Cardinal symptoms of digestive system
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have excellent content from Goldman-Cecil Medicine and Yamada's Gastroenterology. Let me compile the full answer.
Cardinal Symptoms of the Digestive System
GI conditions manifest with a limited number of symptoms and signs, including abdominal pain, heartburn, dysphagia, dyspepsia, nausea, vomiting, gas and bloating, weight loss, diarrhea, constipation, incontinence, and acute or chronic bleeding. - Goldman-Cecil Medicine, p. 1361
Below is a structured breakdown of each cardinal symptom:
1. Abdominal Pain
The most common GI complaint. Key features to characterize:
- Acuity - acute (minutes to hours, may need surgery) vs. chronic/intermittent
- Location and radiation - correlates strongly with the organ involved
- Pattern - steady vs. colicky; abrupt vs. gradual
- Relationship to food and bowel movements - GI symptoms are almost always improved or worsened by eating or bowel movements
- Associated symptoms - vomiting, hematemesis, diarrhea, melena, constipation, jaundice
Severe or dramatic abdominal pain developing acutely requires urgent evaluation to rule out a surgical emergency. Serum amylase and lipase are obtained when pancreatitis is suspected. - Goldman-Cecil Medicine, p. 1360
Common causes by location:
- Epigastric: peptic ulcer, pancreatitis, GERD, gastritis
- Right upper quadrant (RUQ): gallbladder disease, hepatitis
- Right lower quadrant (RLQ): appendicitis, Crohn disease, ovarian pathology
- Left lower quadrant (LLQ): diverticulitis, sigmoid disease
- Periumbilical: early appendicitis, small bowel disease
- Diffuse: peritonitis, IBS, mesenteric ischemia
2. Heartburn (Pyrosis)
A burning retrosternal discomfort caused by reflux of gastric acid into the esophagus. It is the hallmark of gastroesophageal reflux disease (GERD) and typically worsens after meals, when lying down, or with bending. May be accompanied by regurgitation (sour/acid taste in the mouth).
3. Dysphagia
Difficulty swallowing. Two main types:
| Type | Characteristics | Common Causes |
|---|---|---|
| Oropharyngeal | Difficulty initiating the swallow, coughing/nasal regurgitation, neurological cause | Stroke, Parkinson disease, myasthenia gravis |
| Esophageal | Sensation of food sticking in the chest after swallowing | Stricture, achalasia, esophageal cancer, eosinophilic esophagitis |
- Progressive dysphagia to solids only suggests mechanical obstruction (e.g., cancer)
- Dysphagia to both solids and liquids from the outset suggests a motility disorder (e.g., achalasia)
- Odynophagia (pain on swallowing) suggests esophageal ulceration or infection
4. Dyspepsia
Upper abdominal discomfort or pain, often with bloating, early satiety, nausea, or belching. Key differential includes:
- Peptic ulcer disease
- Gastritis (H. pylori-associated)
- Gastroparesis
- Functional (non-ulcer) dyspepsia - the most common cause
- GERD (heartburn-predominant)
Medications are a frequent cause - NSAIDs, aspirin, antibiotics, and iron supplements are common culprits. - Goldman-Cecil Medicine, p. 1356
5. Nausea and Vomiting
A highly non-specific symptom with both GI and non-GI causes.
GI causes include:
- Gastroenteritis (most common acute cause)
- Peptic ulcer disease / gastritis
- Gastroparesis (delayed gastric emptying, commonly in diabetes)
- Intestinal obstruction
- Hepatitis, cholecystitis, pancreatitis
- Appendicitis
Non-GI causes to exclude:
- Pregnancy, medications (opioids, chemotherapy, antibiotics), raised intracranial pressure, metabolic disturbances (uraemia, DKA), labyrinthine disorders, MI
Severe vomiting or diarrhea with signs of dehydration warrants urgent attention. - Goldman-Cecil Medicine, p. 1360
Hematemesis (vomiting blood) is a specific alarming variant indicating upper GI bleeding - from peptic ulcer, variceal hemorrhage, Mallory-Weiss tear, or esophagitis.
6. Gas and Bloating
Subjective sensation of abdominal fullness, distension, or excess gas. Causes include:
- Swallowed air (aerophagia)
- Lactose intolerance / carbohydrate malabsorption
- Small intestinal bacterial overgrowth (SIBO)
- IBS
- Celiac disease / malabsorption syndromes
A low-fiber diet is associated with constipation and bloating; dairy products (lactose), legumes, and cruciferous vegetables may cause pain, flatulence, and diarrhea in susceptible individuals. - Goldman-Cecil Medicine, p. 1361
7. Diarrhea
Passage of loose, watery, or frequent stools. Classified as:
| Category | Duration | Mechanism Examples |
|---|---|---|
| Acute | <2 weeks | Infectious gastroenteritis, food poisoning, medications |
| Chronic | >4 weeks | IBD, IBS, celiac disease, malabsorption, microscopic colitis |
Pathophysiologic mechanisms:
- Secretory - watery, large volume, persists with fasting (e.g., cholera, VIPoma)
- Osmotic - stops with fasting (e.g., lactose intolerance, laxative use)
- Inflammatory - blood/mucus/pus in stool (IBD, infectious colitis)
- Motility-related - IBS, hyperthyroidism, post-vagotomy
Alarm features (red flags): blood in stool, nocturnal diarrhea, weight loss, age >50, fever, family history of IBD or colorectal cancer.
8. Constipation
Infrequent or difficult evacuation of stool. Features include: fewer than 3 bowel movements/week, straining, hard stools, sensation of incomplete evacuation, or need for manual maneuvers.
Causes:
- Low-fiber diet, inadequate fluid intake
- Medications: opioids, anticholinergics, iron, calcium channel blockers
- Hypothyroidism, hypercalcemia, diabetes
- Structural: colorectal cancer (new-onset constipation in older adult is a red flag), stricture
- Functional: IBS-C, dyssynergic defecation
Improvement in symptoms after passage of flatus or bowel movement suggests a disorder of the colon or anorectum. - Goldman-Cecil Medicine, p. 1361
9. GI Bleeding
| Presentation | Location | Typical Causes |
|---|---|---|
| Hematemesis (vomiting blood) | Upper GI (above ligament of Treitz) | Peptic ulcer, varices, Mallory-Weiss tear |
| Melena (black, tarry stools) | Upper GI or proximal small bowel | Same as above; also Meckel diverticulum |
| Hematochezia (bright red blood per rectum) | Lower GI (usually colon/anorectal) | Hemorrhoids, diverticulosis, colitis, colorectal cancer |
| Occult bleeding | Any site | Detected on fecal occult blood testing |
Acute symptoms requiring urgent assessment are severe abdominal pain and overt GI bleeding manifested by hematemesis, melena, or large-volume hematochezia. - Goldman-Cecil Medicine, p. 1360
10. Jaundice
Yellow discoloration of the skin, sclera, and mucous membranes due to elevated serum bilirubin (>2.5-3 mg/dL). Classified as:
- Pre-hepatic - hemolysis (unconjugated hyperbilirubinemia)
- Hepatic (hepatocellular) - hepatitis, cirrhosis, drug-induced liver injury
- Post-hepatic (obstructive/cholestatic) - gallstones, pancreatic cancer, cholangiocarcinoma, primary sclerosing cholangitis
Associated features: dark urine (conjugated bilirubinuria), pale/acholic stools (biliary obstruction), pruritus.
11. Weight Loss
Involuntary loss of >5% of body weight in 12 months is worrisome for serious disease. GI causes include:
- Malabsorption (celiac disease, Crohn disease, short bowel syndrome)
- Malignancy (gastric, pancreatic, colorectal cancer)
- Chronic inflammation (IBD)
- Dysphagia preventing adequate intake
12. Fecal Incontinence
Loss of voluntary control of bowel movements. Often under-reported by patients. Causes include sphincter damage (obstetric injury, surgery), neuropathy (diabetes), rectal prolapse, and severe diarrhea.
Summary Table: Cardinal GI Symptoms
| Symptom | Key Mechanism | Alarm Features |
|---|---|---|
| Abdominal pain | Variable | Acute severe onset, peritoneal signs, fever |
| Heartburn | Acid reflux | Dysphagia, weight loss, hematemesis |
| Dysphagia | Obstruction or dysmotility | Progressive, weight loss |
| Dyspepsia | Ulcer, motility, functional | >50 yrs, weight loss, bleeding |
| Nausea/vomiting | Multiple | Hematemesis, severe dehydration |
| Gas/bloating | Fermentation, malabsorption | Weight loss, steatorrhea |
| Diarrhea | Infectious, inflammatory, secretory | Blood, nocturnal, weight loss |
| Constipation | Functional, structural, drugs | New onset >50 yrs, blood, weight loss |
| GI bleeding | Mucosal damage, vascular | Hemodynamic instability |
| Jaundice | Bilirubin metabolism | Painless (cancer), fever (cholangitis) |
| Weight loss | Malabsorption, malignancy | Always an alarm feature |
| Incontinence | Sphincter/neurologic | Quality of life, anatomic defect |
Sources: Goldman-Cecil Medicine (International Edition), p. 1360-1362; Yamada's Textbook of Gastroenterology, 7th ed.
Explain the importance of USG in diagnosis of different diseases of digestive system
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have rich textbook content and real USG images. Here is the comprehensive answer:
Importance of Ultrasound (USG) in Diagnosis of Digestive System Diseases
Ultrasound is the first-line imaging modality for most abdominal GI complaints. It uses high-frequency sound waves (2-13 MHz) to generate real-time images, and is preferred because it is:
- Non-ionizing (no radiation)
- Widely available and low-cost
- Portable (can be used in critically ill, bedside patients)
- Allows real-time dynamic assessment and Doppler flow evaluation
- Can guide interventional procedures (drainage, biopsy)
Its main limitation is that intraluminal air causes acoustic artifact, reducing its utility for hollow viscera like the bowel. - Yamada's Textbook of Gastroenterology, 7th ed.
1. Gallbladder and Biliary System - The Domain Where USG Excels
Cholelithiasis (Gallstones)
USG is the method of choice for gallstone detection, with sensitivity and specificity >90-95%.
- Gallstones appear as echogenic (bright) foci that cast a posterior acoustic shadow (sound waves cannot penetrate the stone)
- Stones are mobile - they shift to a dependent position when the patient is repositioned
- This distinguishes them from polyps (which do not move) and sludge (which shifts slowly)
- USG can also differentiate cholelithiasis from gallbladder sludge, polyps, and masses - Goldman-Cecil Medicine, p. 1381
Acute Cholecystitis
USG has sensitivity 85%, specificity 95% for acute cholecystitis. Findings include:
- Presence of gallstones
- Gallbladder wall thickening (>3 mm)
- Pericholecystic fluid
- Gallbladder distension
- Sonographic Murphy's sign - focal tenderness directly elicited by pressing the probe over the fundus of the gallbladder - Schwartz's Principles of Surgery, 11th ed.
Acalculous Cholecystitis
In critically ill patients without stones, USG shows a large, tense, static gallbladder without stones with evidence of wall thickening or pericholecystic fluid. - Harrison's Principles of Internal Medicine, 22nd ed.
Chronic Cholecystitis
A contracted, thick-walled gallbladder on USG is indicative of chronic cholecystitis. - Schwartz's Principles of Surgery
Biliary Ductal Dilation / Obstructive Jaundice
- Extrahepatic bile ducts are well-visualized by USG (except the retroduodenal portion)
- Biliary ductal dilation in a jaundiced patient points toward extrahepatic (mechanical) obstruction
- The level and often the cause of obstruction can be identified: gallstones, strictures, or peri-ampullary masses
- A dilated CBD + small gallbladder stones + clinical presentation allows diagnosis of choledocholithiasis even if the stone is not directly visualized
- USG can also assess tumor invasion of the portal vein - important for resectability of periampullary tumors - Schwartz's Principles of Surgery, 11th ed.
2. Liver Diseases
USG is useful to evaluate the liver's size, morphology, and echotexture and to assess for diffuse or focal hepatic processes. - Goldman-Cecil Medicine
Cirrhosis
- Liver appears echogenic, heterogeneous, and nodular in contour
- Associated findings of portal hypertension: splenomegaly, ascites, and collateral vessels (varices)
- Doppler USG can assess blood flow through the portal and hepatic vessels - detects portal vein thrombosis and hepatofugal (reversed) flow
- Splenomegaly and ascites on USG provide indirect evidence of severity - Goldman-Cecil Medicine, p. 1381
Hepatic Masses - Cyst vs. Solid Lesion
USG readily distinguishes a cystic from a solid hepatic mass:
- Simple cysts appear as anechoic (black) fluid-filled structures with posterior acoustic enhancement
- Solid lesions (metastases, HCC, hepatic adenoma) show echogenic characteristics
- Contrast-enhanced USG (CEUS): IV injection of microbubble contrast allows lesion characterization (arterial enhancement pattern) comparable to CT/MRI in some cases
- CT and MRI are superior for full characterization, but USG is the entry-point imaging - Goldman-Cecil Medicine
Focal Hepatic Lesions - Systematic USG Approach
Using the hepatic veins and portal vein branches as landmarks (Brisbane 2000 Terminology), intraoperative USG allows:
- Identification of hepatic veins and their junctions
- Identification of portal vein branches
- Systematic parenchymal sweep - locating lesions by segment and defining vascular involvement
This is used during liver surgery for precise tumor localization and planning resection margins - Fischer's Mastery of Surgery, 8th ed.
Hepatic Abscess
USG detects hepatic abscesses as hypoechoic or heterogeneous collections and can guide percutaneous drainage.
3. Pancreas
Acute Pancreatitis
- USG features include diffuse enlargement, heterogeneity, and hypoechogenicity of the pancreatic parenchyma
- A right upper quadrant USG is mandatory in all acute pancreatitis to evaluate for gallstone etiology (biliary pancreatitis)
- USG may be used as an adjunct to monitor complications (peripancreatic fluid collections) and limit radiation vs. CT
- Doppler USG identifies vascular complications: splenic or portal vein thrombosis, splenic artery aneurysm
- USG can guide drainage of peripancreatic fluid collections - Yamada's Gastroenterology, 7th ed.
Overlying bowel gas often limits pancreatic visualization; CT is the preferred modality for evaluating necrosis and complications. - Goldman-Cecil Medicine
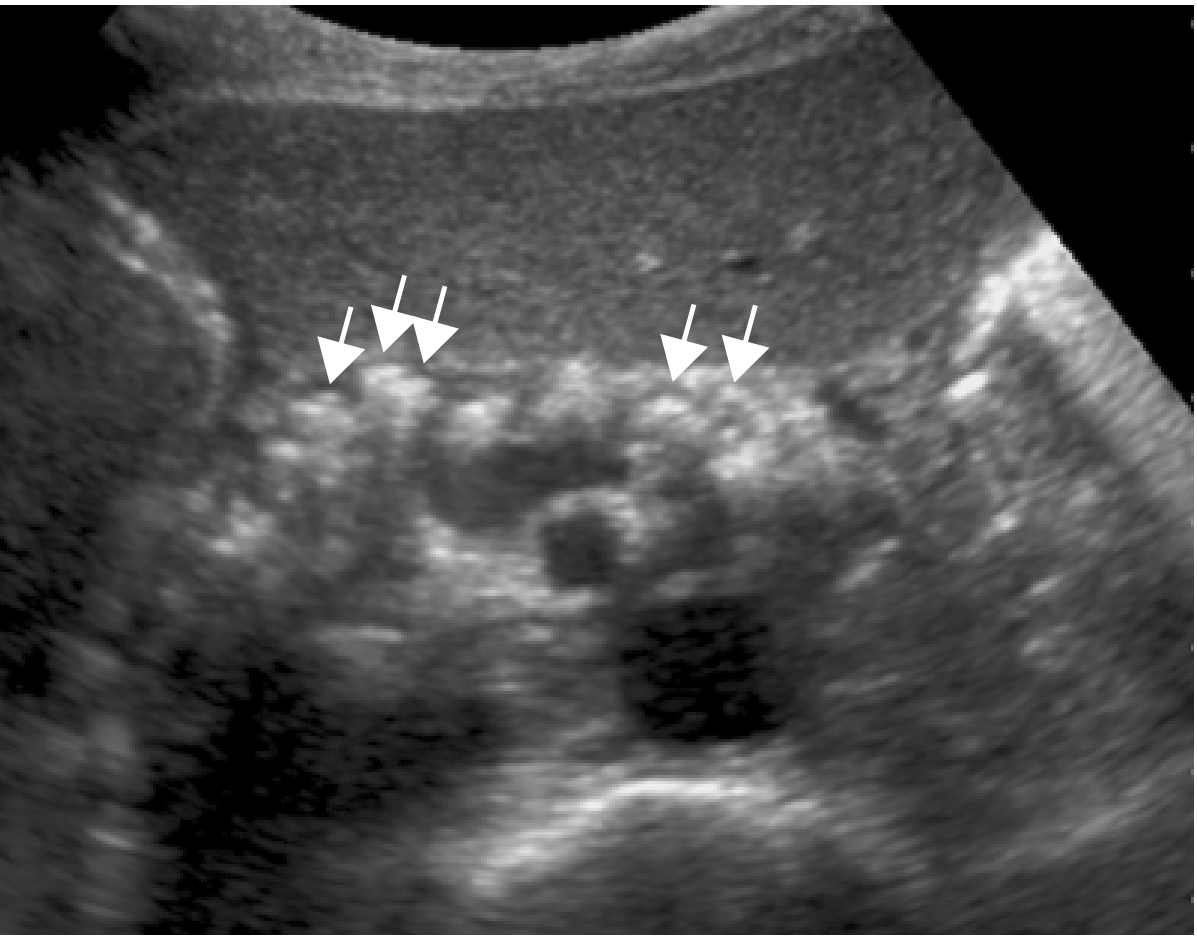
Chronic Pancreatitis
USG findings: pancreatic atrophy, pancreatic ductal dilation, and parenchymal calcifications (shown as bright echogenic foci). An abrupt duct cutoff or isolated cluster of calcifications raises suspicion for pancreatic adenocarcinoma superimposed on chronic pancreatitis.
Pancreatic Tumors
- Pancreatic adenocarcinoma: Focal hypoechoic mass, with possible common bile duct and pancreatic duct dilation ("double duct sign"). USG assesses patency of superior mesenteric, splenic, and portal vessels for resectability.
- Islet cell tumors (insulinoma/gastrinoma): Hypoechoic masses, 20% contain calcification
- Cystic pancreatic neoplasms:
- Mucinous cystadenoma/cystadenocarcinoma: Well-defined cystic mass, may have internal septations and mural nodularity (malignant feature)
- Serous cystadenoma: Microcystic pattern - Yamada's Gastroenterology, 7th ed.
4. Bowel and Hollow Viscera
Limitations
Intraluminal air causes acoustic artifact, obscuring bowel walls. USG is best for bowel when it is decompressed or fluid-filled. A 6-hour fast is recommended. A curved 2-5 MHz probe surveys broadly; a high-frequency linear probe (7.5-13 MHz) is used for superficial structures. - Yamada's Gastroenterology
Acute Appendicitis
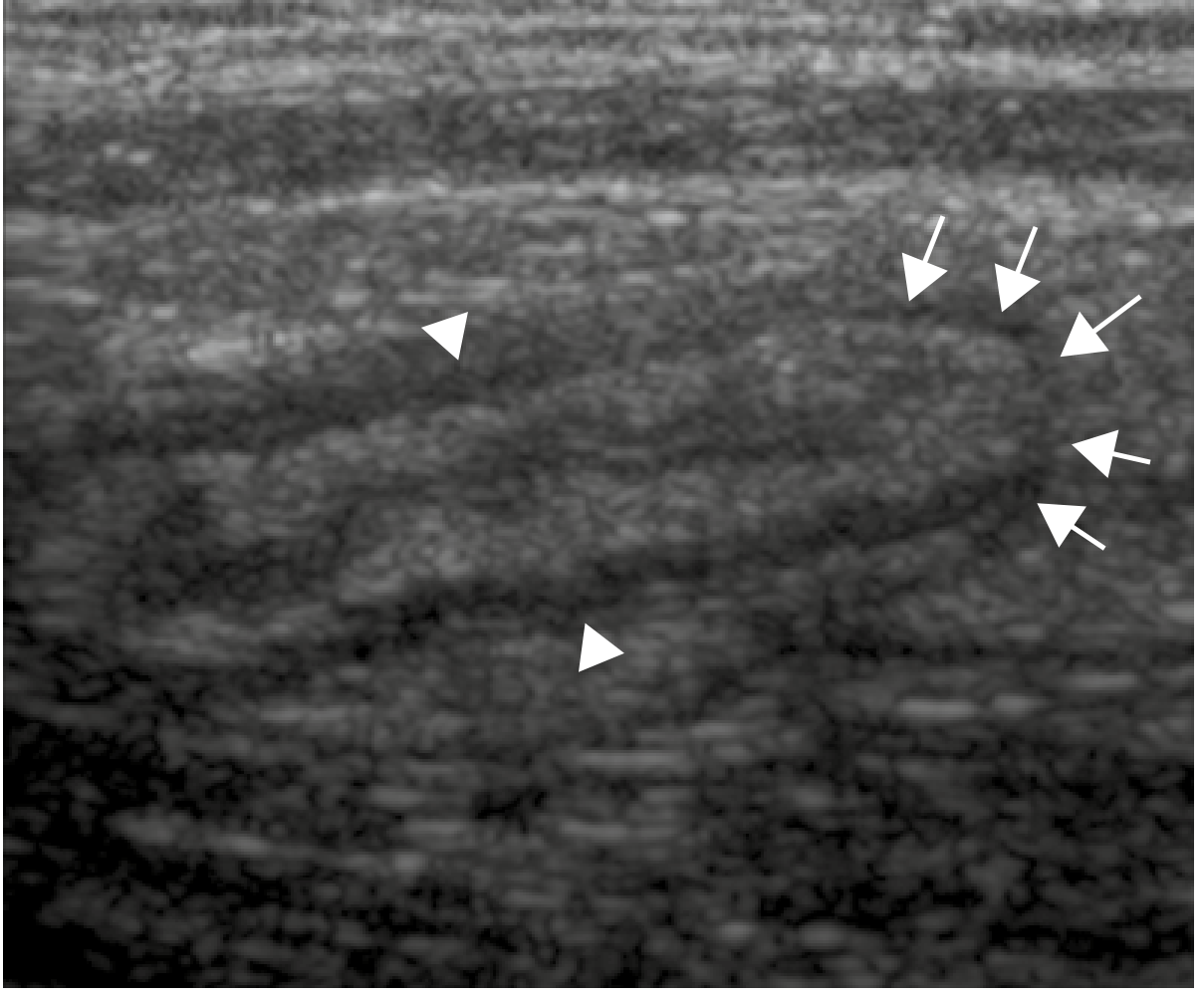
- A normal appendix is very difficult to identify on USG
- An inflamed appendix appears as a dilated (>7 mm), blind-ending, non-compressible tubular structure arising from the cecum
- Target sign on transverse view: hypoechoic center + thickened hyperechoic middle layer + hypoechoic outer layer
- Tenderness on direct probe pressure (sonographic McBurney sign)
- Color Doppler shows hyperemia
- An appendicolith may be seen as an echogenic focus with posterior acoustic shadowing
- Surrounding echogenic inflamed mesenteric fat and pericecal free fluid suggest perforation - Yamada's Gastroenterology, 7th ed.
- High-frequency USG can assess extent and activity of inflammatory bowel disease (IBD) and local rectal tumor staging - Grainger & Allison's Diagnostic Radiology
Intussusception
- On transverse USG view: classic "target sign" or "doughnut sign" - outer hypoechoic ring (edematous outer bowel wall) surrounding echogenic intussuscepted mesentery
- USG is the investigation of choice in pediatric intussusception
Bowel Wall Thickening
Nonspecific but seen in appendicitis, diverticulitis, and infectious or inflammatory enteritis/colitis - Yamada's Gastroenterology
5. Ascites and Intra-abdominal Fluid
USG is extremely sensitive for detecting even small amounts of free fluid (ascites, blood, pus). It characterizes:
- Transudative ascites: simple anechoic fluid
- Exudative/complicated ascites: echogenic debris, septations, loculations
- FAST (Focused Assessment with Sonography in Trauma): rapid bedside detection of hemoperitoneum in trauma
6. Portal Hypertension and Vascular Assessment
Doppler USG is indispensable for:
- Assessing portal vein patency and flow direction (hepatopetal vs. hepatofugal)
- Detecting portal vein thrombosis
- Assessing hepatic artery flow post-transplant
- Identifying varices (dilated collateral vessels)
- Measuring splenic vein and superior mesenteric vein dimensions - Goldman-Cecil Medicine; Maingot's Abdominal Operations
7. Endoscopic Ultrasound (EUS) - Extended Role
When transabdominal USG is limited by bowel gas or depth:
- EUS (ultrasound probe mounted on an endoscope) provides excellent imaging of the gallbladder, biliary tree, common bile duct stones <3 mm, pancreatic lesions, and local staging of GI malignancies
- EUS-guided biopsy of pancreatic masses, lymph nodes, and submucosal lesions
- MR cholangiopancreatography (MRCP) and EUS are superior to transabdominal USG for common bile duct stones - Goldman-Cecil Medicine
Summary: USG Utility by Digestive Organ
| Organ / Disease | USG Role | Sensitivity / Specificity |
|---|---|---|
| Gallstones | First-line, method of choice | >95% / >95% |
| Acute cholecystitis | First-line; sonographic Murphy's sign | 85% / 95% |
| Biliary obstruction | Detects ductal dilation, level of block | Good for dilation; limited for stone |
| Liver - diffuse disease (cirrhosis) | Size, echogenicity, nodularity, ascites | Good |
| Liver - focal lesion | Cyst vs. solid; Doppler vascularity | Good for detection; CT/MRI superior for characterization |
| Acute pancreatitis | Biliary etiology assessment; complication monitoring | Limited (bowel gas); CT preferred for necrosis |
| Chronic pancreatitis | Calcifications, ductal dilation | Good |
| Pancreatic cancer | Hypoechoic mass, vessel invasion | Moderate; EUS superior |
| Acute appendicitis | Dilated non-compressible tubular structure | 80-90% in experienced hands |
| Intussusception | Target/doughnut sign | Excellent in children |
| Ascites | Detection and characterization | Highly sensitive |
| Portal hypertension | Doppler vascular assessment | Good |
| IBD activity | Bowel wall thickening | Adjunct tool |
Sources: Goldman-Cecil Medicine International Edition, p. 1381; Schwartz's Principles of Surgery, 11th ed.; Yamada's Textbook of Gastroenterology, 7th ed.; Grainger & Allison's Diagnostic Radiology; Fischer's Mastery of Surgery, 8th ed.
Describe the Alāmat of Sue Mizãj-e-Meda Hãr
Finding Sources
Searching the Web
Sue Mizaj Meda Har Unani medicine alamat signs symptoms hot temperament stomach
Searching the Web
Sue Mizaj Meda Har alamat Unani tibb hot dyscrasia stomach symptoms classical
Searching the Web
"sue mizaj" meda haar signs "unani" OR "tibb" OR "hikmat" stomach hot temperament dyscrasia
Reading Web Page
http://www.acamjournal.com/open-access/mizaj-theory-of-greko…
Searching the Web
Avicenna Canon medicine stomach hot temperament dyscrasia symptoms Qanoon Meda hararat alamat
Reading Web Page
https://data.nur.nu/Kutub/English/Avicenna_Canon-of-Medicine…
I now have comprehensive material from classical Unani sources (Avicenna's Canon of Medicine, Greco-Arabic medical theory) and modern Unani research papers. Here is the detailed answer:
Alāmat (Signs & Symptoms) of Sue Mizāj-e-Meda Hār
(Hot Dyscrasia / Morbid Hot Temperament of the Stomach)
Background and Conceptual Framework
In Unani (Greco-Arabic/Tibb) medicine, the concept of Mizāj (temperament) is fundamental. Every organ in the body has its own inherent temperament (Mizāj-e-Uzw). The stomach (Meda) possesses a moderately warm and moist natural temperament, which enables it to perform proper digestion (Hadm).
Sue Mizāj (سوء مزاج) literally means "bad/morbid temperament" - i.e., a deviation of an organ's temperament from its normal (Motadil/Motawazin) state. When the stomach's temperament shifts toward excess Harārat (heat), the condition is called:
Sue Mizāj-e-Meda Hār (سوءِ مزاجِ معدہ حار) = Hot Dyscrasia / Morbid Hot Temperament of the Stomach
This is classified as a Sue Mizāj Sāda (simple morbid temperament) when no morbid humor (Khilt) is involved, and as Sue Mizāj Māddī (humoral/compound morbid temperament) when a hot humor - usually Safra (yellow bile/choleric) or Dam (blood/sanguine) - is the underlying cause.
Classification
| Type | Arabic Term | Description |
|---|---|---|
| Simple hot | Sue Mizāj Hār Sāda | Excess heat without humor accumulation |
| Sanguine hot | Sue Mizāj Hār Damī | Excess heat from dominance of Dam (blood) |
| Bilious hot | Sue Mizāj Hār Safrāwī | Excess heat from dominance of Safra (yellow bile) - most common |
Alāmat (Signs and Symptoms)
1. Gastric / Digestive Symptoms
| Symptom | Unani Term | Explanation |
|---|---|---|
| Burning sensation in the stomach | Sozish-e-Meda / Hurqat-e-Meda | The cardinal sign - intense heat felt in the epigastric region |
| Heartburn / acid regurgitation | Huzāz / Tashammus | Hot material rises from stomach toward throat |
| Nausea and vomiting | Ghathayān wa Qay | Stomach rejects food due to excess heat |
| Increased appetite initially | Ziyādat-e-Ishtihā | Heat initially stimulates digestive faculty (Quwwat-e-Hāzima) |
| Weak digestion later | Zoaf-e-Hazm | Prolonged heat eventually exhausts digestive power |
| Epigastric pain / Stomach pain | Dard-e-Meda / Waja-ul-Meda | Burning, sharp, colicky pain - worsens with hot/spicy food |
| Bitter or acrid belching | Quryā Murra | Bilious/bitter eructations from excess safra |
| Early satiety | Imtilā-e-Meda | Stomach cannot hold food properly |
| Flatulence / bloating | Nafakh / Riyah | Disturbed digestion produces gas |
| Excessive thirst | Atash-e-Shadeed | Excess heat burns up moisture - a hallmark of hot Mizāj |
| Diarrhea / loose stools | Ishal | In hot sanguine/bilious types, excess heat loosens bowels |
| Foul-smelling, acrid stools | Classical sign per Avicenna | "Faeces are strong in odour, acrid" in hot temperament |
2. Constitutional / General Signs (from Meda's hot state spreading to the whole body)
| Sign | Unani Term | Details |
|---|---|---|
| Excessive thirst | Atash | Most consistent general sign of heat |
| Insomnia | Bē-Khwābi | Heat agitates and prevents sleep |
| Increased warmth of the body | Hurārat-e-Jism | Radiates from the stomach outward |
| Rapid pulse | Nabz-e-Saree | Heat accelerates pulse - a diagnostic sign per Avicenna |
| Yellowish complexion | Zardi-e-Rang | When safrawi (bilious) humor is involved |
| Redness of face / flushed appearance | Humrat-e-Wajah | In damawi (sanguine) type |
| Dry mouth and lips | Khushki-e-Dahān | Moisture consumed by heat |
| Blackening of skin and hair | Siyāhi-e-Rang | In chronic heat, sawda (black bile) is generated |
| Rapid onset of weakness and weight loss | Zoaf wa Lāghari | Heat disperses body fluids and wastes tissues |
| Headache | Sudā | Heat ascending from stomach to the head |
3. Urinary Signs
| Sign | Details |
|---|---|
| Dark-colored urine | Urine appears deep yellow/orange - sign of excess heat burning body fluids |
| Strong-smelling, acrid urine | Per Avicenna: "urine strong in odour, acrid" in hot temperament |
| Reduced urine output | Heat retains waste in concentrated form |
4. Mental / Psychological Signs
| Sign | Unani Term |
|---|---|
| Irritability and quick temper | Tund-Mizāji - especially in safrawi (choleric) type |
| Restlessness / agitation | Iztirāb |
| Light, disturbed sleep | Neem-Khwābi |
| Quick intelligence but short patience | Characteristic of hot-bilious temperament |
5. Signs on Examination (Dalāil-e-Jismiya)
| Examination Finding | Significance |
|---|---|
| Warm, dry skin on epigastric palpation | External warmth from stomach heat |
| Skin feels hot to touch | Malmas Hār - indicator of underlying hot Mizāj |
| Tongue: dry, red, with yellow coating | Safra dominant in stomach |
| Rapid, strong (full) pulse | Nabz Saree wa Qawi |
| Epigastric tenderness on palpation | Especially in Waram-e-Meda Hār (hot gastritis) |
Important Distinguishing Features by Humoral Type
Sue Mizāj Hār Sāda (Simple Hot - no humor)
- Burning stomach, intense thirst, hot skin
- Improved by cold foods (cucumber, pomegranate juice, curd)
- Treatment: Ilāj bil Zidd (opposite-quality treatment) with cold-natured foods/drugs
Sue Mizāj Hār Damawi (Sanguine)
- Red face, full bounding pulse, epistaxis
- Veins prominent, energetic initially
- Plethoric body build
Sue Mizāj Hār Safrāwī (Bilious - most common hot type)
- Yellow complexion, bitter vomiting (Qay-e-Safrāwī), intense thirst
- Dard-e-Meda (safrawi) - sharp burning stomach pain
- Bitter belching, green/yellow vomit
- Light sleep, irritability, shrewdness
Asbāb (Causes) of Sue Mizāj-e-Meda Hār
According to Unani texts, the common causes include:
- Ingestion of hot-natured foods (spicy, fatty, fried, alcohol, hot water)
- Excess of Safra (yellow bile) production in liver
- Liver disease - close anatomical and functional relationship of liver and stomach
- Emotional heat - excessive anger (Ghazab) generates heat
- Environmental factors - hot dry climate (summer)
- Excessive exercise or physical exertion
- Prolonged hunger - stomach bile increases
Related Disease Conditions (Sue Mizāj Hār as underlying pathology)
When chronic, Sue Mizāj-e-Meda Hār can lead to:
- Waram-e-Meda Hār (hot gastritis / Warm-e-Meda Safrāwī or Damī)
- Qurha-e-Meda (gastric ulcer - from prolonged heat eroding the stomach lining)
- Hurqat-e-Meda (acid-peptic disease / heartburn syndrome)
- Sokhtan-e-Akhlāt (burning of humors → sawda formation)
- Hummā Safrāwī (bilious fever) as secondary complication
Summary in Tabular Form
| Category | Key Alāmat |
|---|---|
| Gastric | Burning in stomach (Hurqat-e-Meda), heartburn, bitter belching, nausea, vomiting, epigastric pain, weak digestion |
| Constitutional | Excessive thirst, insomnia, restlessness, rapid weight loss |
| Skin/Appearance | Warm dry skin, yellowish/flushed face, dark complexion in chronic cases |
| Pulse | Rapid, strong (Nabz Saree wa Qawi) |
| Urine | Dark, concentrated, strong-smelling |
| Bowels | Diarrhea with foul acrid stool (hot type), occasional constipation |
| Psychological | Irritability, short temper, restlessness, light disturbed sleep |
Classical References
- Ibn Sīnā (Avicenna), Al-Qānūn fī al-Tibb (Canon of Medicine), Book 3 - describes diseases of the stomach with classification by temperamental imbalance; hot temperament signs include: rapid pulse, strong-smelling acrid discharges, excessive heat, thirst, and overactivity of functions
- Thābit ibn Qurra (826-901 AD), Al-Zakhīra fil Tibb - described four varieties of gastritis based on humoral imbalance of Meda's Mizāj
- Ibn Hubbal Baghdādī - described Waram-e-Meda pathogenesis through humoral accumulation
The classical Unani principle of treatment is Ilāj bil Zidd (heterotherapy by opposites) - hot dyscrasia is corrected with cold-natured medicines and diet such as pomegranate juice, curd (cow's milk), purslane, barley water, sandalwood preparations, and cold regimenal therapies.
This is a shared conversation. Sign in to Orris to start your own chat.