Genu varus in detail according to orthopaedics text books
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from the orthopaedics textbooks. Let me compile the full detailed answer.
Genu Varus (Genu Varum) - Detailed Orthopaedic Review
Definition
Genu varus (also called genu varum, or "bow legs") is a deformity of the lower limb in the frontal (coronal) plane where the axis deviation causes the knee joint to be displaced lateral to the mechanical axis of the limb (the Mikulicz line). The tibia points toward the median line - i.e., the deformity is concave toward the vertical body axis.
Clinically, when the knees are separated and the medial malleoli are touching (feet together), an intercondylar distance greater than 3 cm is considered abnormal.
- General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy)
Mechanical Axis and Biomechanics
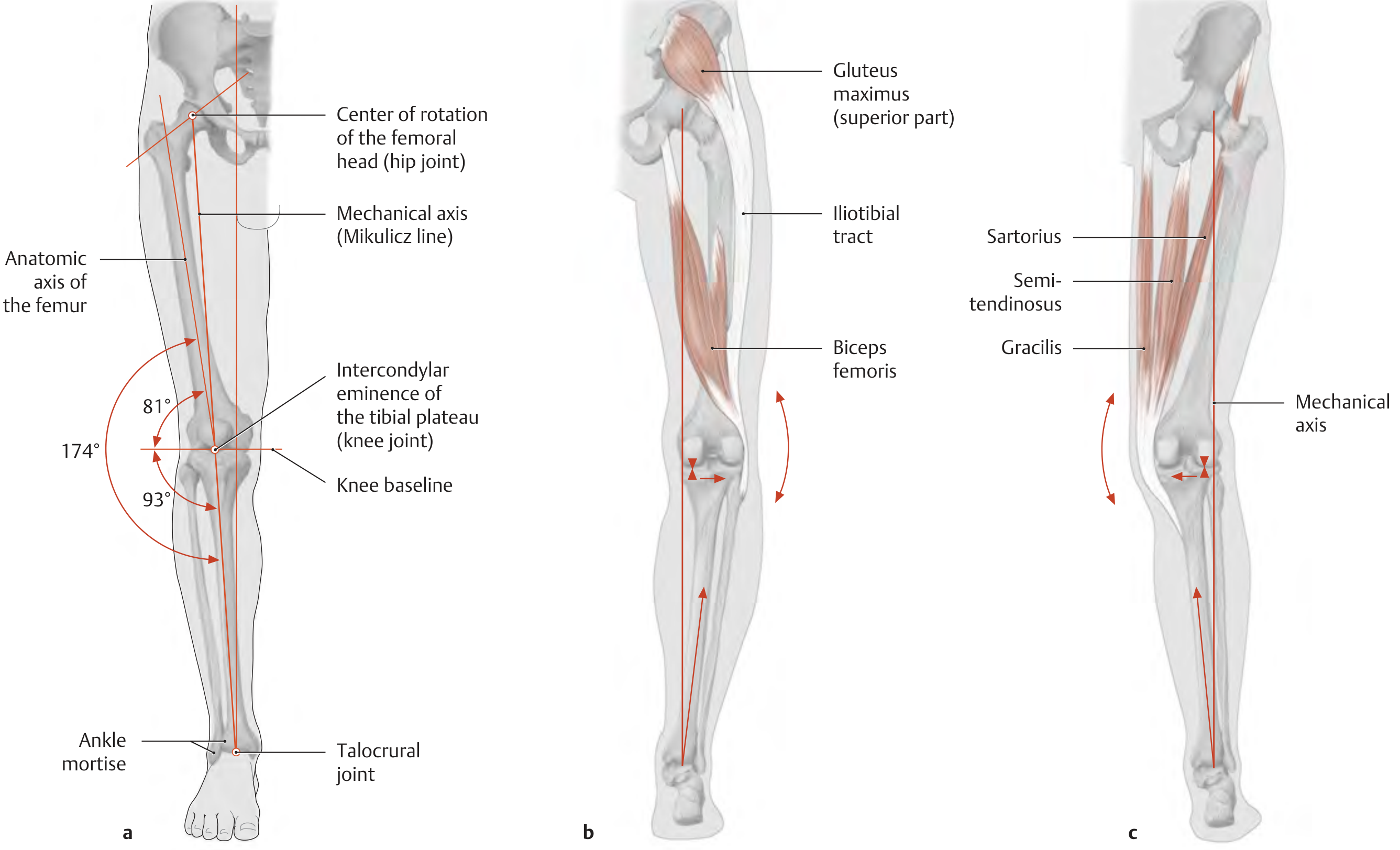
The Mikulicz line (mechanical axis) normally runs from the center of rotation of the femoral head through the intercondylar eminence of the tibial plateau to the center of the ankle mortise. The anatomic and mechanical axes of the femur diverge at a 6-degree angle, making the femorotibial angle normally 174° at the knee (a laterally open angle).
In genu varum:
- The center of the knee joint lies lateral to the mechanical axis
- The medial joint complex is subjected to abnormal compressive pressure
- The lateral structures (lateral collateral ligament, iliotibial tract, biceps femoris) are subjected to abnormal tension
- Greater stress is placed on the lateral border of the foot, resulting in a fallen pedal arch
- Progressive degenerative changes (medial compartment osteoarthritis) develop over time
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
Physiologic vs. Pathologic Genu Varum
Normal developmental progression (physiologic)
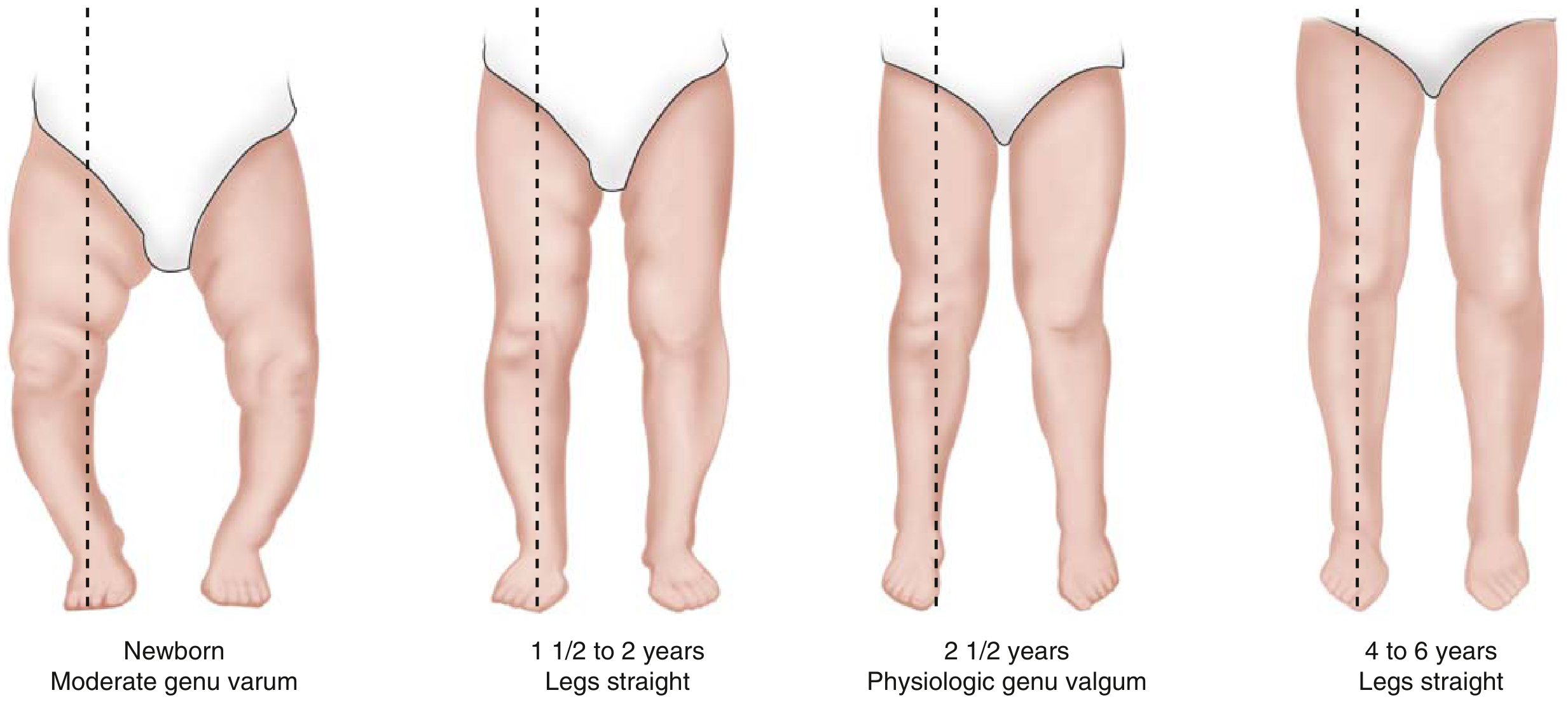
The above figure from Miller's Review illustrates the normal physiologic sequence:
| Age | Alignment |
|---|---|
| Newborn | Moderate genu varum |
| 1.5-2 years | Legs straight |
| 2.5 years | Physiologic genu valgum |
| 4-6 years | Legs straight (adult alignment) |
- Up to 20° of genu varum is considered normal during the first year of life
- Physiologic genu varum normally evolves to genu valgum by age 2.5 years, with transition to physiologic valgus angulation by age 4
- Radiographs in physiologic bowing show symmetric flaring of the tibia and femur
- No treatment is needed for physiologic bowing
Pathologic Causes
- Blount disease (tibia vara) - most common pathologic cause
- Osteogenesis imperfecta
- Osteochondromas
- Trauma
- Various skeletal dysplasias
- Rickets (X-linked hypophosphatemic / vitamin D-resistant: defect in cellular endopeptidase, presents with short stature and genu varum, with physeal widening and metaphyseal cupping on radiographs)
- Achondroplasia and other dwarfism syndromes (dwarfs with disproportionately short extremities tend to have genu varum)
- Miller's Review of Orthopaedics, 9th Edition
Blount Disease (Tibia Vara) - The Most Important Pathologic Cause
History and Pathogenesis
Erlacher first described tibia vara (1922), but Blount's 1937 article gave the condition its name, describing it as "an osteochondrosis similar to coxa plana and Madelung deformity but located at the medial side of the proximal tibial epiphysis." It is now considered an acquired disease of the proximal tibial physis, not an epiphyseal dysplasia.
Exact cause is unknown, but the following factors are implicated:
- Altered enchondral ossification
- Hereditary and developmental factors (most likely combination)
- Weight bearing is required - does not occur in non-ambulatory patients
- Strongly associated with early walking and obesity
- Rising incidence linked to the "obesity epidemic" and vitamin D deficiency
The abnormality is characterized by:
- Varus and internal torsion of the tibia
- Genu procurvatum
Types of Blount Disease
Infantile Blount Disease (age 0-8 years)
- Begins before age 8
- Bilateral and symmetric in 60% (vs. physiologic bowing which is 100% bilateral)
- Progressive varus (vs. physiologic bowing which resolves with growth)
- Difficult to differentiate from physiologic bowing at <2 years
- Classic presentation: overweight child who begins walking before 1 year of age, associated with internal tibial torsion
- More common overall
Adolescent Blount Disease (late onset)
- Less severe than infantile forms
- More often unilateral
- Epiphysis appears relatively normal - no beaking as seen in infantile type
- Most characteristic radiographic finding: widening of the proximal medial physis
- Thought to result from mechanical overload in genetically susceptible patients (obese, Black individuals)
- A variant ("obesity-related Blount") shows dome-shaped metaphysis, open growth plate, and inferomedial translation of the proximal tibial epiphysis
Radiographic Assessment
Key Radiographic Findings (Infantile Blount)
- Medial half of proximal tibial epiphysis is short, thin, and wedged
- Physis is irregular in contour and slopes medially
- Proximal metaphysis forms a palpable medial projection
- Medial metaphyseal fragmentation is pathognomonic for progressive tibia vara
- Angular deformity occurs just distal to the medial projection
MRI Additional Findings
- Increased thickness of the chondroepiphysis of the proximal medial tibia
- Increased height and width of the medial meniscus
- Abnormal medial femoral epiphysis
Measurement Tools
1. Drennan Metaphyseal-Diaphyseal Angle
- Lines drawn along the longitudinal axis of the tibia and through the metaphyseal beaks
- >11-16 degrees = abnormal (classic Drennan threshold is >16°)
- A Drennan angle >16° strongly suggests tibia vara over physiologic bowing
2. Tibiofemoral Angle
- Lines drawn along the longitudinal axes of the tibia and femur
- In Blount disease, the tibiofemoral angle does not progress normally from varus to valgus between 1.5-3 years
3. Mechanical Axis (Long-Film Radiograph)
- Most functional measurement of the amount of deformity
- Standing long-film radiographs recommended
- Femoral varus of 10 degrees more than the calculated ideal femoral-tibial joint angle represents 34-76% of the genu varum deformity
Langenskiöld Classification (Infantile Blount)
The Langenskiöld classification describes six stages based on progressive epiphyseal-metaphyseal changes. At stage VI, the medial portion of the epiphysis fuses at a 90-degree downward angle - the most severe form.
Treatment
Physiologic Genu Varum
- Observation only - resolves spontaneously
- No bracing or surgery needed
Infantile Blount Disease
| Stage / Age | Treatment |
|---|---|
| Children aged 2-3 years, Stage I-II | Observation or KAFO bracing (knee-ankle-foot orthosis) |
| Children >3 years, Stage II-III | Proximal osteotomy of tibia/fibula with valgus angulation (mild overcorrection) |
| Stages IV-VI | Complex - multiple procedures may be needed; epiphysiolysis for stages V-VI |
Key surgical principle: Valgus osteotomy of the proximal tibia and fibula with mild overcorrection is recommended in young children (<4 years), because medial physeal growth abnormalities persist.
Recurrence rates:
- Children >4 years: 80-90% recurrence after osteotomy
- Children <4 years: <20% recurrence
Guided Growth (Emerging Technique)
- Temporary epiphysiodesis using tension band plates (eight-plate technique)
- Lateral guided growth correction based on the Hueter-Volkmann law (growth is decreased by compression; returns when compression is removed)
- Minimally invasive vs. osteotomy
- ~12% implant failure rate requiring return to OR
- Growing evidence supports use at earlier ages
Adolescent Blount Disease
- First-line when growth remains: Proximal tibial and fibular lateral hemiepiphysiodesis
- Larger plates usually required (due to plate failure incidence in obese patients)
- If physes are closed or residual deformity exists: tibial and fibular osteotomy
- Ilizarov technique for deformity correction + lengthening when significant LLD is present
Osteotomy Techniques
Proximal Tibial Osteotomy for Genu Varum
Oblique osteotomy (Rab technique):
- Begins distal to the tibial tubercle, through a transverse cosmetic incision
- An oblique osteotomy directed anterodistal to posteroproximal simultaneously corrects varus and internal rotation
- In Blount disease, patients have approximately equal amounts of varus and internal rotation
- A 45-degree upward osteotomy provides adequate correction in most patients
- Post-operative cast wedging possible since no rigid internal fixation
Other techniques:
- Crescent-shaped chevron osteotomy (Greene) - maintains limb length
- Hemicondylar tibial osteotomy (Zayer) through the epiphysis into the intercondylar notch - corrects posteromedial slope of the tibial epiphysis
External Fixation
- Uniplanar external fixator: easy to apply, adjustable, allows early weight bearing, avoids second operation
- Hexapod-based (Ilizarov-type) systems: preferred for obese patients with complex multi-plane deformities; allows computer-navigated correction of residual deformity post-operatively
- Excellent correction with good safety profile
Neurovascular Complications
- Peroneal nerve palsy
- Vascular occlusion (anterior tibial artery compression occurs with valgus correction; stretching occurs with varus correction at the interosseous membrane)
Genu Varum in the Context of Arthritis
In the adult knee, genu varum leads to medial compartment overload and eventual medial compartment osteoarthritis. The "triple varus knee" (Noyes) describes:
- Genu varum alignment
- Soft-tissue varus instability
- Lateral/varus thrust in the stance phase of ambulation
This is the most advanced form requiring combined bony and soft-tissue reconstruction.
Summary Table
| Feature | Physiologic | Infantile Blount | Adolescent Blount |
|---|---|---|---|
| Age | <2 years | <8 years | >8 years |
| Bilaterality | 100% | 60% | Usually unilateral |
| Progression | Resolves | Progressive | Variable |
| Drennan angle | <11° | >11-16° | (Less reliable) |
| Epiphyseal beaking | Absent | Present | Absent |
| Medial physis changes | Absent | Fragmentation | Widening |
| Treatment | Observation | KAFO → osteotomy | Hemiepiphysiodesis → osteotomy |
Sources:
- Miller's Review of Orthopaedics, 9th Edition - Chapter on Leg/Knee
- Campbell's Operative Orthopaedics, 15th Ed 2026 - Tibia Vara (Chapter 34)
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System - Mechanical Axis sections
This is a shared conversation. Sign in to Orris to start your own chat.