Heart and great vessels complete notes of anatomy full details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the core content needed for a full set of notes. Let me compile the comprehensive anatomy notes.
Heart and Great Vessels - Complete Anatomy Notes
Sources: Gray's Anatomy for Students, Color Atlas of Human Anatomy Vol. 2 (Internal Organs), Goldman-Cecil Medicine
1. OVERVIEW AND GENERAL FEATURES
The heart is a hollow, muscular pump located in the mediastinum of the thoracic cavity. Its shape resembles a pyramid that has fallen over and rests on one of its sides. The heart has:
- Weight: ~250-350 g in adults
- Size: Roughly the size of the owner's fist
- Location: The middle mediastinum, enclosed within the pericardial sac
2. ORIENTATION, SURFACES, AND BORDERS
Orientation
The heart rests on its diaphragmatic surface, with:
- Apex pointing forward, downward, and to the left (left 5th intercostal space, 8-9 cm from the midsternal line)
- Base directed posteriorly, fixed to the pericardial wall opposite vertebral bodies TV-TVIII (TVI-TIX standing)
Surfaces
| Surface | Composition |
|---|---|
| Anterior (sternocostal) | Mostly right ventricle; right atrium on the right, left ventricle on the left |
| Diaphragmatic (inferior) | Left ventricle (majority) + small portion of right ventricle; separated by posterior interventricular groove |
| Left pulmonary | Left ventricle + portion of left atrium; broad and convex |
| Right pulmonary | Right atrium; broad and convex |
| Base (posterior) | Left atrium (mostly) + small portion of right atrium + proximal great veins (SVC, IVC, pulmonary veins) |
Margins
- Right margin = Right pulmonary surface (right atrium)
- Left margin (obtuse) = Anterior/left pulmonary surfaces; from left auricle to apex; formed by left ventricle
- Inferior margin (acute) = Sharp edge between anterior and diaphragmatic surfaces; mostly right ventricle
- Superior margin = Formed by the right and left atria and auricles
Radiological Borders (PA CXR)
| Border | Structures |
|---|---|
| Right | SVC, right atrium, IVC |
| Left | Arch of aorta (aortic knuckle), pulmonary trunk, left auricle, left ventricle |
| Inferior | Right ventricle + left ventricle at apex |
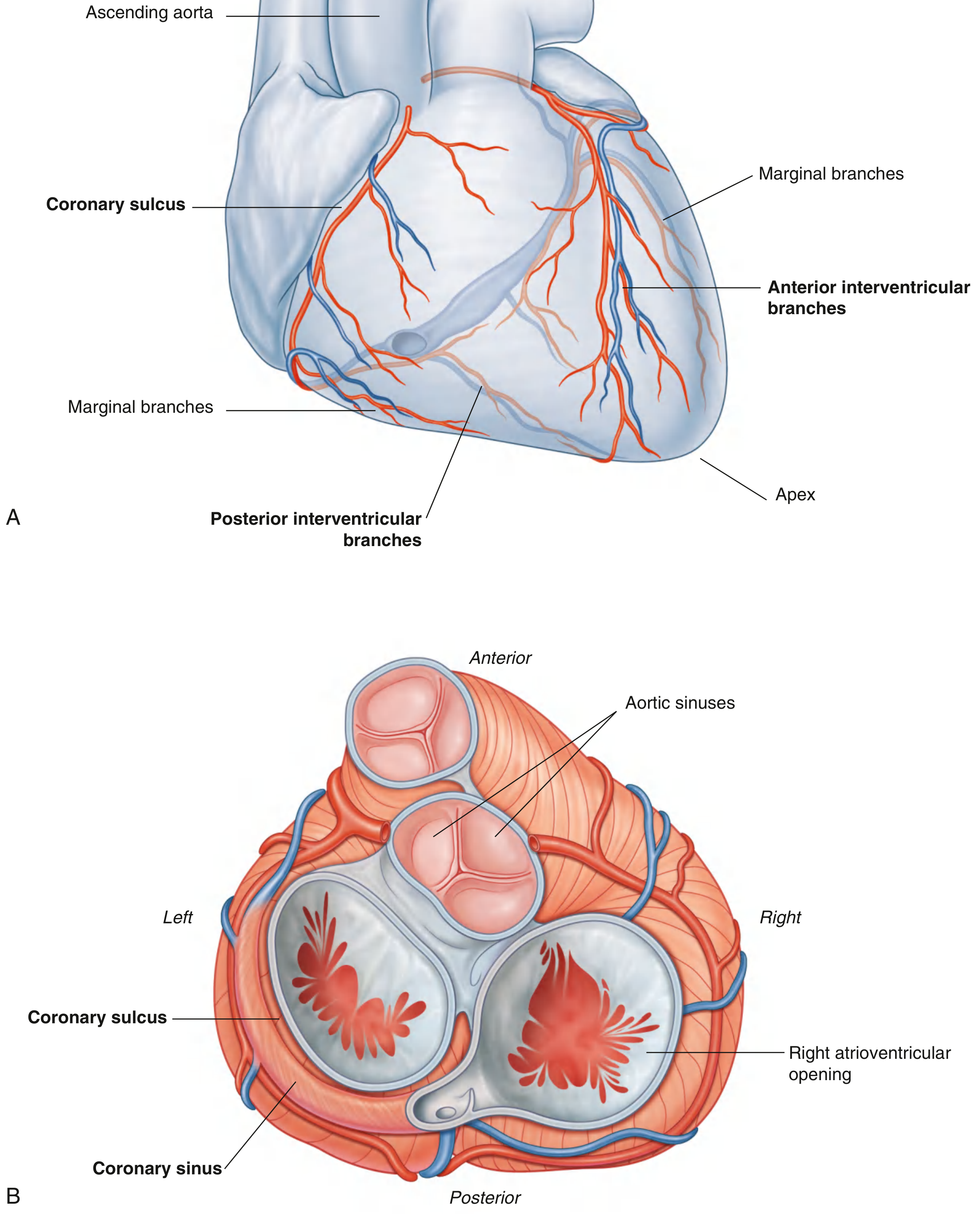
3. EXTERNAL SULCI
Internal partitions produce external grooves (sulci):
- Coronary sulcus (atrioventricular groove): Circles the heart, separates atria from ventricles. Contains: right coronary artery, small cardiac vein, coronary sinus, and circumflex branch of the left coronary artery.
- Anterior interventricular sulcus: Anterior surface; separates the two ventricles. Contains: anterior interventricular artery (LAD) and great cardiac vein.
- Posterior interventricular sulcus: Diaphragmatic surface. Contains: posterior interventricular artery (PDA) and middle cardiac vein.
4. PERICARDIUM
The heart is enclosed in the pericardium, a double-walled sac:
- Fibrous pericardium (outer): Tough, inextensible; attached to the central tendon of the diaphragm below and fusing with the adventitia of the great vessels above
- Serous pericardium (inner): Two layers:
- Parietal layer: Lines the inner surface of fibrous pericardium
- Visceral layer (epicardium): Closely applied to the surface of the heart and great vessels
- Pericardial cavity: Potential space between the two serous layers, containing a thin film of serous fluid for lubrication
Pericardial Sinuses
- Transverse sinus: Lies between the arterial vessels (aorta + pulmonary trunk) anteriorly and the venous vessels (SVC + pulmonary veins) posteriorly
- Oblique sinus: A blind-ending recess behind the left atrium, bounded by the pulmonary veins
5. LAYERS OF THE HEART WALL
| Layer | Description |
|---|---|
| Epicardium | Outer layer; mesothelium + thin connective tissue + subepicardial fat (visceral pericardium) |
| Myocardium | Middle; cardiac muscle; thickest in the left ventricle |
| Endocardium | Inner lining; continuation of the tunica intima of vessels; endothelium + thin connective tissue |
Histology of Cardiac Muscle
- Cells are up to 120 μm long, average diameter 20 μm in adults
- Branched cells connected end-to-end; centrally placed pale nucleus
- Intercalated discs: Transverse cell boundaries; contain desmosomes (mechanical coupling) and gap junctions/nexus (electrical coupling for impulse propagation)
- T-tubules (transverse): Derivatives of the sarcolemma; involved in excitation-contraction coupling
- L-tubules (longitudinal): Formed by the sarcoplasmic/endoplasmic reticulum
- Rich in mitochondria (energy supply) and glycogen
6. CARDIAC SKELETON
A collection of dense fibrous connective tissue forming four fibrous rings in a plane between the atria and ventricles:
- Surrounds all four valve orifices: two atrioventricular (mitral, tricuspid) + two arterial (aortic, pulmonary)
- Functions: Provides attachment for cardiac muscle bundles; electrically insulates atria from ventricles (except the AV bundle); maintains shape of valve orifices
- The only pathway for electrical conduction from atria to ventricles is the AV bundle (Bundle of His) passing through the central fibrous body
7. CHAMBERS OF THE HEART
7.1 Right Atrium
Two functional parts:
Sinus of the venae cavae (posterior, smooth-walled):
- Receives the superior vena cava (SVC) - opens downward and anteriorly, no valve
- Receives the inferior vena cava (IVC) - opening shielded by the valve of the IVC (Eustachian valve), a crescent-shaped fold; in fetal life this was large and directed blood through the foramen ovale
- Foramen ovale (fetal) becomes the oval fossa (fossa ovalis) after birth, bordered by the limbus fossae ovalis
- Receives the coronary sinus (returns deoxygenated blood from the heart wall), guarded by the valve of the coronary sinus (Thebesian valve)
- Smallest cardiac veins (foramina of Thebesius) open directly into the right atrium
True atrium (anterior):
- Interior: pectinate muscles (muscular ridges projecting into the cavity)
- Continuous anteriorly with the right auricle
- Separated from the sinus by the crista terminalis (internal ridge; externally the sulcus terminalis)
Interatrial septum: Contains the fossa ovalis; occasionally a patent foramen ovale (PFO) persists.
7.2 Right Ventricle
Two parts separated by muscular ridges:
- Supraventricular crest (crista supraventricularis)
- Septomarginal trabecula (moderator band)
| Part | Location | Features |
|---|---|---|
| Inflow tract | Posteroinferior | Trabeculae carneae (muscular ridges); chordae tendineae; papillary muscles |
| Outflow tract (conus arteriosus/infundibulum) | Anterosuperior; smooth-walled | Leads to pulmonary trunk |
Key structures:
- Trabeculae carneae: Muscular ridges projecting into the cavity
- Papillary muscles (3): Anterior (largest), posterior, septal - prevent eversion of tricuspid valve cusps during systole
- Chordae tendineae: Tendinous cords connecting papillary muscles to valve cusps
- Septomarginal trabecula (moderator band): Bridges the lower interventricular septum to the base of the anterior papillary muscle; carries the right bundle branch of the AV conduction system
- Myocardial wall thickness: Thin (3-5 mm); produces lower pressure (pulmonary circulation)
7.3 Left Atrium
- Forms most of the base (posterior surface) of the heart
- Four pulmonary veins enter (two on each side) - no valves; the pulmonary vein ostia are smooth-walled (derived from incorporated pulmonary vein)
- Interior: mostly smooth-walled (evolved from absorbed pulmonary veins)
- Left auricle is a small appendage projecting anteriorly - in atrial fibrillation, thrombi commonly form here
- Interatrial septum: The left side shows a slight depression at the fossa ovalis
7.4 Left Ventricle
Thickest-walled chamber (~8-12 mm vs. 3-5 mm of RV) - generates systemic arterial pressure
Two parts:
- Inflow tract: Receives blood from left atrium through mitral valve; contains trabeculae carneae and two large papillary muscles (anterior and posterior), connected to mitral valve cusps by chordae tendineae
- Outflow tract (aortic vestibule): Smooth-walled; leads to ascending aorta through the aortic valve
Interventricular septum: Has a thick muscular part and a thin membranous part superiorly (site of most VSDs).
8. HEART VALVES
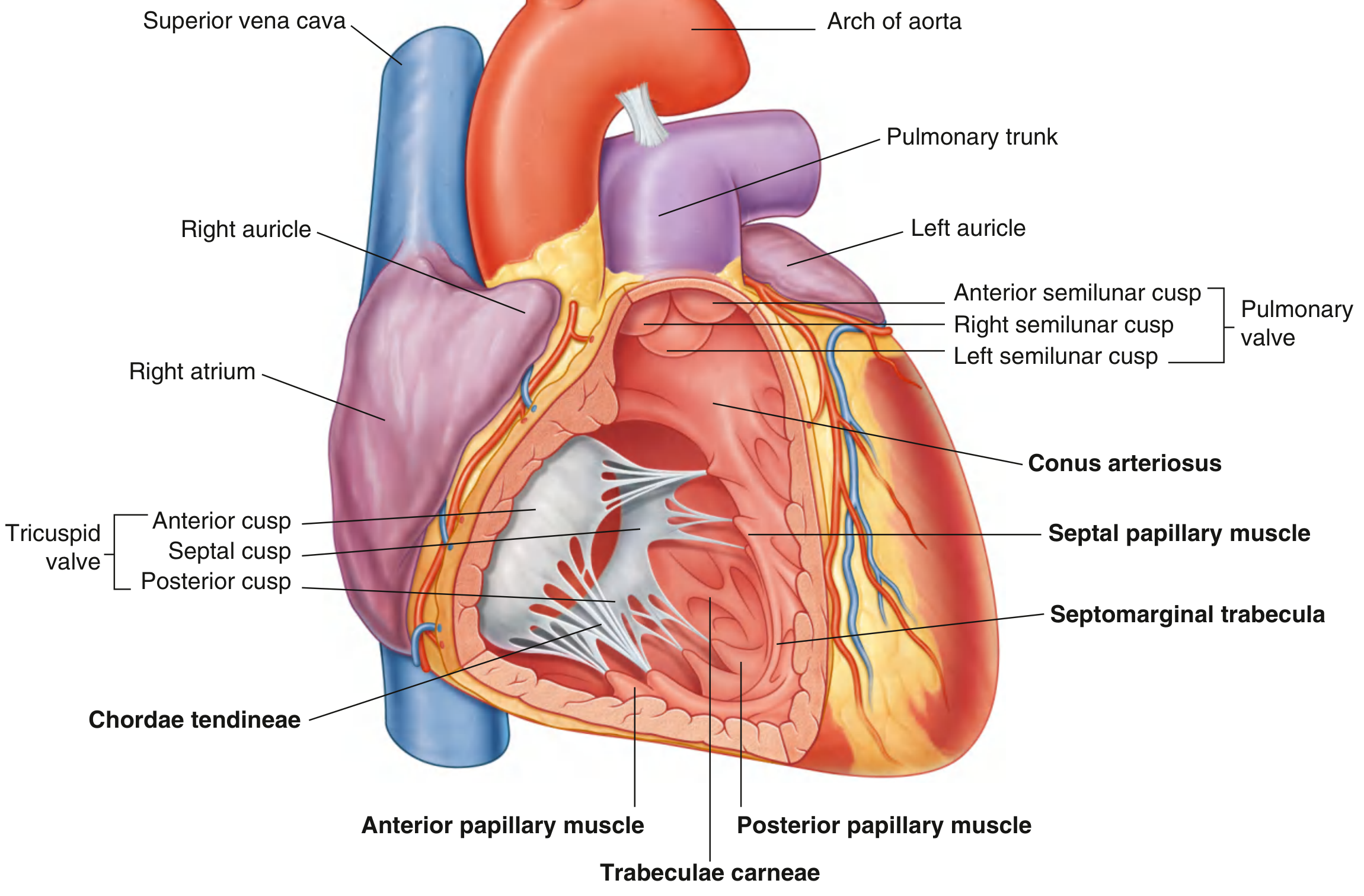
8.1 Tricuspid Valve (Right AV Valve)
- 3 cusps: Anterior, septal, posterior (named by position in RV)
- Bases attached to the right fibrous ring (annulus fibrosus)
- Cusps are continuous at commissures
- Chordae tendineae attach the free margins to 3 papillary muscles
- Prevents reflux into right atrium during ventricular systole
8.2 Pulmonary Valve (Semilunar)
- Located at the apex of the infundibulum (outflow tract of RV)
- 3 semilunar cusps: Left, right, and anterior (named by fetal position before outflow rotation)
- Each cusp has:
- Nodule (thickened middle of free edge)
- Lunula (thin lateral portions)
- Pulmonary sinus (pocket-like dilation in pulmonary trunk wall)
- After ventricular contraction, blood recoil fills sinuses, forcing cusps closed
8.3 Mitral Valve / Bicuspid Valve (Left AV Valve)
- 2 cusps: Anterior (aortic/septal) and posterior (mural)
- Bases attached to the left fibrous ring (annulus fibrosus)
- Connected by chordae tendineae to two papillary muscles (anterior and posterior) in the LV
- Prevents reflux into left atrium during ventricular systole
8.4 Aortic Valve (Semilunar)
- Located at the junction of the aortic vestibule and ascending aorta
- 3 semilunar cusps: Right, left, and posterior (= non-coronary)
- Each forms a pocket-like aortic sinus (sinus of Valsalva):
- Right aortic sinus → gives rise to the right coronary artery
- Left aortic sinus → gives rise to the left coronary artery
- Posterior (non-coronary) sinus → no coronary artery origin
- After ventricular contraction, blood recoil fills the sinuses, closes the valve, and simultaneously forces blood into the coronary arteries
Valve Surface Landmarks (Auscultation Areas)
| Valve | Anatomical location | Auscultation site |
|---|---|---|
| Aortic | Right 2nd intercostal space, parasternal | Right 2nd ICS |
| Pulmonary | Left 2nd intercostal space, parasternal | Left 2nd ICS |
| Tricuspid | Lower left sternal border | Left 4th/5th ICS, parasternal |
| Mitral | Left 5th ICS, midclavicular line | Apex (mitral area) |
9. BLOOD SUPPLY - CORONARY ARTERIES
Coronary arteries arise from the right and left aortic sinuses of the ascending aorta. They lie in the subepicardial fat within the coronary and interventricular sulci. Functionally, they are end arteries (small anastomoses are insufficient to develop adequate collateral circulation acutely).
9.1 Right Coronary Artery (RCA)
- Arises from the right aortic sinus
- Travels in the coronary sulcus (right atrioventricular groove)
- Branches:
- SA nodal artery (in ~60% of people from RCA; 40% from LCx)
- Right marginal artery (acute marginal)
- Posterior interventricular artery (PDA) - in right dominant circulation (~70% of people); runs in the posterior interventricular sulcus to supply the posterior 1/3 of interventricular septum
- AV nodal artery (usually from RCA in right-dominant hearts)
- Supply (right-dominant): Right atrium, SA node (mostly), AV node, right ventricle (most), posterior portion of LV, posterior 1/3 of interventricular septum
9.2 Left Coronary Artery (LCA)
- Short trunk (~1-2 cm = left main stem) arising from left aortic sinus
- Passes between the pulmonary trunk and left auricle before bifurcating
A. Left Anterior Descending (LAD) / Anterior Interventricular Artery
- Travels in the anterior interventricular sulcus toward the apex
- Clinical name: LAD
- Branches: Diagonal branches, septal perforating arteries
- Supply: Anterior 2/3 of interventricular septum, anterior wall of LV, anterior wall of RV, apex
B. Left Circumflex (LCx) / Circumflex Artery
- Runs posteriorly in the left coronary sulcus (left atrioventricular groove)
- Branches: Obtuse marginal arteries
- Supply: Left atrium, lateral and posterior wall of LV
Coronary Dominance
| Dominance | Definition | Incidence |
|---|---|---|
| Right dominant | PDA from RCA | ~70% |
| Left dominant | PDA from enlarged LCx | ~10% |
| Co-dominant (balanced) | Both RCA and LCx contribute | ~20% |
Coronary Veins
| Vein | Course | Empties into |
|---|---|---|
| Great cardiac vein | Anterior interventricular sulcus → left coronary sulcus | Coronary sinus |
| Middle cardiac vein | Posterior interventricular sulcus | Coronary sinus |
| Small cardiac vein | Right side of coronary sulcus | Coronary sinus |
| Coronary sinus | Posterior coronary sulcus | Right atrium (between IVC and TV) |
| Anterior cardiac veins | Anterior RV wall | Directly into right atrium |
| Smallest cardiac veins (Thebesian) | Heart wall | Directly into cardiac chambers |
10. CONDUCTING SYSTEM OF THE HEART
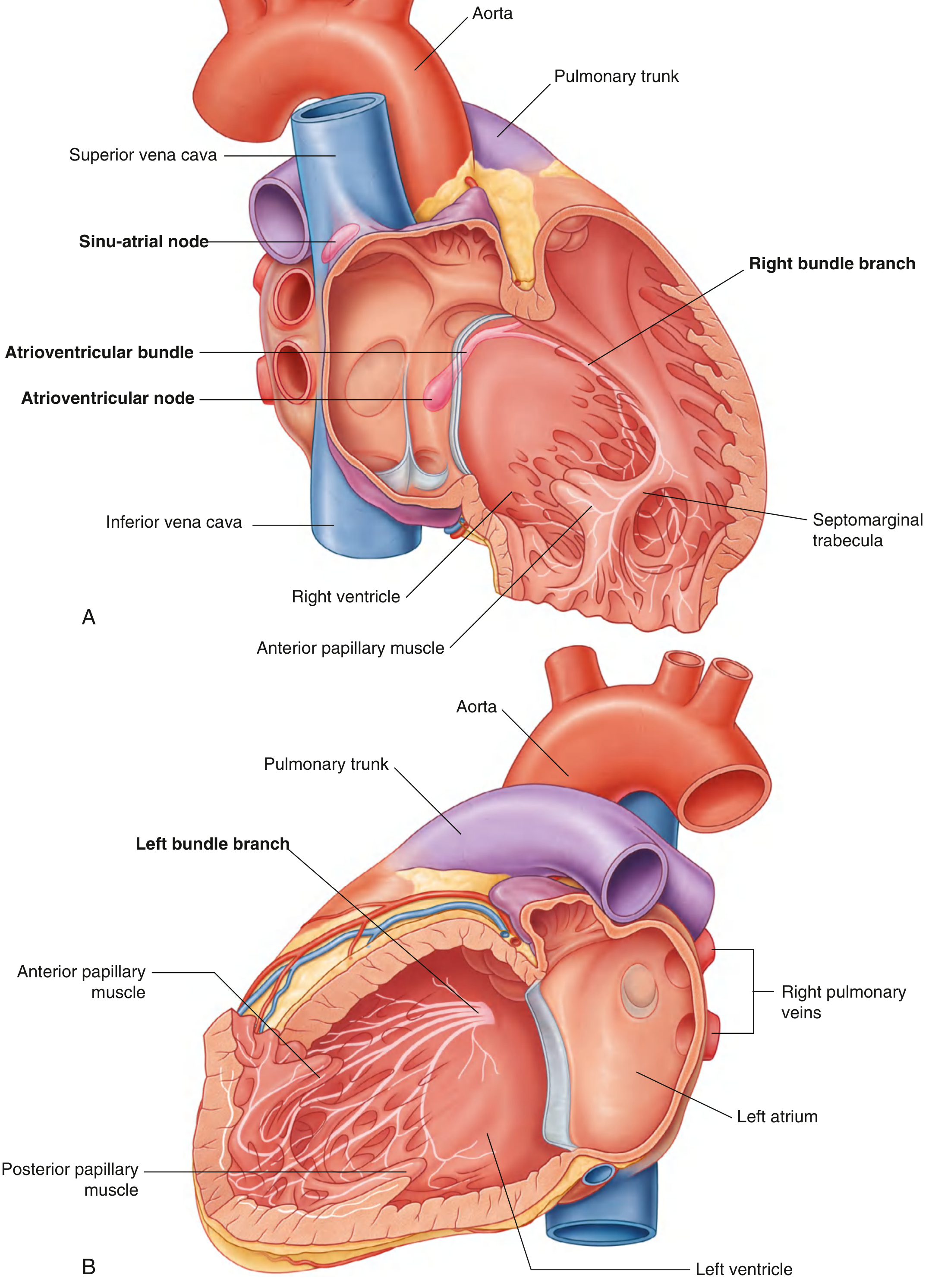
Specialized cardiac muscle cells that generate and conduct rhythmic electrical impulses, differing histologically and functionally from the working myocardium.
Components
| Structure | Location | Function |
|---|---|---|
| SA Node (Keith-Flack node) | Beneath epicardium at the junction of SVC and right atrium (near sulcus terminalis) | Primary pacemaker; generates ~60-100 impulses/min |
| Internodal pathways | Atrial myocardium | Conduct impulse from SA → AV node |
| AV Node (Aschoff-Tawara node) | Floor of right atrium near the opening of the coronary sinus; at apex of Koch's triangle | Delays impulse (~0.12 sec); allows atrial contraction to complete before ventricular contraction; backup pacemaker (~40-60/min) |
| Bundle of His (AV bundle) | Runs along the lower border of the membranous interventricular septum | Only electrical pathway between atria and ventricles (through the cardiac skeleton) |
| Right bundle branch | Descends on right side of interventricular septum → enters septomarginal trabecula → to anterior papillary muscle | Conducts to right ventricle |
| Left bundle branch | Passes to left side of muscular IVS → descends to apex | Conducts to left ventricle (divides into anterior and posterior fascicles) |
| Subendocardial plexus (Purkinje fibers) | Spread throughout ventricular walls (subendocardial) | Rapidly distributes impulse to ventricular myocardium including papillary muscles |
Koch's triangle (boundaries): Tendon of Todaro posteriorly, septal leaflet of tricuspid valve anteriorly, coronary sinus ostium inferiorly - the AV node lies at the apex.
11. INNERVATION OF THE HEART
The heart receives autonomic innervation via the cardiac plexus:
Cardiac Plexus
| Part | Location |
|---|---|
| Superficial | Inferior to the aortic arch, between it and the pulmonary trunk |
| Deep | Between the aortic arch and the tracheal bifurcation |
Sympathetic Supply
- Origin: T1-T5 lateral horn (sympathetic chain ganglia - cervical and upper thoracic)
- Nerves: Cardiac accelerator nerves from the superior, middle, and inferior cervical sympathetic ganglia + thoracic cardiac branches
- Effects: Increased heart rate (chronotropy), increased force of contraction (inotropy), coronary vasodilation, increased conduction velocity
Parasympathetic Supply
- Origin: Dorsal motor nucleus of the vagus nerve (CN X)
- Nerves: Superior and inferior cervical cardiac branches of the vagus nerve
- Effects: Decreased heart rate, decreased AV conduction (primarily acts on SA and AV nodes), coronary vasoconstriction (minor effect)
Afferent (Pain) Fibers
- Travel with sympathetic fibers → enter the spinal cord at T1-T5
- Referred pain of cardiac ischemia: Left chest, left arm (ulnar aspect), left jaw, epigastrium - due to convergence of afferent fibers from these dermatomes at T1-T5
12. GREAT VESSELS
12.1 Aorta
Four parts:
A. Ascending Aorta
- Rises from the aortic valve (at the level of sternal angle/T4)
- Length: ~5 cm
- Gives off the right and left coronary arteries (only branches of ascending aorta)
- Enclosed within the pericardial sac
B. Arch of the Aorta
- Begins after the pericardium; curves superiorly, posteriorly, and to the left over the left main bronchus
- Ends at the level of the sternal angle (T4)
- Branches from right to left:
- Brachiocephalic trunk (innominate artery) - divides into right common carotid + right subclavian
- Left common carotid artery
- Left subclavian artery
- Related to: ligamentum arteriosum (remnant of ductus arteriosus, connecting it to the pulmonary trunk), recurrent laryngeal nerves, cardiac plexus, trachea
Aortic isthmus: The slight constriction just distal to the origin of the left subclavian and proximal to the ductus arteriosus/ligamentum; site of coarctation of the aorta.
C. Descending Thoracic Aorta
- From T4 to T12 (aortic hiatus of the diaphragm)
- Branches: Posterior intercostal arteries (3rd-11th), subcostal arteries, bronchial arteries, esophageal arteries, superior phrenic arteries
D. Abdominal Aorta
- From aortic hiatus (T12) to bifurcation at L4 into right and left common iliac arteries
12.2 Pulmonary Trunk
- Arises from the right ventricle (infundibulum) at the pulmonary valve
- Approximately 5 cm long; passes posterosuperiorly within the pericardium
- Divides at the concavity of the aortic arch (below the carina, at T5) into:
- Right pulmonary artery - longer; passes to the right lung behind the ascending aorta and SVC
- Left pulmonary artery - shorter; connected to the aortic arch by the ligamentum arteriosum (obliterated ductus arteriosus)
- Carries deoxygenated blood from the right ventricle to the lungs
12.3 Superior Vena Cava (SVC)
- Formed by the union of the right and left brachiocephalic veins at the level of the right 1st costal cartilage
- Length: ~7 cm; no valves
- Descends on the right side, entering the right atrium at the level of the right 3rd costal cartilage
- The lower half is within the pericardium
- Drains venous blood from: head, neck, upper limbs, and thoracic wall (above the diaphragm)
- The azygos vein drains into the SVC posteriorly at the level of the right hilum
12.4 Inferior Vena Cava (IVC)
- Formed by the union of the two common iliac veins at the level of L5
- Passes through the caval opening in the diaphragm at T8
- Enters the right atrium from below
- Guarded by the valve of the IVC (Eustachian valve) within the right atrium
- Drains venous blood from: lower limbs, abdominopelvic organs, kidneys, gonads, liver (via hepatic veins)
12.5 Pulmonary Veins
- Four pulmonary veins (right superior, right inferior, left superior, left inferior)
- Drain oxygenated blood from the lungs into the left atrium
- Enter the left atrium at its four corners (forming the base of the heart)
- No valves at the pulmonary vein-atrial junction
- The smooth posterior wall of the left atrium is derived from the incorporated proximal pulmonary veins
12.6 Brachiocephalic Veins
- Right brachiocephalic vein: Short (~2.5 cm); formed behind the right sternoclavicular joint
- Left brachiocephalic vein: Long (~6 cm); crosses the midline horizontally behind the manubrium
- Both drain: internal jugular vein + subclavian vein
- They join to form the SVC at the right 1st costal cartilage level
13. FETAL CIRCULATION AND POSTNATAL CHANGES
| Fetal Structure | Function | Postnatal Remnant |
|---|---|---|
| Foramen ovale | Right-to-left shunt at atrial level (IVC blood bypasses lungs) | Fossa ovalis (closed in most) |
| Ductus arteriosus | Shunt between pulmonary trunk and aortic arch (bypasses lungs) | Ligamentum arteriosum |
| Ductus venosus | Shunt bypassing hepatic circulation in umbilical vein | Ligamentum venosum |
| Umbilical arteries | Carry deoxygenated blood from fetus to placenta | Medial umbilical ligaments |
| Umbilical vein | Carries oxygenated blood from placenta to fetus | Ligamentum teres hepatis |
At birth, with the first breath:
- Pulmonary vascular resistance falls
- Left atrial pressure rises, closing the foramen ovale
- Increased oxygen tension causes contraction of the ductus arteriosus (closes within hours; anatomically within weeks)
14. LYMPHATICS OF THE HEART
- Dense lymphatic network divided into: deep endocardial, middle myocardial, and superficial epicardial networks
- Larger collecting vessels travel in the epicardium accompanying the aorta and pulmonary trunk
- Drain to tracheobronchial lymph nodes and anterior mediastinal lymph nodes
15. PERICARDIAL RELATIONS AND IMPORTANT ANATOMICAL POINTS
- Posterior relations of the heart: Esophagus (immediately behind the left atrium - basis for transesophageal echocardiography), descending aorta, azygos vein
- Anterior relations: Sternum and costal cartilages (2nd-6th), thymus remnant
- Inferior relations: Diaphragm (central tendon)
- Superiorly: Great vessels (aorta, pulmonary trunk, SVC)
Key Clinical-Anatomical Points
| Point | Significance |
|---|---|
| Apex beat (cardiac impulse) | Left 5th ICS, midclavicular line - formed by left ventricle |
| Cardiac tamponade | Blood in pericardial cavity compresses the heart; rigid fibrous pericardium prevents expansion |
| Sternal angle (angle of Louis) | Level T4/T5 - marks bifurcation of trachea, arch of aorta, SVC entering pericardium |
| Moderator band (septomarginal trabecula) | Carries right bundle branch; clinically important landmark in RV |
| Coarctation of aorta | Narrowing at aortic isthmus (just distal to left subclavian artery origin) |
| PFO | Patent foramen ovale - present in ~25% of adults; potential paradoxical embolism pathway |
Summary Table: Four Chambers at a Glance
| Feature | Right Atrium | Right Ventricle | Left Atrium | Left Ventricle |
|---|---|---|---|---|
| Inflow | SVC, IVC, coronary sinus | Tricuspid valve | 4 pulmonary veins | Mitral valve |
| Outflow | Tricuspid valve | Pulmonary valve (infundibulum) | Mitral valve | Aortic valve (vestibule) |
| Wall texture | Pectinate muscles (anterior); smooth (posterior) | Trabeculae carneae (inflow), smooth (outflow) | Mostly smooth | Thick trabeculae carneae |
| Wall thickness | Thin | 3-5 mm | Thin | 8-12 mm |
| Septal feature | Fossa ovalis | Membranous + muscular IVS | Fossa ovalis (left side) | Membranous + muscular IVS |
| Papillary muscles | 3 (ant., post., septal) | 3 | None (AV valve has subvalvular apparatus) | 2 (ant., post.) |
Sources:
- Gray's Anatomy for Students (9780323934237), pp. 226-252
- Color Atlas of Human Anatomy Vol. 2, Internal Organs (9783132424487), pp. 40-65
- Goldman-Cecil Medicine International Edition (9780323930345)
This is a shared conversation. Sign in to Orris to start your own chat.