Bones and Cartilages from laiq Hussain full chapter
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Note: Laiq Hussain Siddiqui's textbook is not in this library's catalog. The chapter below is compiled from the best available anatomy and histology sources covering all standard topics found in that chapter: Gray's Anatomy for Students, Histology: A Text and Atlas (Ross & Pawlina), The Developing Human (Moore & Persaud), THIEME General Anatomy Atlas, and Imaging Anatomy Vol. 3 - Bones, Joints, Vessels and Nerves.
BONES AND CARTILAGES
Full Chapter - General Anatomy
PART I: CARTILAGE
Definition and General Features
Cartilage is an avascular form of connective tissue composed of cells called chondrocytes embedded in a firm yet pliable extracellular matrix. Over 95% of cartilage volume is extracellular matrix. Because cartilage contains no blood vessels, lymphatics, or nerves, chondrocytes are nourished entirely by diffusion through the matrix from surrounding perichondrial vessels (or, in articular cartilage, from synovial fluid).
Functions:
- Supports soft tissues
- Provides smooth, low-friction gliding surfaces at joints
- Enables longitudinal growth of long bones (epiphyseal plates)
- Structural support in the respiratory tract (larynx, trachea, bronchi)
- Shock absorption (intervertebral discs, menisci)
Types of Cartilage
There are three types, distinguished by their extracellular matrix composition:
1. Hyaline Cartilage (Most Common)
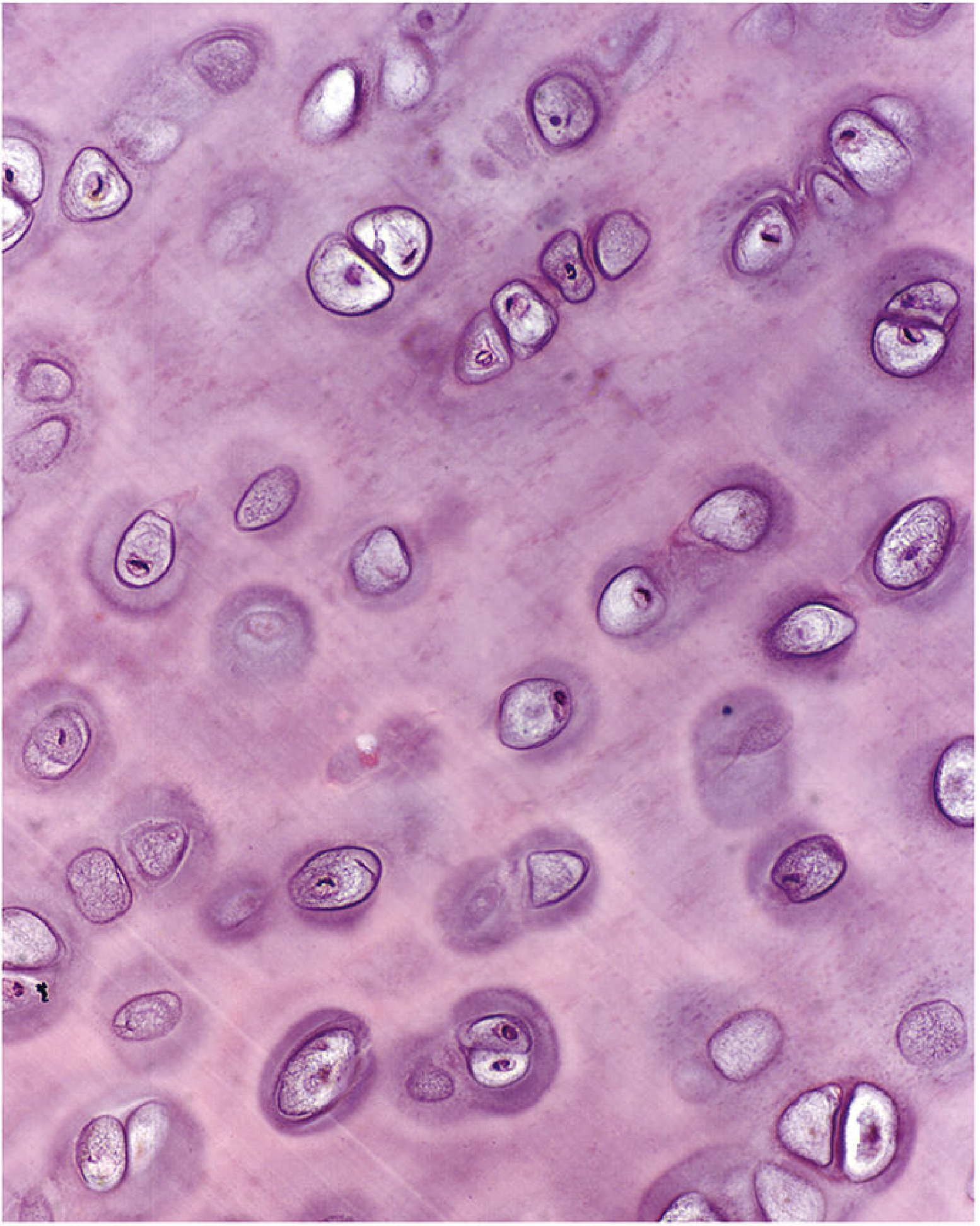
Matrix: Type II collagen fibers, glycosaminoglycans (GAGs), proteoglycans (mainly aggrecan), and multiadhesive glycoproteins. Collagen fibers are fine and invisible on routine light microscopy, giving the matrix a glassy (hyaline = glass-like) appearance.
Perichondrium: Present everywhere EXCEPT on articular surfaces and epiphyseal plates.
Locations:
| Site | Role |
|---|---|
| Fetal skeleton | Template for endochondral ossification |
| Articular surfaces of synovial joints | Low-friction gliding |
| Costal cartilages (ribs 1-10) | Attachment to sternum; flexibility of thorax |
| Epiphyseal growth plates | Longitudinal bone growth |
| Laryngeal cartilages (thyroid, cricoid, arytenoids) | Structural support of airway |
| Tracheal rings and bronchial plates | Keep airways patent |
| Nasal septum and cartilages | Structural support |
Histological zones of matrix staining:
- Capsular (pericellular) matrix - immediately surrounds each chondrocyte; darkest staining; highest concentration of sulfated proteoglycans, hyaluronan, and type VI collagen; type VI collagen anchors cells via integrin receptors
- Territorial matrix - surrounds the isogenous group; type II collagen fibrils randomly arranged; less intensely stained
- Interterritorial matrix - between cell groups; least stained; occupies the bulk of matrix volume
Isogenous groups (cell nests): Chondrocytes divide within their lacunae but cannot escape through the solid matrix, so daughter cells cluster together forming groups of 2-8 cells called isogenous groups.
2. Elastic Cartilage
Matrix: Same as hyaline PLUS abundant elastic fibers and elastic lamellae, clearly visible on special stains (orcein, resorcin-fuchsin). Perichondrium present.
Locations:
- Pinna (auricle) of the external ear
- External auditory canal
- Eustachian (auditory) tube
- Epiglottis
- Corniculate and cuneiform cartilages of larynx
- Vocal folds
Function: Provides flexibility and elasticity - can bend and spring back to original shape. Does NOT undergo endochondral ossification.
3. Fibrocartilage
Matrix: Predominantly type I collagen (large, clearly visible bundles on light microscopy) PLUS type II collagen and small amounts of proteoglycans. Chondrocytes appear in rows between collagen bundles.
Perichondrium: ABSENT - the only cartilage without a perichondrium; transitions directly with adjacent dense connective tissue.
Locations:
| Location | Function |
|---|---|
| Intervertebral discs (annulus fibrosus) | Shock absorption; resists compression and torsion |
| Pubic symphysis | Weight transmission; allows slight mobility during childbirth |
| Articular discs of sternoclavicular joint | Load distribution |
| Articular discs of temporomandibular joint | Load distribution |
| Menisci of knee joint | Load distribution; joint stability |
| Triangular fibrocartilage complex (wrist) | Wrist stability |
| Tendon/bone insertion sites | Anchors tendons to bone |
Comparison Table:
| Feature | Hyaline | Elastic | Fibrocartilage |
|---|---|---|---|
| Main collagen type | Type II | Type II + elastic fibers | Type I (+ Type II) |
| Perichondrium | Yes (except articular/epiphyseal) | Yes | No |
| Appearance | Glassy, homogeneous | Yellow (fresh specimen) | Fibrous, dense |
| Endochondral ossification | Yes | No | No |
| Repair capacity | Poor | Poor | Moderate |
Perichondrium
All cartilage except articular cartilage and fibrocartilage is covered by perichondrium, a layer of dense connective tissue with two layers:
- Outer fibrous layer - dense connective tissue; contains fibroblasts; provides mechanical support
- Inner chondrogenic layer - contains chondroprogenitor cells capable of differentiating into chondroblasts; vascular; responsible for appositional growth and repair
Chondrogenesis (Cartilage Development)
Cartilage develops from mesenchyme during the 5th embryonic week:
- Mesenchymal cells aggregate → form a chondrogenic nodule (chondrification center)
- Transcription factor SOX-9 triggers differentiation into chondroblasts
- Chondroblasts secrete cartilage matrix (type II collagen, proteoglycans)
- As chondroblasts become surrounded by their own matrix, they mature into chondrocytes (trapped in lacunae)
- Surrounding mesenchyme forms the perichondrium
Two modes of cartilage growth:
- Interstitial growth - chondrocytes divide within lacunae, expanding cartilage from within; only possible in young, pliable cartilage
- Appositional growth - chondroprogenitor cells in the perichondrium differentiate and add new cartilage to the surface; predominates in mature cartilage
Repair of Cartilage
Hyaline cartilage has very limited capacity for repair due to avascularity. Damage results in fibrocartilaginous scar. Articular cartilage repair is particularly poor (no perichondrium). This underlies the progressive, irreversible degradation seen in osteoarthritis.
PART II: BONE
Definition and General Features
Bone is a calcified, living connective tissue - the hardest tissue in the body. It consists of cells and a mineralized extracellular matrix. The mineral is calcium phosphate in the form of hydroxyapatite crystals [Ca₁₀(PO₄)₆(OH)₂], which constitutes approximately 65% of dry bone weight. The organic component (~35%) is mainly type I collagen (~90% of organic weight) plus noncollagenous proteins.
Functions of bone:
- Support - structural framework of the body
- Protection - shields vital organs (brain, heart, lungs, spinal cord)
- Movement - levers on which muscles act via tendons
- Mineral homeostasis - reservoir for 99% of body calcium and 85% of body phosphate
- Hematopoiesis - red marrow in spongy bone produces all blood cells
- Energy storage - yellow marrow contains adipocytes (energy reserve)
The adult human skeleton consists of 206 bones.
Classification of Bones (by Shape)
| Type | Description | Examples |
|---|---|---|
| Long bones | Longer in one dimension; shaft + two expanded ends | Humerus, femur, tibia, fibula, radius, ulna, metacarpals, metatarsals, phalanges |
| Short bones | Roughly equal in all dimensions (cuboidal) | Carpals (wrist), tarsals (ankle) |
| Flat bones | Thin, plate-like; two compact layers sandwiching spongy bone | Skull vault, scapula, sternum, ribs, ilium |
| Irregular bones | Complex shapes that don't fit other categories | Vertebrae, facial bones, ethmoid |
| Sesamoid bones | Develop within tendons; reduce tendon friction | Patella (largest), sesamoids of thumb and big toe |
| Pneumatic bones | Contain air-filled sinuses | Frontal, maxilla, ethmoid, sphenoid |
| Accessory (Wormian) bones | Supernumerary; result from failure of ossification center fusion | Skull sutures; foot |
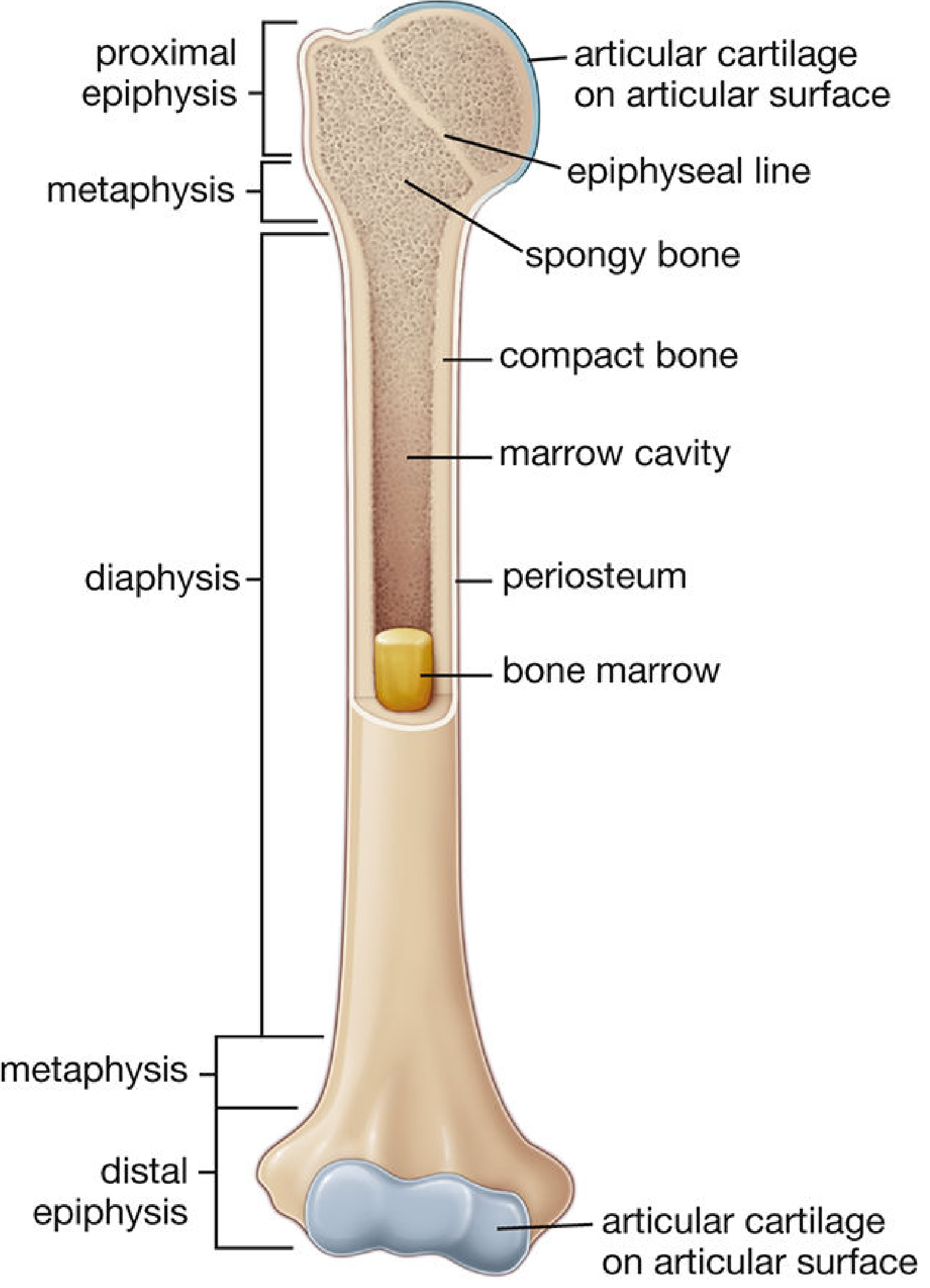
Structure of a Long Bone
| Region | Description |
|---|---|
| Diaphysis | The shaft; thick-walled cylinder of compact bone surrounding the medullary (marrow) cavity; contains yellow (fatty) marrow in adults |
| Epiphysis | Expanded proximal and distal ends; chiefly spongy bone with a thin compact shell; articular surface covered by hyaline (articular) cartilage |
| Metaphysis | Flared region between diaphysis and epiphysis; contains epiphyseal plate in growing bone; becomes epiphyseal line after growth ceases |
| Epiphyseal plate (growth plate / physis) | Disc of hyaline cartilage between epiphysis and metaphysis; site of longitudinal bone growth; replaced by bone (epiphyseal line) at skeletal maturity |
| Articular cartilage | Hyaline cartilage covering articulating surface of epiphysis; no perichondrium; nourished by synovial fluid |
| Medullary (marrow) cavity | Central cavity within the diaphysis; contains yellow marrow in adults, red marrow in children |
| Periosteum | Covers all external bone surfaces except articular cartilage |
| Endosteum | Thin connective tissue layer lining all internal bone surfaces (marrow cavity walls, trabeculae, Haversian canals) |
Periosteum
The periosteum consists of two layers:
- Outer fibrous layer - dense irregular connective tissue; fibroblasts; continuous with joint capsule, tendons, and fascia; attached to bone by Sharpey's fibers (collagenous perforating fibers penetrating the cortex)
- Inner osteogenic (cambium) layer - contains osteoprogenitor cells, osteoblasts, blood vessels, and mesenchymal stem cells; the source of new bone during growth and fracture repair
In children: cambium is thick, vascular, and highly osteogenic. In adults: thin, less vascular, tightly adherent to cortex. The periosteum is critical for fracture healing and is the source of reactive periosteal new bone in osteomyelitis, tumors, and trauma.
Bone Matrix Composition
Inorganic phase (~65% dry weight):
- Hydroxyapatite [Ca₁₀(PO₄)₆(OH)₂] crystals - provide hardness and compressive strength
- Also: calcium carbonate, magnesium phosphate, calcium fluoride
Organic phase (~35% dry weight):
- Type I collagen (~90% of organic weight) - provides tensile strength and flexibility
- Noncollagenous proteins (~10%):
- Proteoglycans (chondroitin sulfate, keratan sulfate, hyaluronan) - compressive strength; osteoadherin binds hydroxyapatite
- Multiadhesive glycoproteins: osteonectin (bridges collagen to hydroxyapatite), osteopontin/BSP-1 (cell attachment), BSP-2 (initiates mineralization), fibronectin
- Vitamin K-dependent proteins: osteocalcin (calcium capture; attracts osteoclasts), matrix Gla-protein (MGP)
- Growth factors and cytokines: BMPs (uniquely induce osteoblast differentiation from mesenchyme), TGF-β, IGFs, PDGFs, interleukins, VEGF
Cells of Bone
1. Osteoprogenitor Cells
- Derived from mesenchymal stem cells
- Found in periosteum (inner layer), endosteum, and walls of Haversian canals
- Flat/spindle-shaped with pale-staining nuclei
- Give rise to osteoblasts when stimulated (by mechanical loading, fracture, BMPs, PTH)
2. Osteoblasts (Bone-forming cells)
- Large, polygonal, basophilic cytoplasm (abundant rER producing collagen and proteoglycans)
- Prominent Golgi apparatus; strong alkaline phosphatase activity on cell membrane
- Synthesize and secrete osteoid (unmineralized bone matrix = type I collagen + noncollagenous proteins)
- Osteoid is later mineralized by hydroxyapatite deposition (facilitated by matrix vesicles)
- Communicate with adjacent cells via gap junctions
- Fate: Only 10-20% become osteocytes; the rest undergo apoptosis or become bone-lining cells
3. Osteocytes (Most numerous bone cells)
- Former osteoblasts entrapped in their own mineralized matrix
- Occupy small cavities called lacunae
- Extend cytoplasmic processes through minute tunnels called canaliculi
- Neighboring osteocyte processes connect via gap junctions - forming a 3D communication network throughout bone
- Functions: maintain matrix viability; act as mechanosensors (sense mechanical deformation and signal via sclerostin, nitric oxide); regulate mineral homeostasis
4. Bone-Lining Cells
- Flat, inactive osteoblasts covering quiescent bone surfaces (periosteal and endosteal)
- Can be reactivated to become osteoblasts when needed
5. Osteoclasts (Bone-resorbing cells)
- Large, multinucleated (6-50 nuclei) giant cells
- Derived from fusion of hematopoietic progenitor cells (monocyte-macrophage lineage) - NOT from mesenchyme
- Located in shallow depressions called Howship's lacunae (resorption pits) on bone surfaces
- The membrane facing bone forms a ruffled border (highly folded = large surface area) surrounded by a clear zone (sealing zone) that isolates the resorption compartment
- Mechanism of resorption: secrete HCl (via H⁺-ATPase pump, aided by carbonic anhydrase II) to dissolve mineral + lysosomal enzymes (cathepsin K, MMP-9) to digest organic matrix
- Regulated by RANKL/RANK/OPG system: RANKL on osteoblast surface binds RANK on osteoclast precursors → osteoclast formation and activation; Osteoprotegerin (OPG) from osteoblasts acts as decoy receptor → inhibits osteoclastogenesis
Types of Bone Tissue
1. Compact (Cortical/Dense) Bone
Forms the outer shell of all bones; especially thick in the diaphysis.
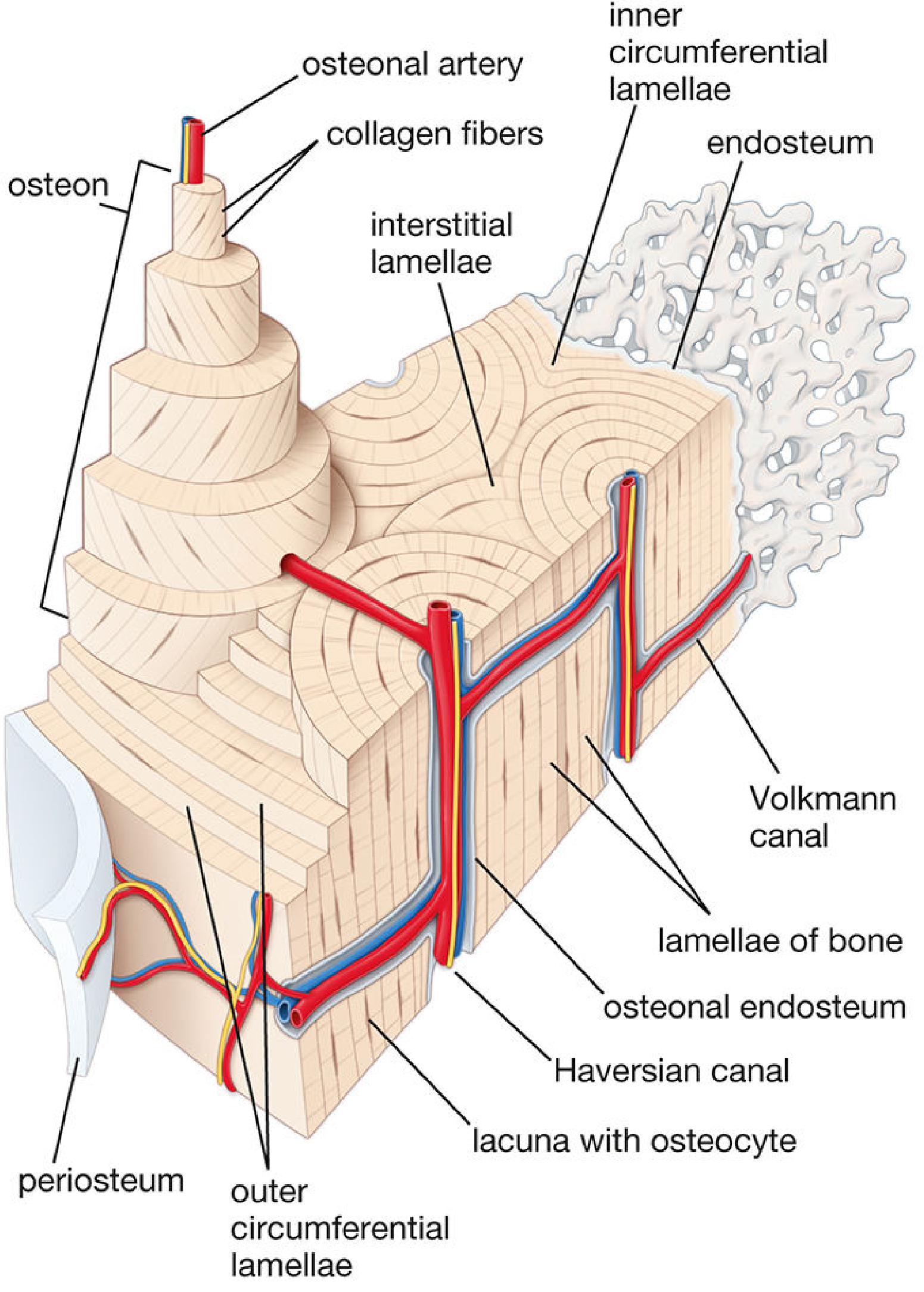
Structural unit = Osteon (Haversian system):
- Cylinder ~1 cm long, 250-350 μm diameter
- Central Haversian canal - contains arteriole, venule, nerve fibers, lymphatic vessel, and endosteum
- Surrounded by 5-20 concentric lamellae of mineralized matrix
- Osteocytes occupy lacunae between lamellae; their processes travel through canaliculi to reach the Haversian canal (source of nutrients)
- Collagen fibers in each lamella run parallel, but alternate in direction between adjacent lamellae (like plywood) - maximizes strength in multiple directions
Other lamellar systems in compact bone:
| Lamellar System | Location | Description |
|---|---|---|
| Osteons (Haversian systems) | Throughout compact bone | Cylindrical units; each has a central canal |
| Interstitial lamellae | Between osteons | Remnants of old osteons after remodeling |
| Outer circumferential lamellae | Outer (periosteal) surface of shaft | Several layers parallel to bone surface |
| Inner circumferential lamellae | Inner (endosteal) surface of shaft | Several layers facing medullary cavity |
Volkmann's (perforating) canals: Run transversely/obliquely, connecting Haversian canals to each other and to periosteal and endosteal vessels. Unlike Haversian canals, they have no surrounding concentric lamellae.
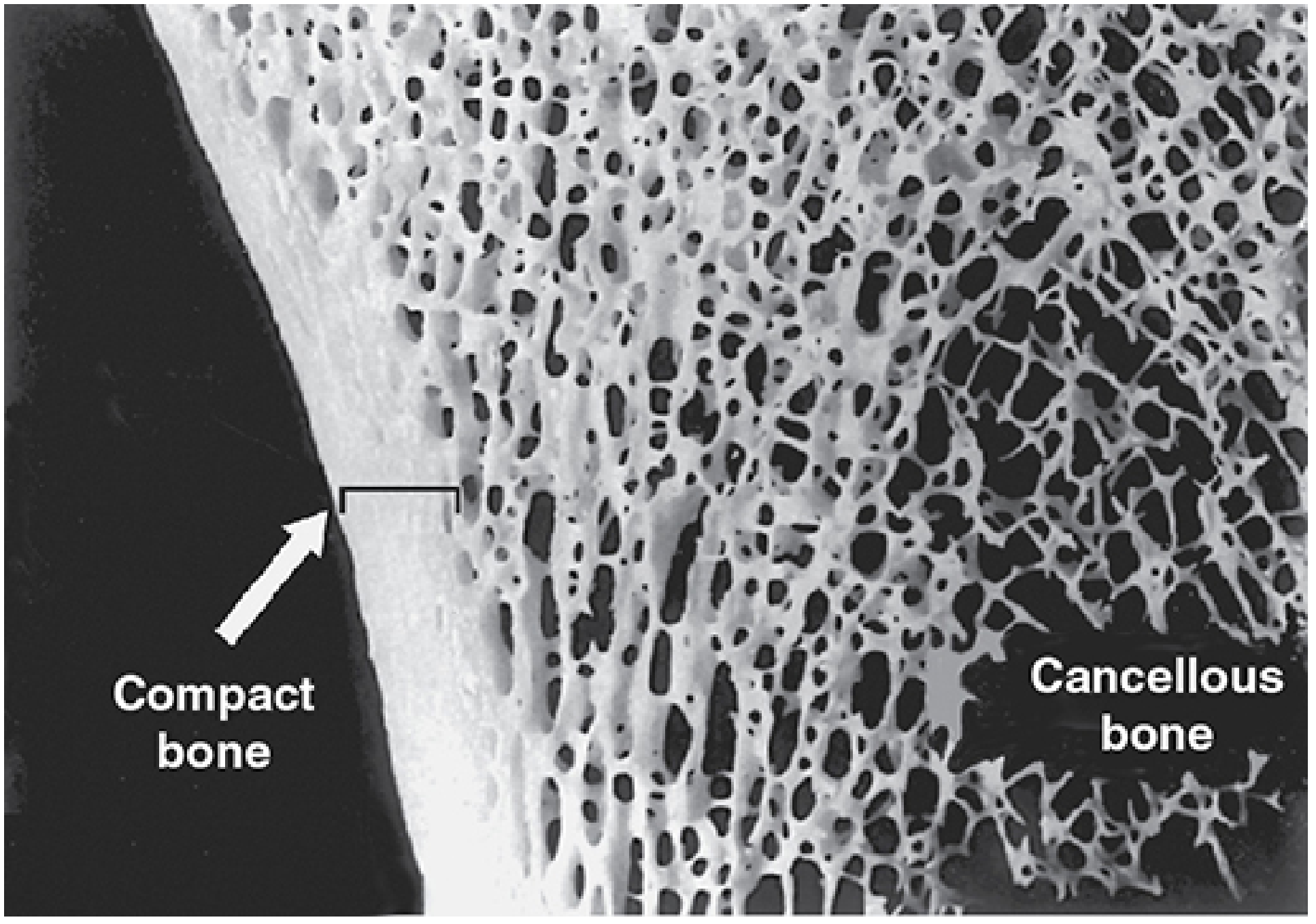
2. Spongy (Cancellous/Trabecular) Bone
- Found inside bones - predominantly at epiphyses, in flat bones, and surrounding the medullary cavity
- Consists of a 3D lattice of thin, anastomosing trabeculae separated by interconnecting marrow spaces
- Trabeculae are aligned along principal stress lines (Wolff's Law architecture)
- Trabeculae are ~200-300 μm thick - thin enough to be nourished by diffusion from adjacent marrow; they do not contain Haversian systems
- Spaces between trabeculae are filled with red bone marrow (hematopoietic) at active sites, or yellow marrow elsewhere
- Trabeculae are composed of lamellae with osteocytes in lacunae - same histology as compact bone but without osteons
Blood Supply of a Long Bone
- Nutrient artery - main supply; enters diaphysis through the nutrient foramen; divides into ascending and descending branches in the medullary cavity; supplies inner 2/3 of compact bone and marrow
- Periosteal vessels - supply outer 1/3 of compact bone; anastomose with Haversian/Volkmann canals
- Epiphyseal arteries - enter at the ends via small foramina; supply epiphyseal spongy bone
- Metaphyseal arteries - supply the metaphyses
PART III: OSSIFICATION (BONE FORMATION / OSTEOGENESIS)
Bone forms by two mechanisms:
1. Intramembranous (Membranous) Ossification
Bone forms directly from mesenchyme without any cartilage precursor.
Sequence:
- Mesenchyme condenses in a vascular membranous sheet
- Mesenchymal cells differentiate into osteoblasts (driven by Wnt signaling and RUNX2 transcription factor)
- Osteoblasts secrete osteoid (type I collagen matrix)
- Calcium phosphate deposits in osteoid → bone spicules form
- Osteoblasts trapped in matrix → become osteocytes
- Spicules coalesce → lamellae form → concentric lamellae around vessels → primary osteons
- Peripheral osteoblasts deposit compact bone plates on surfaces
- Intervening spongy bone persists; mesenchyme in interstices → red bone marrow
- Surrounding mesenchyme → periosteum
Bones formed by intramembranous ossification:
- Flat bones of skull vault (frontal, parietal, squamous temporal, squamous occipital)
- Mandible and maxilla
- Clavicle (predominantly)
2. Endochondral Ossification
Bone forms within a pre-existing hyaline cartilage model. This is how most bones of the body develop (all long bones, short bones, base of skull, vertebrae, pelvis, ribs).
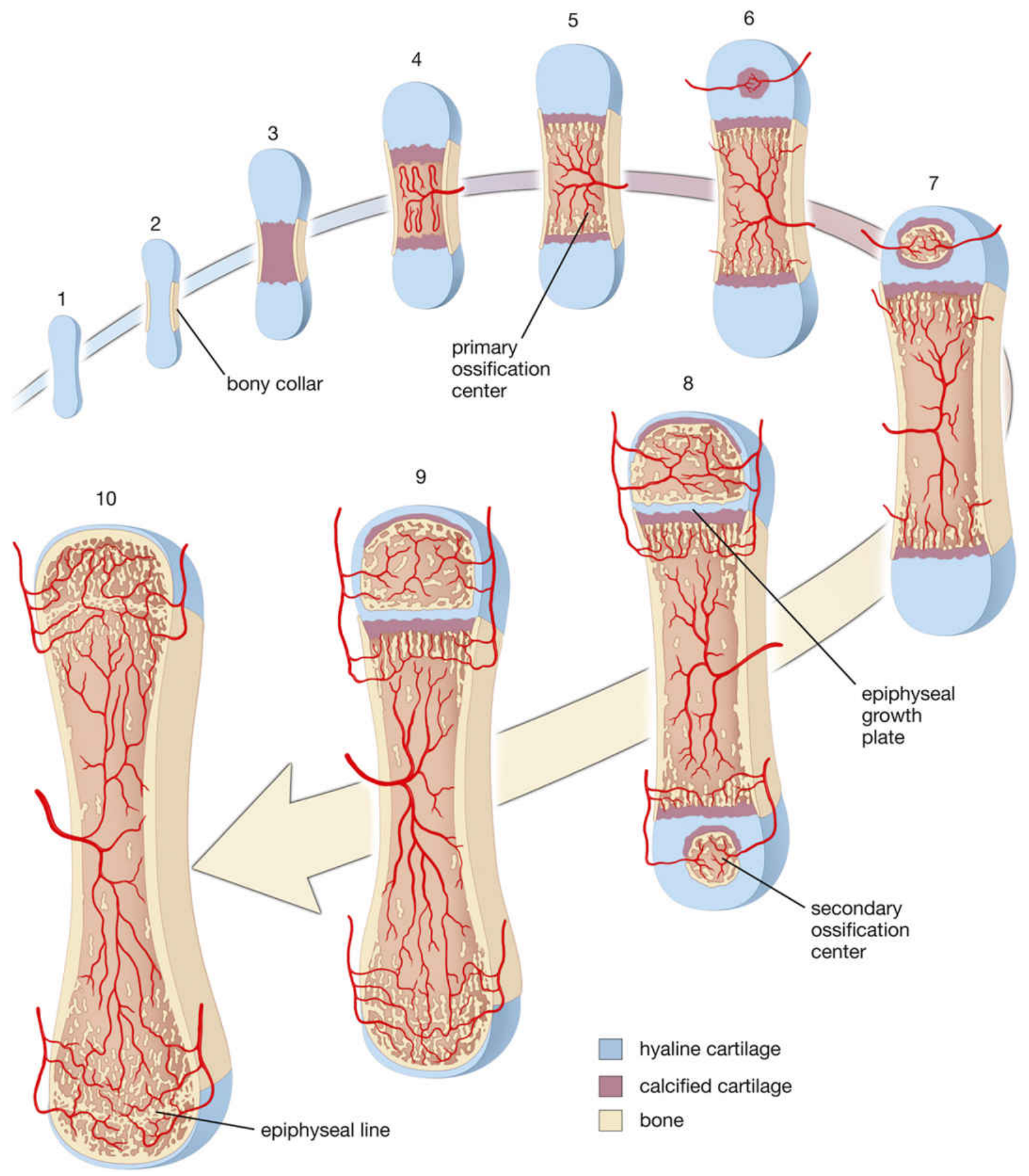
Sequence in a long bone:
Step 1 - Cartilage model: Mesenchyme condenses → chondroblasts form a hyaline cartilage model of the future bone surrounded by perichondrium
Step 2 - Chondrocyte hypertrophy: Chondrocytes in the shaft center enlarge (hypertrophy); lacunae enlarge; matrix calcifies; hypertrophic chondrocytes secrete VEGF (attracts vessels); cells die (apoptosis)
Step 3 - Bone collar: Osteoblasts in the periosteum deposit a bone collar around the diaphysis (by intramembranous ossification); perichondrium becomes periosteum
Step 4 - Vascular invasion + Primary Ossification Center: Blood vessels invade calcified cartilage bringing osteoprogenitor cells; osteoblasts deposit bone matrix on calcified cartilage remnants (forming spicules) → primary ossification center in the diaphysis (forms during fetal life, ~8th week for most long bones)
Step 5 - Medullary cavity: Osteoclasts resorb central spongy bone → medullary cavity forms; fills with red marrow
Step 6 - Secondary Ossification Centers: After birth, blood vessels invade the epiphyses → secondary ossification centers form in each epiphysis; cartilage replaced by bone from center outward
Step 7 - Epiphyseal plate: Disc of cartilage remains between primary and secondary ossification centers = epiphyseal plate (growth plate / physis) - responsible for longitudinal growth
Step 8 - Articular cartilage: Cartilage on the articular surface of each epiphysis is NEVER replaced → persists as articular cartilage throughout life
Step 9 - Epiphyseal closure (synostosis): Sex hormones at puberty cause the growth plate to be fully replaced by bone → epiphyseal line remains (visible on X-ray as a dense line)
Zones of the Epiphyseal Growth Plate
Reading from epiphysis toward diaphysis (i.e., the direction of bone growth):
| Zone | Key Features |
|---|---|
| Zone of resting (reserve) cartilage | Small, scattered chondrocytes; little proliferation; anchors the plate to the epiphysis; stores nutrients |
| Zone of proliferation | Chondrocytes divide rapidly by mitosis; arranged in longitudinal columns (coin-stack appearance); responsible for bone elongation |
| Zone of hypertrophy | Chondrocytes enlarge 5-10x; cytoplasm accumulates glycogen; matrix begins to calcify |
| Zone of calcification (provisional calcification) | Chondrocytes die (apoptosis); matrix calcifies; blood vessels invade from metaphysis; osteoblasts deposit bone on calcified cartilage spicules |
The width of the epiphyseal plate reflects bone growth rate. Growth hormone (via IGF-1) stimulates proliferation; sex hormones (estrogen, testosterone) drive plate closure.
Bone Remodeling
Adult bone undergoes continuous remodeling throughout life through coordinated cycles called Basic Multicellular Units (BMUs):
- Osteoclasts resorb old/damaged bone (creating a cutting cone in cortical bone or a resorption bay in trabecular bone)
- Osteoblasts deposit new bone in the resorbed space (filling with concentric lamellae in cortical bone)
- Cycle takes ~3-6 months; the process maintains bone strength and regulates mineral homeostasis
Wolff's Law: Bone architecture adapts to the mechanical loads placed upon it - trabeculae align along stress lines.
Hormonal regulation of bone remodeling:
| Hormone | Effect on Bone |
|---|---|
| PTH | Stimulates osteoclasts (raises serum Ca²⁺); also anabolic in intermittent dosing |
| Calcitonin | Inhibits osteoclasts; lowers serum Ca²⁺ |
| 1,25-(OH)₂ Vitamin D₃ | Promotes calcium absorption from gut; promotes mineralization |
| Estrogen | Inhibits osteoclastogenesis via OPG upregulation; loss → postmenopausal osteoporosis |
| Growth hormone / IGF-1 | Stimulates bone growth (epiphyseal plate) |
| Glucocorticoids (excess) | Inhibit osteoblasts, promote osteoclasts → steroid-induced osteoporosis |
| Thyroid hormones (excess) | Increase bone turnover → osteoporosis |
PART IV: DEVELOPMENT - MOLECULAR REGULATION
Key transcription factors and signaling molecules (Moore & Persaud, The Developing Human):
| Molecule | Role |
|---|---|
| RUNX2 (CBFA1) | Master transcription factor for osteoblast differentiation; required for all bone formation |
| SOX-9 | Master transcription factor for chondrocyte differentiation; triggers type II collagen expression |
| BMPs (2, 4, 7) | Induce differentiation of mesenchymal cells into osteoblasts and chondroblasts |
| Wnt/β-catenin | High β-catenin → osteoblast fate; low → chondrocyte fate |
| FGFR3 | Regulates chondrocyte proliferation in growth plate; gain-of-function mutations → achondroplasia |
| PTHrP | Produced by perichondrium; delays chondrocyte hypertrophy; keeps growth plate wide/active |
| VEGF | Produced by hypertrophic chondrocytes; drives vascular invasion into calcified cartilage |
| RANKL/OPG | Controls osteoclast formation and bone resorption |
Key developmental timelines:
- Cartilage formation begins: 5th embryonic week
- Intramembranous ossification (skull, mandible): 6th-7th embryonic week
- Primary ossification centers in long bones: ~8th fetal week onward
- Secondary ossification centers: mostly after birth (distal femur and proximal tibia are present at birth)
- Epiphyseal plate closure: puberty through early adulthood (~18-25 years; earlier in females)
PART V: CLINICAL CORRELATIONS
| Condition | Mechanism | Key Features |
|---|---|---|
| Osteoarthritis | Articular cartilage degeneration; poor repair due to avascularity | Progressive joint space loss; pain; subchondral sclerosis; osteophytes |
| Osteoporosis | Osteoclast activity > osteoblast activity; reduced bone mass | Fragility fractures (vertebral, hip, wrist); postmenopausal (estrogen loss) |
| Achondroplasia | Gain-of-function mutation in FGFR3 → inhibits growth plate chondrocyte proliferation | Rhizomelic short stature; normal trunk; normal intelligence; autosomal dominant |
| Rickets / Osteomalacia | Vitamin D deficiency → defective mineralization of osteoid | Wide growth plate (rickets); bowing of long bones; bone pain (osteomalacia) |
| Osteogenesis Imperfecta | Mutation in type I collagen genes (COL1A1, COL1A2) | Brittle bones; multiple fractures; blue sclerae; hearing loss |
| Paget's Disease | Uncontrolled osteoclast activity → disorganized remodeling | Mosaic (woven + lamellar) bone pattern on biopsy; elevated ALP; bone pain |
| Scurvy | Vitamin C deficiency → impaired collagen hydroxylation by osteoblasts | Weak osteoid; subperiosteal hemorrhage; perifollicular hemorrhage |
| Osteopetrosis | Osteoclast dysfunction (carbonic anhydrase II or chloride channel mutations) | Dense, brittle bone; obliterated medullary cavity; anemia; "marble bone" |
Sources:
- Gray's Anatomy for Students, 4th ed. (Drake, Vogl, Mitchell), pp. 28-30
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina), 8th ed., Chapters 7 & 8, pp. 548-600
- The Developing Human: Clinically Oriented Embryology (Moore & Persaud), 11th ed., Chapter 14, pp. 905-910
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy, Sections 1.8-1.9, pp. 36-60
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3, pp. 29-32
Bones it's classification ,types, Ossification, Blood supply
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed. Here is the complete, detailed topic:
BONES - Classification, Types, Ossification & Blood Supply
1. CLASSIFICATION OF BONES
Bones are classified by shape, internal structure (tissue type), and developmental origin.
A. Classification by Shape (Gross Anatomy)
| Type | Description | Examples |
|---|---|---|
| Long bones | Length > width; shaft (diaphysis) + two expanded ends (epiphyses) | Humerus, femur, tibia, fibula, radius, ulna, metacarpals, metatarsals, phalanges |
| Short bones | Roughly equal in all dimensions (cuboidal) | Carpal bones (wrist), tarsal bones (ankle) |
| Flat bones | Thin, plate-like; two layers of compact bone sandwiching spongy bone (diploë) | Skull vault (frontal, parietal), sternum, ribs, scapula, ilium |
| Irregular bones | Complex shape not fitting other categories; some contain air sinuses | Vertebrae, ethmoid, sphenoid, maxilla, facial bones |
| Sesamoid bones | Small; develop within tendons; reduce friction on tendon at bony surfaces | Patella (largest), sesamoids of thumb and big toe flexor tendons |
| Pneumatic bones | Contain air-filled cavities (sinuses) within their substance | Frontal, maxilla, ethmoid, sphenoid |
| Accessory (Wormian/sutural) bones | Supernumerary; result from failure of fusion of ossification centers | Found in calvarial sutures; os trigonum in foot |
B. Classification by Tissue Type (Histological)
| Type | % of Skeleton | Structure | Location |
|---|---|---|---|
| Compact (Cortical) bone | ~80% | Dense; structural units are osteons (Haversian systems); no visible spaces | Outer shell of all bones; thick in diaphysis of long bones |
| Spongy (Cancellous/Trabecular) bone | ~20% | Lattice of thin trabeculae; spaces filled with marrow | Interior of bones; predominates at epiphyses and inside flat bones |
Distribution in different bone shapes:
- Long bones: Diaphysis = thick compact cortex + medullary cavity (yellow marrow); Epiphyses = spongy bone + thin compact shell
- Short bones: Core of spongy bone completely surrounded by compact bone
- Flat bones: Two compact bone plates (outer + inner tables) separated by a layer of spongy bone called the diploë (e.g., skull vault)
C. Classification by Maturity / Collagen Arrangement
| Type | Also Called | Features | When Present |
|---|---|---|---|
| Woven (immature) bone | Bundle bone; primary bone | Collagen fibers randomly arranged; more cells per unit area; less mineralized; weaker | Fetal skeleton; fracture callus; bone tumors (Paget's) |
| Lamellar (mature) bone | Secondary bone | Collagen fibers in parallel sheets (lamellae) alternating in direction between layers (plywood effect); heavily mineralized; strong | All normal adult bone |
D. Classification by Developmental Origin
| Type | Method | Bones |
|---|---|---|
| Intramembranous bones | Form directly from mesenchyme | Flat bones of skull vault; mandible; maxilla; clavicle (mainly) |
| Endochondral bones | Form on a cartilage model | All long bones; short bones; vertebrae; ribs; base of skull; pelvis |
2. TYPES OF BONE TISSUE - DETAILED
Compact Bone and Its Structural Unit: The Osteon (Haversian System)
Mature compact bone is composed of cylindrical structural units called osteons (Haversian systems):
- Each osteon is ~1 cm long and 250-350 μm in diameter
- Central Haversian canal - contains an arteriole, venule, capillary, nerve fibers, and a thin sleeve of endosteum
- Surrounded by 5 to 20 concentric lamellae of mineralized matrix
- Osteocytes sit in lacunae between lamellae; their processes travel through canaliculi to reach the Haversian canal for nutrient exchange
- Collagen fibers within each lamella run parallel to each other but change direction in adjacent lamellae (like plywood), giving maximum resistance to stress in multiple directions
- The long axis of each osteon runs roughly parallel to the long axis of the bone
Other lamellar systems in compact bone:
| System | Location | Description |
|---|---|---|
| Outer circumferential lamellae | Beneath periosteum | Several lamellae paralleling the outer bone surface; like tree growth rings |
| Inner circumferential lamellae | Adjacent to endosteum | Several lamellae paralleling the medullary cavity surface |
| Interstitial lamellae | Between osteons | Irregular angular remnants of old, partially resorbed osteons from previous remodeling cycles |
| Volkmann (perforating) canals | Run transversely/obliquely through compact bone | Connect Haversian canals to each other and to periosteal and endosteal vessels; no concentric lamellae around them (distinguishes them from Haversian canals) |
Spongy Bone
- Three-dimensional lattice of thin, anastomosing trabeculae separated by interconnecting spaces filled with bone marrow
- Trabeculae are oriented along principal lines of mechanical stress (Wolff's Law)
- Trabeculae are ~200-300 μm thick - thin enough to be nourished by diffusion from adjacent marrow; they do NOT contain Haversian systems
- Trabeculae consist of lamellae with osteocytes in lacunae and canaliculi - same histology as compact bone at the microscopic level, just without osteons
- Covered on all surfaces by endosteum
3. OSSIFICATION (OSTEOGENESIS)
Bone is formed by two fundamentally different mechanisms:
A. Intramembranous Ossification
"Bone forms directly from mesenchyme with NO cartilage intermediate"
Sites: Flat bones of skull vault (frontal, parietal, squamous temporal, squamous occipital), mandible, maxilla, clavicle
Step-by-step process:
| Step | Event |
|---|---|
| 1 | Mesenchymal cells migrate and aggregate in a specific region, forming an ossification center within a vascular membranous sheet |
| 2 | Mesenchymal cells elongate and express CBFA1 (RUNX2) transcription factor → differentiate into osteoprogenitor cells → osteoblasts (cytoplasm changes from eosinophilic to basophilic; Golgi becomes prominent) |
| 3 | Osteoblasts secrete osteoid (type I collagen + noncollagenous proteins) |
| 4 | Osteoid undergoes mineralization (hydroxyapatite deposition) |
| 5 | Osteoblasts trapped in mineralizing matrix → become osteocytes in lacunae; cytoplasmic processes persist in canaliculi |
| 6 | More osteoprogenitor cells → osteoblasts → appositional growth; spicules enlarge and fuse into a trabecular network (woven bone) |
| 7 | Concentric lamellae deposit around blood vessels → primary osteons |
| 8 | Peripheral osteoblasts deposit plates of compact bone on outer surfaces; central region remains as spongy bone |
| 9 | Mesenchyme in the interstices → red bone marrow; surrounding mesenchyme → periosteum |
B. Endochondral Ossification
"Bone forms within a pre-existing hyaline cartilage model"
Sites: ALL long bones, short bones, vertebrae, ribs, pelvic bones, base of skull - the majority of the skeleton
Step-by-step process:
| Step | Event | Timing |
|---|---|---|
| 1. Cartilage model | Mesenchymal cells condense → differentiate into chondroblasts → form a hyaline cartilage model of the future bone surrounded by perichondrium | ~5th-6th week embryonic |
| 2. Cartilage growth | Model grows by interstitial (length) and appositional (width) growth | 6th-8th week |
| 3. Bone collar | Perichondrial cells in the mid-diaphysis stop producing chondrocytes and instead produce osteoblasts → a bony collar (periosteal bone) forms around the cartilage diaphysis by intramembranous ossification; perichondrium becomes periosteum | ~8th week |
| 4. Chondrocyte hypertrophy | The bone collar impedes nutrient diffusion → chondrocytes in the center hypertrophy, compress matrix, release osteocalcin and alkaline phosphatase → matrix calcifies; hypertrophic chondrocytes also secrete VEGF (vascular invasion signal) and undergo apoptosis | |
| 5. Vascular invasion + Primary Ossification Center | Blood vessels + osteoprogenitor cells from periosteum invade calcified cartilage; osteoblasts deposit bone matrix on calcified cartilage spicules (basophilic cartilage remnant + acidophilic new bone = characteristic histological picture) → PRIMARY OSSIFICATION CENTER forms in diaphysis | Fetal life (~8th week most long bones) |
| 6. Medullary cavity | Osteoclasts resorb central spongy bone → medullary cavity forms; fills with red bone marrow | |
| 7. Secondary Ossification Centers | Blood vessels invade epiphyses → SECONDARY OSSIFICATION CENTERS form in each epiphysis (bone replaces cartilage from center outward) | Mostly after birth; distal femur + proximal tibia = present at birth |
| 8. Epiphyseal plate | A disc of hyaline cartilage persists between primary and secondary ossification centers = EPIPHYSEAL PLATE (GROWTH PLATE / PHYSIS) → responsible for longitudinal bone growth throughout childhood | |
| 9. Articular cartilage | Cartilage on the articular surface of each epiphysis is never replaced → persists as articular cartilage throughout life | |
| 10. Epiphyseal closure (Synostosis) | When growth ceases (driven by sex hormones at puberty), the growth plate is fully replaced by bone → EPIPHYSEAL LINE (dense line visible on X-ray) remains | ~18-25 yrs; earlier in females |
Zones of the Epiphyseal Growth Plate
(Reading from epiphysis → diaphysis, i.e., the direction of bone growth)
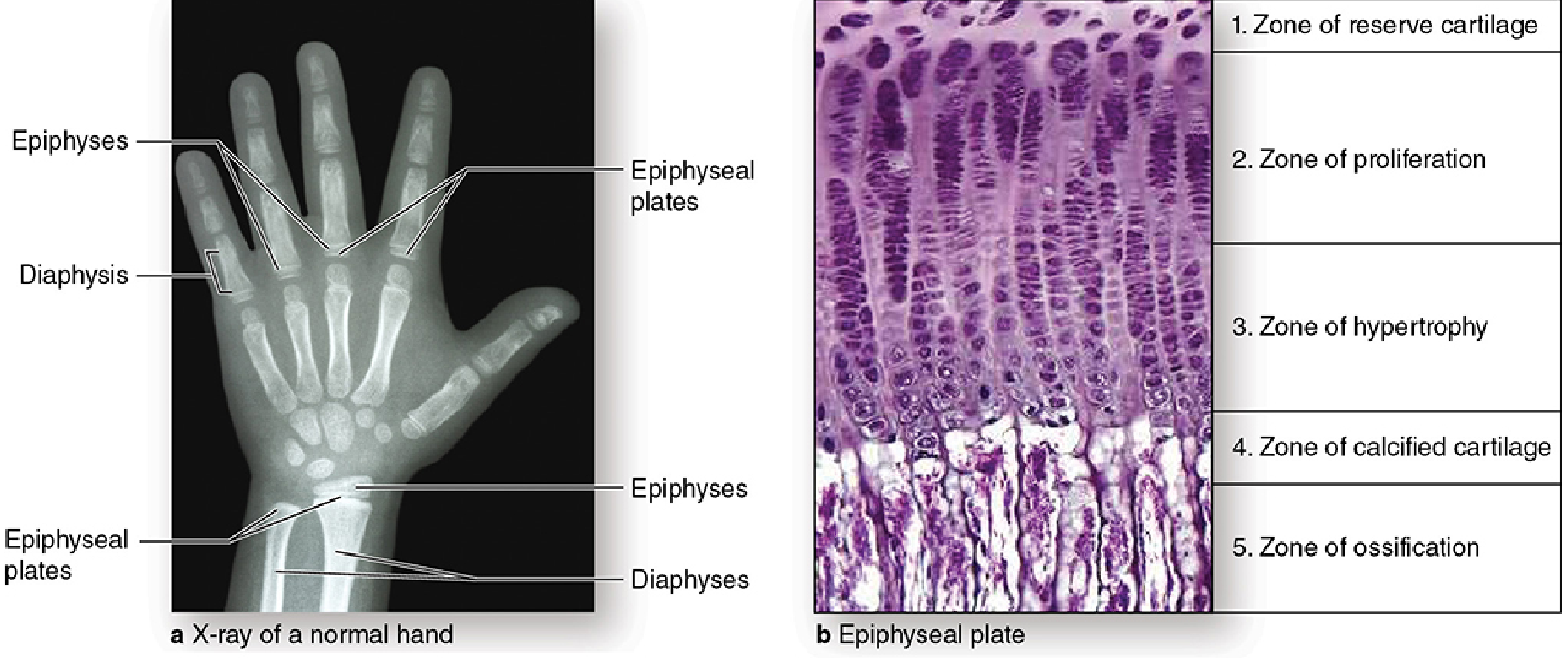
| Zone | What Happens | Key Features |
|---|---|---|
| 1. Zone of Reserve (Resting) Cartilage | Normal hyaline cartilage; few cells | Stores nutrients; anchors plate to epiphysis; no active division |
| 2. Zone of Proliferation | Chondrocytes divide rapidly by mitosis; stack in longitudinal columns (coin-stack/stacked-coin appearance) | Responsible for bone lengthening; produce type II collagen + proteoglycans; largest zone |
| 3. Zone of Hypertrophy | Chondrocytes swell 5-10x normal size; cytoplasm fills with glycogen; matrix compresses into aligned spicules | Secrete type X collagen (unique to this zone); stiffens matrix; promotes vascularization |
| 4. Zone of Calcified Cartilage | Chondrocytes undergo apoptosis; release matrix vesicles + osteocalcin → hydroxyapatite crystals form → matrix calcifies | "Tidemark" separates zones 3 and 4; vascular invasion begins |
| 5. Zone of Ossification (Resorption) | Capillaries and osteoprogenitor cells invade from metaphysis; osteoblasts deposit osteoid on calcified cartilage spicules → woven bone → remodeled to lamellar bone | Merges with primary spongiosa of metaphysis |
Key rules about the growth plate:
- The thickness of the plate stays constant during active growth because the rate of new cartilage production (zone 2) equals the rate of resorption (zone 5)
- Bone lengthening occurs when new cartilage matrix in zone 2 pushes the epiphysis away from the diaphysis
- GH/IGF-1 stimulates chondrocyte proliferation; sex hormones (estrogen > testosterone) drive epiphyseal closure
Clinical note - Growth plate fractures (Salter-Harris classification): The weakest zone is between the zone of hypertrophy and zone of calcified cartilage - most growth plate fractures propagate through this area.
4. BLOOD SUPPLY OF BONE
Blood supply to a long bone comes from three main sources, which anastomose freely:
Sources of Blood Supply
LONG BONE - BLOOD SUPPLY
┌───────────────────────────────────────────────────┐
│ EPIPHYSEAL ARTERIES ──────► Epiphysis │
│ (enter via small foramina at bone ends) │
│ │
│ ────── Epiphyseal growth plate ────── │
│ │
│ METAPHYSEAL ARTERIES ─────► Metaphysis │
│ (from periosteal vessels incorporated into │
│ metaphysis during growth) │
│ │
│ NUTRIENT ARTERY ──────────► Diaphysis │
│ (enters via nutrient foramen → medullary │
│ cavity → ascending + descending branches) │
│ │
│ PERIOSTEAL ARTERIES ──────► Outer cortex │
│ (from surrounding soft tissue) │
└───────────────────────────────────────────────────┘
| Vessel | Origin | Area Supplied | Notes |
|---|---|---|---|
| Nutrient artery (1 or 2) | Nearest regional artery | Inner 2/3 of compact bone; entire marrow cavity (diaphysis + metaphysis) | Enters via the nutrient foramen in the diaphysis; divides into ascending + descending branches in medullary cavity; developmentally, these are the principal vessels of the periosteal bud |
| Epiphyseal arteries | Regional arteries near the joint | Spongy bone of the epiphysis | Enter via multiple small foramina at the ends of the bone; in children, separated from metaphyseal supply by the avascular growth plate |
| Metaphyseal arteries | Periosteal vessels incorporated during growth | Metaphyseal spongy bone; contribute to adjacent marrow | Arise from periosteal vessels that become incorporated into the metaphysis as bone widens during growth |
| Periosteal arteries | Surrounding muscular and connective tissue vessels | Outer 1/3 of compact bone; periosteum | Enter Haversian canals via Volkmann's canals; provide a lesser contribution than the nutrient/medullary system |
Direction of Blood Flow Within Bone (Centrifugal Flow)
Blood flow through bone tissue is centrifugal (inside → outside):
Nutrient artery → Medullary cavity → Haversian canals (via Volkmann's canals) → Periosteal veins
Specifically:
- The nutrient artery enters the medullary cavity and branches into the sinusoidal network of marrow
- From the marrow, blood passes into the cortical bone via Volkmann's canals (the major entry route for cortical bone)
- From Volkmann's canals, blood enters the Haversian canals of individual osteons
- The Haversian canal contains a single arteriole + venule (or a capillary)
- Osteocytes in lacunae are nourished by diffusion through the canalicular network from the Haversian canal
- Blood exits via periosteal veins
- Bone lacks lymphatic vessels - lymphatic drainage occurs only from the periosteum
Clinical Significance of Bone Blood Supply
| Situation | Clinical Relevance |
|---|---|
| Nutrient artery disruption (e.g., femoral neck fracture) | Avascular necrosis (osteonecrosis) of the femoral head - especially in intracapsular fractures where the retinacular vessels are torn |
| Growth plate avascularity | The growth plate itself is avascular → chondrocytes nourished by diffusion from metaphyseal vessels; this makes the growth plate a site where bacteria can lodge during hematogenous osteomyelitis in children (especially at the metaphysis just below the plate) |
| Periosteal stripping | Disrupts periosteal blood supply → impairs fracture healing; also seen in surgical approaches |
| Scaphoid fractures | The scaphoid bone has a precarious blood supply entering distally → proximal pole fractures deprive the proximal fragment → avascular necrosis |
| Fracture healing | Initial hematoma is organized; the periosteum (outer fibrous + inner osteogenic layers) and endosteum both contribute to the healing process - periosteal cells produce external callus (soft callus → hard callus) |
Nerve Supply of Bone
- Nerves accompany blood vessels through Haversian and Volkmann canals
- Periosteum is richly innervated (sensory and vasomotor fibers) → accounts for the severe pain of periosteal elevation, fracture, and infection
- Cortical bone and marrow have fewer nerve endings
SUMMARY TABLE
| Topic | Key Points |
|---|---|
| Shapes | Long, short, flat, irregular, sesamoid, pneumatic, accessory |
| Tissue types | Compact (80%, osteons) vs Spongy (20%, trabeculae) |
| Histological maturity | Woven (immature, random collagen) vs Lamellar (mature, organized lamellae) |
| Intramembranous ossification | Direct mesenchyme → bone; skull vault, mandible, maxilla, clavicle |
| Endochondral ossification | Cartilage model → bone; most bones; primary center (fetal) → secondary center (postnatal) |
| Growth plate zones | Reserve → Proliferation → Hypertrophy → Calcification → Ossification (from epiphysis to diaphysis) |
| Blood supply | Nutrient artery (main), epiphyseal arteries, metaphyseal arteries, periosteal arteries; flow is centrifugal |
| Epiphyseal closure | Sex hormones → ~18-25 years; earlier in females; leaves epiphyseal line on X-ray |
Sources:
- Junqueira's Basic Histology: Text and Atlas, 17e, Chapter 8
- Histology: A Text and Atlas (Ross & Pawlina), 8th ed., Chapter 8
- The Developing Human (Moore & Persaud), 11th ed., Chapter 14
- General Anatomy and Musculoskeletal System, THIEME Atlas, Sections 1.8-1.9
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.