JNA its definition, site of origin, pathogenesis, histopathology, clinical features, Fisch staging classification, differential diagnosis, management (investigation and treatment), complications according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the information needed from authoritative ENT textbooks (Cummings, Scott-Brown's, Robbins). I have comprehensive details on all the requested topics. The Fisch classification is referenced in the textbooks as a well-known system, and I know it from established medical knowledge. Let me now compose the comprehensive answer.
Juvenile Nasopharyngeal Angiofibroma (JNA)
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 & 2; Robbins & Cotran Pathologic Basis of Disease
Definition
Juvenile Nasopharyngeal Angiofibroma (JNA) is a benign but locally aggressive, highly vascular tumor of the nasopharynx. It is histologically characterized by vascular endothelium-lined spaces embedded in a fibrous stroma, and it occurs almost exclusively in adolescent males. Although histologically benign, it displays locally destructive behavior and may extend intracranially.
Immunohistochemical and electron microscopy studies suggest it may represent a vascular malformation (hamartoma) rather than a true neoplasm. - Cummings Otolaryngology, p. 988
It accounts for less than 1% of all head and neck tumors. - Cummings Otolaryngology, p. 1768
Site of Origin
The tumor has a pathognomonic epicenter of origin at the pterygopalatine fossa, at the level of the sphenopalatine foramen and the base of the pterygoid process on the lateral nasal wall. Recent imaging-based studies have further focused attention on the superior portion of the choana and the root of the pterygoid process as the precise point of origin. - Cummings Otolaryngology, p. 988
From this origin, it spreads predictably along foramina and fissures of the skull base:
- Medially through the sphenopalatine foramen into the nasopharynx and nasal cavity
- Superiorly along the vidian nerve into the floor of the sphenoid sinus
- Laterally through the pterygomaxillary fissure into the infratemporal fossa
- Anteriorly, pushing the posterior wall of the maxillary sinus forward
- Intracranially via the inferior/superior orbital fissure, or along the maxillary nerve to the parasellar region (less common)

Pathogenesis
Hormonal Theory
JNA occurs almost exclusively in adolescent males. The tumor cells express androgen receptors, and there is evidence of estrogen receptor involvement. The nasal mucosal target cells are thought to develop muscularized vascular channels secondary to testosterone stimulation and estrogen hypersensitivity at puberty. This is consistent with the observation that some tumors reportedly regress after puberty. - Scott-Brown's Vol. 1, p. 2889
Branchial Arch / Vascular Malformation Theory
Schick et al. postulated that JNA develops from incomplete regression of the first branchial arch artery, which arises in embryogenesis between days 22-24 and transiently connects the ventral and dorsal aortas. Incomplete regression of this structure leaves vascular remnants that may develop into JNA - supported by the finding that JA vessels express laminin α2, a marker of early angiogenesis. - Cummings Otolaryngology, p. 988
Molecular Pathogenesis
- β-catenin (CTNNB1) mutations are found in the majority of sporadic JNAs - Robbins & Cotran, p. 690
- JNA can also occur syndromically in familial adenomatous polyposis (FAP) via germline APC gene mutations, also leading to β-catenin activation
- Upregulation of VEGFA and activation of VEGF/FGFR signaling pathways implicated in angiogenesis
- Additional markers studied: bFGF, H-Ras, IL-6, c-Kit, c-Myc, PDGFa, TP53 - Cummings Otolaryngology, p. 988
Histopathology
Gross Pathology
- Sessile, lobulated, rubbery mass; dark red to tan-gray in color
- Can be large; unencapsulated
- Admixture of vascular tissue and fibrous stroma
- Mucosal ulceration is not a feature - Cummings Otolaryngology, p. 1768
Microscopic Features
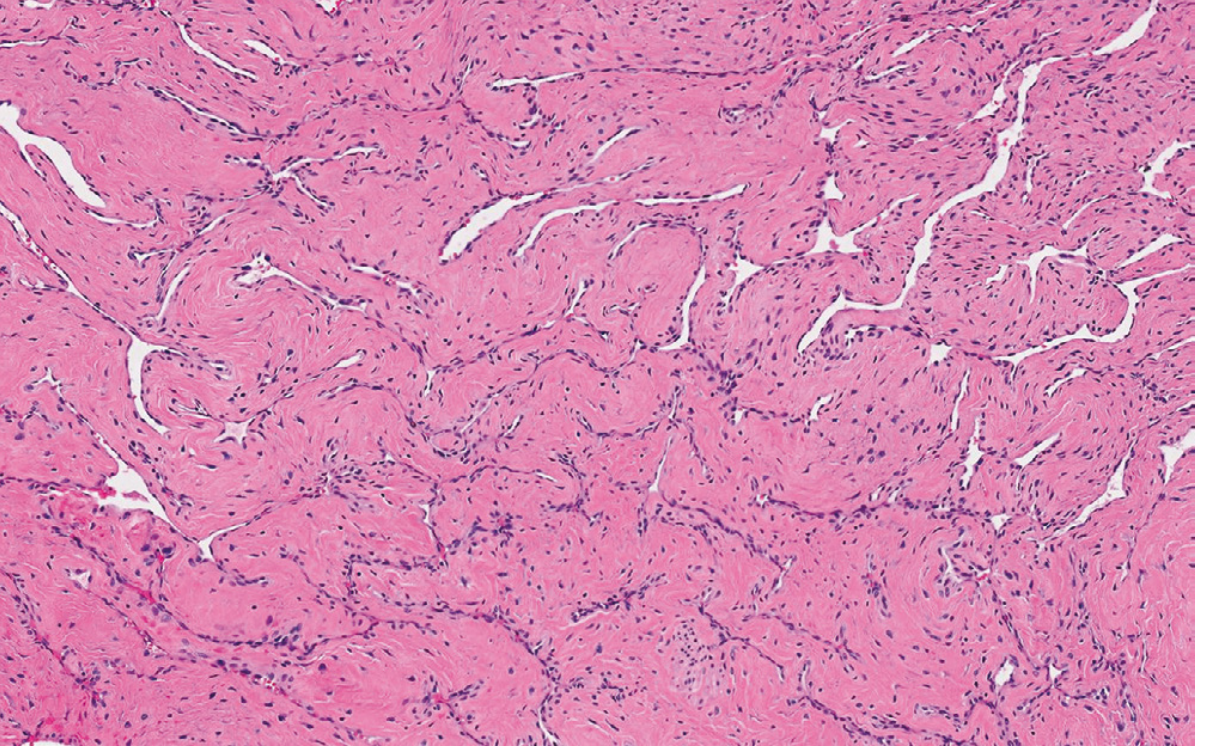
- Vascular component: Thin-walled, irregular vascular channels of varying caliber - some large sinusoidal spaces, some smaller capillary-type vessels
- Key feature: Vessel walls lack elastic fibers and have incomplete or absent smooth muscle - this explains the tendency for profuse, uncontrolled bleeding when incised (vessels cannot contract)
- The endothelial lining is a single layer; no muscle layer in larger sinusoidal spaces
- Stromal component: Dense collagenous stroma containing bland spindle-shaped fibroblasts/myofibroblasts; no atypia or mitoses
- Scott-Brown's describes vascular cavities with endothelial layer but no muscle layer, mixed with a more conventional arteriocapillary tree with muscle layers - Scott-Brown's Vol. 1, p. 2889-2893
- Robbins: "numerous vessels embedded in a dense collagenous stroma" - Robbins & Cotran, p. 690
Clinical Features
- Age and sex: Typically adolescent males, ages 10-25 years; rare in females and older patients - Cummings Otolaryngology, p. 1768
- Unilateral nasal obstruction (most common presenting symptom)
- Epistaxis - recurrent, often severe; may lead to anemia - Scott-Brown's Vol. 1, p. 2903
- Blood-stained sputum
- Serous otitis media (Eustachian tube obstruction)
Symptoms with Advanced Disease
- Facial swelling / cheek swelling - infratemporal fossa involvement
- Proptosis and diplopia - orbital involvement
- Headache - cranial fossa involvement
- Nasal discharge, anosmia, sinusitis
Examination Findings
- Endoscopy: smooth, hypervascularized polypoid mass originating behind the middle turbinate, which is laterally displaced; choana may be completely obstructed
- The lesion bleeds readily on contact
- A clinical presentation of nasal obstruction + epistaxis in a teenage boy with an endoscopic hypervascular nasopharyngeal mass is virtually diagnostic
Fisch Staging Classification
The Fisch classification (originally described by Fisch and subsequently modified) is the most widely used staging system for JNA in standard ENT practice:
| Stage | Description |
|---|---|
| I | Tumor limited to the nasopharynx and nasal cavity; no bone destruction |
| II | Tumor invading the pterygopalatine fossa, maxillary, ethmoid or sphenoid sinuses with bone destruction |
| IIIa | Tumor invading the infratemporal fossa or orbital region without intracranial involvement |
| IIIb | Tumor invading the infratemporal fossa or orbit with intracranial extradural (parasellar) involvement |
| IVa | Intracranial intradural tumor without infiltration of the cavernous sinus, pituitary fossa, or optic chiasm |
| IVb | Intracranial intradural tumor with infiltration of the cavernous sinus, pituitary fossa, or optic chiasm |
The Scott-Brown's textbook specifically references Fisch Class IIIb-IV as indications for infratemporal fossa approach surgery. - Scott-Brown's Vol. 2, p. 2195-2202
Other Staging Systems
Several classification systems exist in the literature; Cummings notes they should be used to stratify cases by extent for comparing outcomes:
- Chandler (1984): 4-stage system - Stage I (nasopharynx only) → Stage II (nasal cavity/sphenoid) → Stage III (maxillary sinus, ethmoid, infratemporal fossa, orbit, cavernous sinus) → Stage IV (intracranial)
- Andrews-Fisch (1980): The standard Fisch I-IV classification above
- Snyderman/UPMC (2010): Emphasizes residual vascularization from the internal carotid artery after embolization and route of intracranial growth as predictors of endoscopic resectability - Cummings Otolaryngology, p. 990
Differential Diagnosis
Other diagnoses to consider in a teenager with nasopharyngeal mass:
- Antrochoanal polyp - benign, non-vascular; arises from maxillary sinus; pale, non-pulsatile; occurs in both sexes
- Lobular capillary hemangioma (pyogenic granuloma) - vascular but different location and age group; does not involve pterygopalatine fossa
- Hemangiopericytoma - different age group; does not involve pterygopalatine fossa
- Schwannoma / neurofibroma - enhances on imaging but lacks flow voids; different origin
- Nasopharyngeal carcinoma - older age group; lymphadenopathy; ulceration common
- Rhabdomyosarcoma - pediatric malignancy; rapid growth; destructive imaging features
- Lymphoma - systemic features, lymphadenopathy
- Chordoma - midline origin from clivus, different age/presentation
Key distinguishing feature of JNA on imaging: origin invariably at pterygopalatine fossa, hypervascular enhancement with flow voids on MRI, and occurrence in an adolescent male. - Cummings Otolaryngology, p. 989
Management
Investigations
Imaging
-
CT with contrast (primary initial investigation):
- Shows enhancing soft tissue mass arising from nasopharynx/lateral wall
- Classically demonstrates widening of the pterygopalatine fossa
- "Antral sign" / Holman-Miller sign: anterior bowing of posterior maxillary sinus wall
- Bone expansion with diffuse/patchy enhancement suggests invasion
- Dural enhancement suggests intracranial extension
- Bone erosion is uncommon in early disease
-
MRI with contrast (gadolinium):
- T1 and T2 sequences show multiple flow voids (signal voids from large feeding vessels) - pathognomonic
- Better delineates soft tissue extent, intracranial spread, orbital involvement
- Preferred for postoperative surveillance - Cummings Otolaryngology, p. 1769
-
Digital Subtraction Angiography (DSA):
- Shows enlarged intratumoral vessels; intense inhomogeneous blush in venous phase
- Maps vascular supply: primarily external carotid artery (internal maxillary artery, ascending pharyngeal artery) - internal carotid involvement in ~35% of cases
- Essential before embolization
- Shows connections with ICA, vertebral artery, and contralateral carotid
-
MR Angiography: Less invasive vascular mapping option
Biopsy
- Biopsy is avoided due to extremely high risk of hemorrhage. Diagnosis is established clinically and radiologically. Final histologic proof is obtained from the surgical specimen. - Cummings Otolaryngology, p. 1769
Treatment
Pre-operative Embolization
- Standard adjunct performed 24-48 hours before surgery
- Dramatically reduces intraoperative blood loss and improves surgical access; improves visualization of tumor borders
- Particles (polyvinyl alcohol - PVA) or liquid agents (NBCA, Onyx) via transarterial approach
- Direct tumor puncture with Onyx is increasingly used, especially when ICA supply is present
- Devascularization is more complete with Onyx direct puncture than traditional transarterial techniques
- Not without controversy - some authors note increased likelihood of residual disease at tumor periphery after embolization, and advocate clipping the maxillary artery early in small tumors instead
- Complications: facial dull ache (common), transient facial numbness/hemiparesis; rare: blindness, permanent neurologic deficit - Scott-Brown's Vol. 1, p. 2926-2940
Surgery (Primary Treatment)
Surgery is the mainstay of management. - Cummings Otolaryngology, p. 990
Approach selection based on tumor stage:
| Approach | Indication |
|---|---|
| Endoscopic endonasal (transnasal) | Stages I-III; now standard for early/intermediate lesions; preferred where expertise available |
| Transpalatal (intraoral) | Small lesions limited to nasopharynx |
| Lateral rhinotomy / medial maxillectomy | Intermediate lesions |
| Midfacial degloving | Good access, avoids facial scars; intermediate-to-advanced |
| Le Fort I osteotomy | Access to maxillary sinuses, ethmoid, pterygopalatine canal |
| Facial translocation | Large lesions with infratemporal fossa involvement |
| Infratemporal fossa approach (Fisch type C/D) | Fisch Stage IIIb-IV; intracranial extension; requires neurosurgical collaboration |
Key surgical principles:
- Dissection in the subperiosteal plane with bipolar coagulation
- Extensive drilling of the basisphenoid where the tumor grows in digitations - reduces recurrence rates
- Early control of the maxillary artery reduces bleeding in small tumors
Non-surgical (Adjuvant) Options
- Radiotherapy: Reserved for unresectable tumors, extensive intracranial involvement, or recurrent disease not amenable to re-resection with acceptable morbidity. Dose typically 30-45 Gy.
- Gamma Knife / CyberKnife radiosurgery: Alternatives with low morbidity for small residual lesions
- Hormonal therapy: Flutamide (androgen antagonist) has shown tumor reduction in some reports and may serve as a preoperative adjunct; not standard practice
- Anti-angiogenic/targeted therapy: Under investigation (VEGF, FGFR pathway targeting)
Post-operative Surveillance
- Periodic endoscopy and contrast-enhanced CT or MRI for minimum of 3 years
- MRI is preferred as residual lesions tend to grow submucosally
- Imaging in the immediate postoperative period best detects residual disease before inflammatory changes develop
- Residual/recurrent disease rate: 6-39%; more likely with preoperative skull base involvement and residual ICA vascularization after embolization
- Most residual lesions diagnosed within 1 year
- Residual disease: monitored with MRI; treatment scheduled only when clear progressive growth is demonstrated - Cummings Otolaryngology, p. 991
Complications
Tumor-Related Complications
- Severe epistaxis and anemia from tumor vascularity
- Intracranial extension (Fisch Stage IIIb-IV) - uncommon but reported
- Visual impairment / blindness from orbital involvement
- Eustachian tube obstruction → serous otitis media, conductive hearing loss
- Cranial nerve compression in advanced disease
- Malignant transformation: Very rare; reported cases of transformation to fibrosarcoma (Makek, Andrews, Fisch) - Cummings references
- Fatality: Recurrence rates approach 20%; approximately 9% of cases can be fatal (usually due to massive hemorrhage or intracranial invasion) - Robbins & Cotran, p. 690
Treatment-Related Complications
Embolization complications:
- Facial pain/dull ache (most common)
- Transient facial numbness
- Transient hemiparesis
- Blindness (rare case reports)
- Permanent neurological deficit (rare) - Scott-Brown's Vol. 1, p. 2936-2940
Surgical complications:
- Massive intraoperative hemorrhage (major risk)
- Residual disease (6-39%)
- CSF leak (in operations for intracranial lesions)
- Meningitis
- Cranial nerve injury
- Facial scarring (with open approaches)
- Orbital injury/diplopia
- Nasal obstruction/synechiae
Radiotherapy complications (if used):
- Radiation-induced malignancy (osteosarcoma, fibrosarcoma) - long-term risk
- Growth disturbance in skeletally immature patients
- Cataracts, dry eye
- Pituitary dysfunction
Compiled from: Cummings Otolaryngology Head and Neck Surgery (Chapter 50, p. 987-991; Chapter 95, p. 1768-1770); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (p. 2887-2940); Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 690)
This is a shared conversation. Sign in to Orris to start your own chat.