Lead time in screening
Reading File
Searching the Web
lead time bias screening epidemiology definition
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a thorough explanation of lead time and lead time bias in screening, drawn from multiple medical textbooks.
Lead Time in Screening
Definition
Lead time is the interval between:
- The point when a disease is detected by a screening test (before symptoms appear), and
- The point when it would have been diagnosed clinically (i.e., when symptoms bring the patient to medical attention)
In other words, it is the "head start" that screening gives over symptom-driven diagnosis. The goal of early detection is to push that first moment of diagnosis as far left on the timeline as possible.
- Campbell Walsh Wein Urology, p. 602
- Swanson's Family Medicine Review
Lead Time Bias
Lead time bias is the systematic error that arises when survival statistics make a screening program appear effective even when it has no real effect on the disease course.
How it works:
If a patient is diagnosed via screening (at an earlier point), their "clock" (measured survival from diagnosis) starts earlier. If the time of death is unchanged, the patient still dies at the same point - but their measured survival time from diagnosis is longer, purely because the diagnosis was made earlier.
"The point of death is not moved back; the disease was simply detected earlier making it seem that life expectancy is improved."
- Textbook of Family Medicine 9e, p. 122
Visual Explanation
Figure 1 - Lead time and length bias timeline:
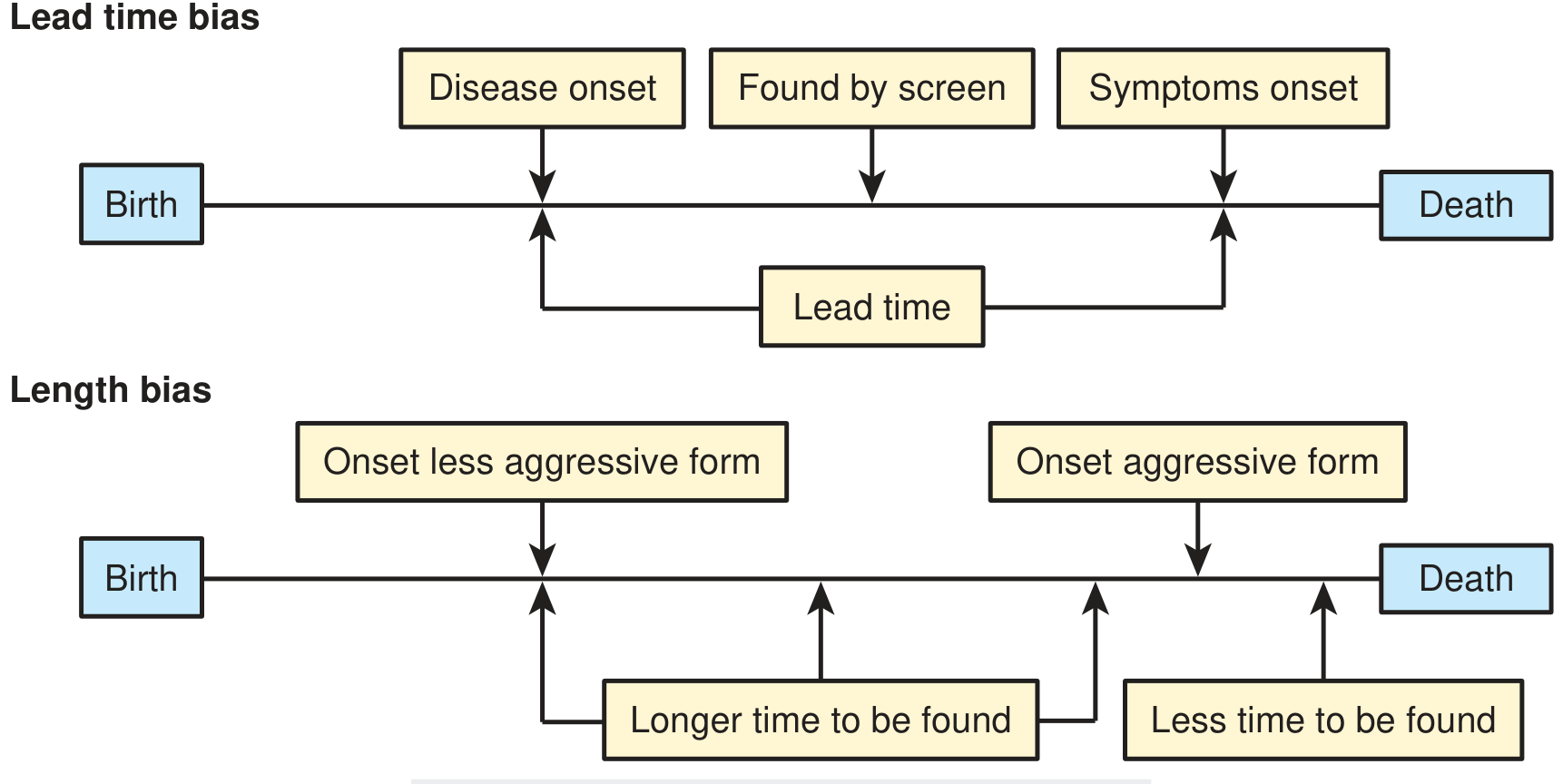
As the diagram shows:
- Lead time = the gap between "Found by screen" and "Symptoms onset"
- The death point is the same whether or not the patient was screened
- The screened patient appears to "survive longer" from diagnosis, but total lifespan is identical
Figure 2 - Screened vs. unscreened patient timelines:
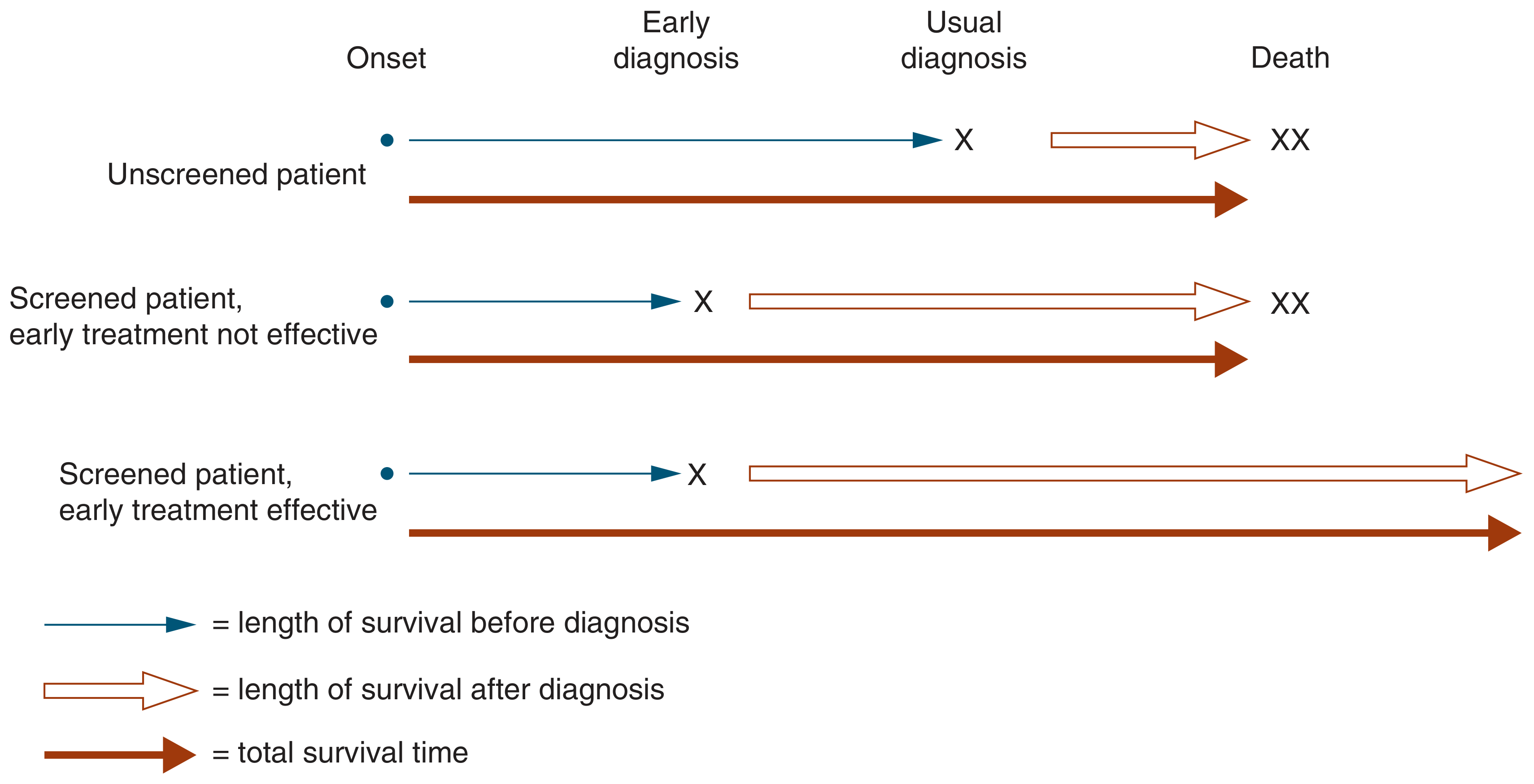
This illustrates three scenarios:
- Unscreened patient - diagnosed at symptom onset, dies at the usual time
- Screened patient, early treatment NOT effective - diagnosed earlier, but dies at the same time. The post-diagnosis survival interval appears longer, but total survival is the same. This is pure lead time bias.
- Screened patient, early treatment IS effective - diagnosed earlier AND lives genuinely longer. This is real benefit, not bias.
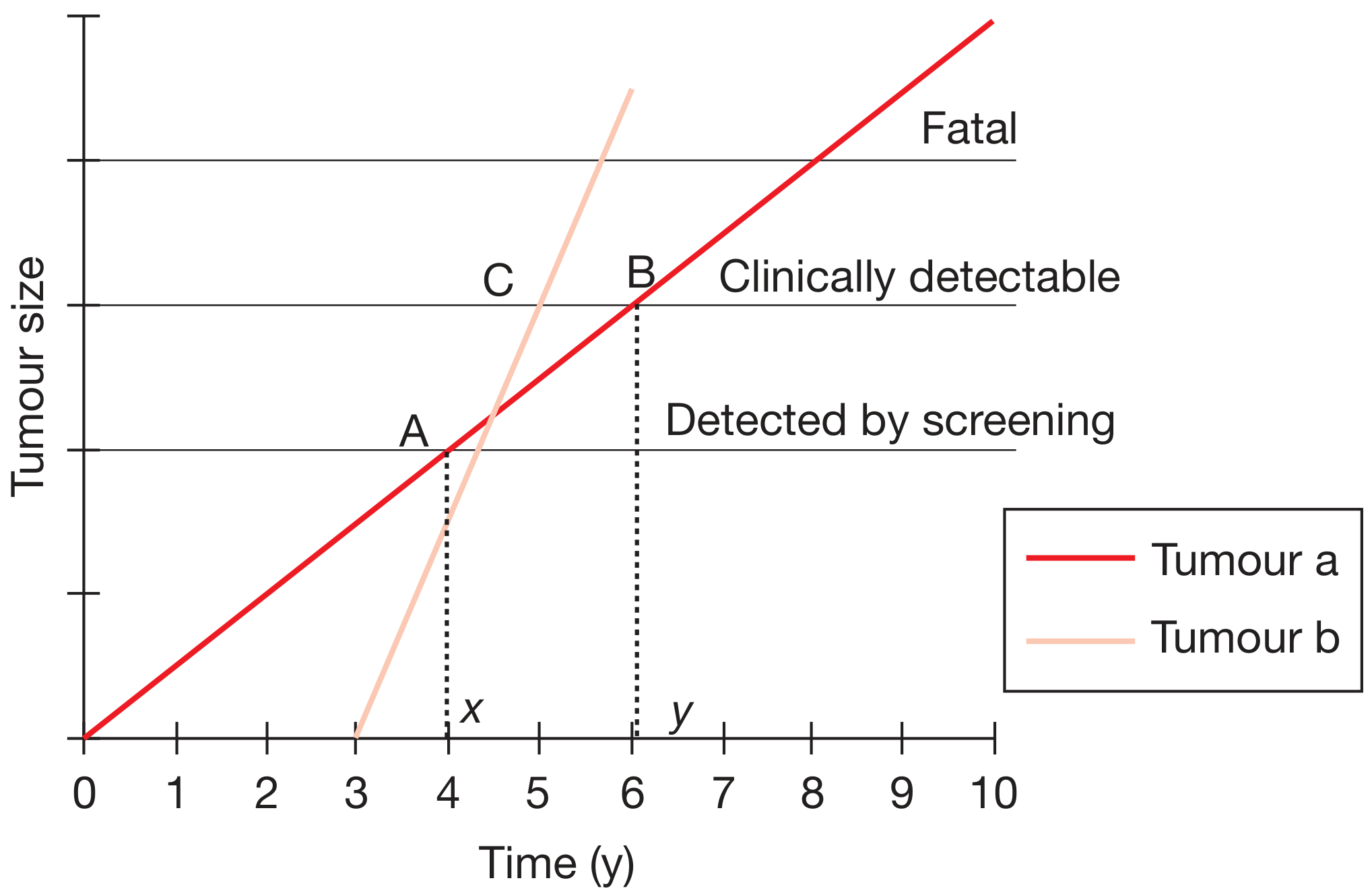
Figure 3 - Tumour growth curves illustrating lead time and length bias:
-
Tumour a (slow-growing, red line): Detected by screening at point A (year ~4), would not be clinically detectable until point B (year ~6). Lead time = y - x ≈ 2 years. This 2-year "survival gain" is entirely artefactual if treatment makes no difference.
-
Tumour b (fast-growing, pale line): Grows so quickly it crosses both screening threshold (C) and clinical threshold within a single screening interval - it is "missed" by screening and presents symptomatically with rapid progression. This is also used to illustrate length bias.
-
Bailey and Love's Short Practice of Surgery 28e, p. (Fig. 12.4)
Lead Time Bias vs. Length Bias - Key Distinction
| Feature | Lead Time Bias | Length Bias |
|---|---|---|
| Mechanism | Earlier diagnosis shifts the clock, not the death | Screening preferentially detects slow-growing, less aggressive disease |
| Effect | Artificially inflates survival time from diagnosis | Artificially inflates survival by enriching for indolent disease |
| Example | Kidney cancer: 5-yr survival rose 50%→75% while mortality unchanged | Screen-detected cancers tend to be less aggressive than symptom-detected ones |
Classic Real-World Examples
-
Kidney cancer - Incidence doubled over 30 years (more CT scanning detecting incidental renal masses). Five-year survival rose from 50% to 75%. Yet population-level kidney cancer mortality remained stable - the apparent benefit is almost entirely lead time bias. (Campbell Walsh Wein Urology)
-
PSA screening for prostate cancer - Claims of improved survival from PSA testing have been attributed partly to lead time bias, since PSA diagnoses cancer earlier without necessarily preventing death from it.
-
Mammography - Lead time of mammographic breast cancer detection is age-related: it determines the interval at which repeat screening is needed. (Grainger & Allison's Diagnostic Radiology)
How to Correct for Lead Time Bias
Because of this bias, observational survival studies comparing screened vs. unscreened cohorts are unreliable for proving a screening test works. The correct approach is:
- Population-based randomized controlled trials (RCTs) comparing mortality rate in a whole population offered screening vs. one not offered screening
- Use disease-specific mortality (or all-cause mortality) rather than survival from diagnosis as the endpoint
- Statistical methods to estimate and subtract lead time from survival analyses
This design has been successfully applied to breast cancer and colorectal cancer screening, both showing genuine reduction in disease-specific mortality - confirming real benefit beyond lead time bias.
- Bailey and Love's Short Practice of Surgery 28e
- Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.