGD within 24 hours: stable patients with melena or coffee-ground emesis
- IV prokinetic (erythromycin or metoclopramide) 30-90 minutes before EGD improves gastric visualization and reduces need for repeat endoscopy
Forrest Classification - Peptic Ulcer Stigmata
| Endoscopic Finding | Forrest Class | Rebleeding Risk (without Rx) | Management |
|---|---|---|---|
| Active spurting | Ia | ~90% | Endoscopic hemostasis + high-dose PPI 72h |
| Active oozing | Ib | ~10% | Endoscopic hemostasis + high-dose PPI 72h |
| Non-bleeding visible vessel (NBVV) | IIa | ~50% | Endoscopic hemostasis + high-dose PPI 72h |
| Adherent clot | IIb | ~33% | Clot removal + hemostasis if underlying high-risk stigmata |
| Flat pigmented spot | IIc | ~7% | PPI only; no endoscopic treatment |
| Clean ulcer base | III | ~3% | PPI only; early discharge possible |
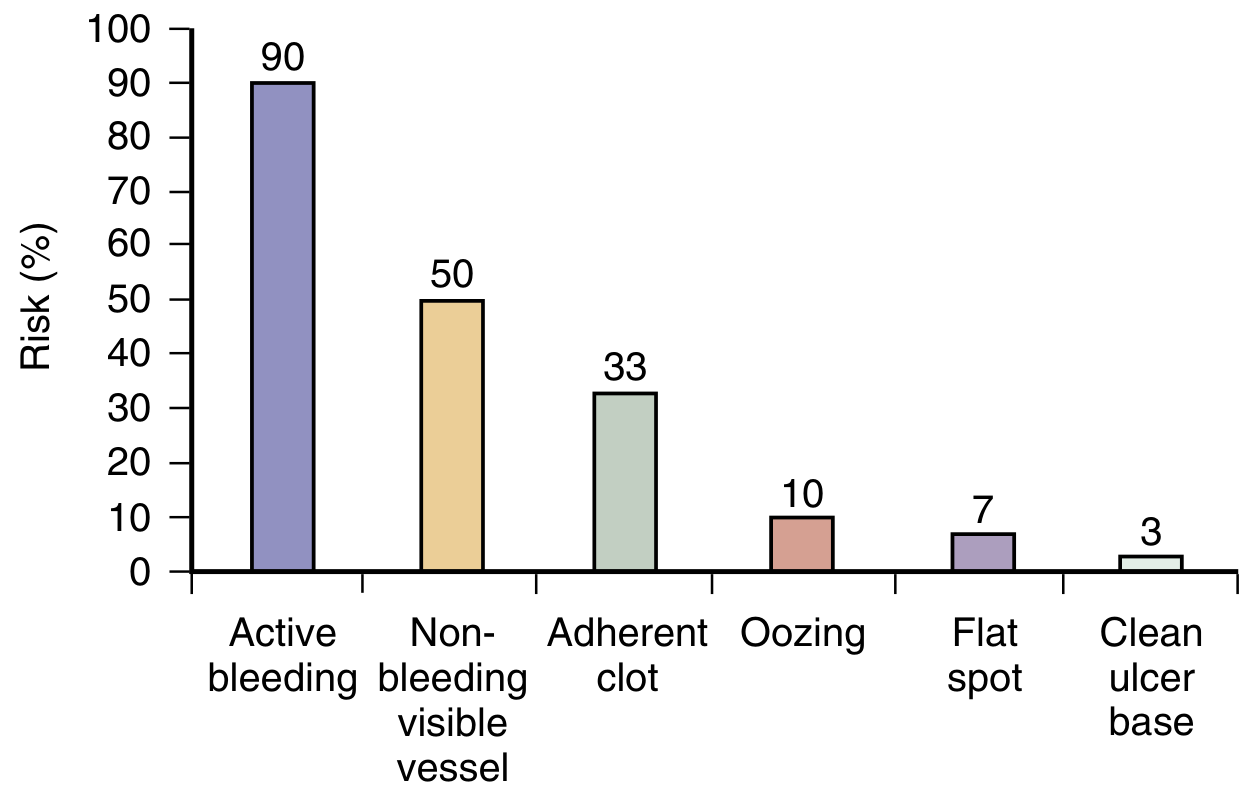
Forrest Ia, IIa, and IIb are high-risk stigmata requiring endoscopic hemostasis. Modalities include:
- Epinephrine injection (1:10,000 - 1:20,000)
- Coaptive thermal probe (heater probe or bipolar probe)
- Hemostatic clips
- Combination therapy is superior to monotherapy for active bleeding
Lower GI Bleeding (Colonoscopy)
- Within 12-14 hours for severe or ongoing active hematochezia (after colonic purge with 6-8 L PEG over 4-6 hours)
- Within 24 hours for mild/moderate self-limited hematochezia
- Metoclopramide 10 mg IV before/during purge to reduce nausea and facilitate gastric emptying
8. Mid-GI (Small Bowel) Bleeding
~70% of patients with overt GI hemorrhage in whom EGD and colonoscopy are both negative are bleeding from the small bowel.
Diagnostic approach:
- Hemodynamically unstable: CT angiography first to localize bleeding
- Hemodynamically stable: Repeat EGD/colonoscopy (identifies source in 30-40% of cases)
- Video Capsule Endoscopy (VCE): Test of choice for stable patients; 80-90% small bowel visualization, 80% diagnostic yield (highest if performed within 2-3 days of hemorrhage); contraindicated if bowel obstruction suspected (1% capsule retention rate)
- Device-Assisted Enteroscopy (DAE): Diagnostic yield ~60%, increases to 75% after positive VCE; allows therapeutic hemostasis
- CT enterography: 40-57% yield for inflammatory/neoplastic/vascular lesions
- Tc-99m pertechnetate scintigraphy (Meckel scan): >90% sensitivity in children; <50% in adults
9. Independent Risk Factors for Persistent or Recurrent Bleeding
- Bright red blood on rectal exam or in NG aspirate
- Active arterial bleeding at endoscopy
- Large ulcer size (>2 cm)
- Posterior duodenal ulcer or lesser gastric curvature ulcer (overlying major vessels)
- Comorbid illnesses (cardiac, renal, hepatic disease)
- Coagulopathy
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Table 20.4
10. Special Populations
Pediatric GI Bleeding
Age strongly determines likely etiology (see age-based table from Tintinalli's):
- Neonates: Swallowed maternal blood, hemorrhagic disease of newborn (Vit K deficiency), NEC
- Infants/Toddlers: Anal fissure (lower GI), Mallory-Weiss, intussusception
- Children/Adolescents: Mallory-Weiss, H. pylori gastritis, IBD, polyps, Meckel diverticulum
Cirrhosis/Portal Hypertension
- Octreotide infusion + urgent EGD (band ligation preferred over sclerotherapy for esophageal varices)
- Prophylactic antibiotics (norfloxacin or ceftriaxone) reduce bacterial infection and rebleeding
Recent Evidence Note
Two 2025 meta-analyses (PMIDs 40029534 and 40752050) specifically examined tranexamic acid (TXA) in acute GI bleeding. Unlike its established role in trauma, TXA has NOT shown consistent mortality benefit in GI bleeding in recent large RCTs (notably the HALT-IT trial), and both meta-analyses reflect ongoing debate. Current guidelines do not routinely recommend TXA for GI bleeding - this is an area of active investigation that may update existing recommendations.
A 2025 meta-analysis (PMID 40317012) confirms the BUN:creatinine ratio as a useful biomarker in critical care settings, supporting its use as an adjunct marker for UGI vs. LGI source.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Mulholland and Greenfield's Surgery, 7e | Tintinalli's Emergency Medicine | Clinical Gastrointestinal Endoscopy, 3e | Bailey and Love's Short Practice of Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.