Classification and imaging of Müllerian duct anomalies
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Mullerian duct anomalies" AND classification
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks plus all the key images. Let me compile the full answer.
Müllerian Duct Anomalies: Classification and Imaging
Müllerian duct anomalies (MDAs) arise from defects in the normal development, fusion, or resorption of the paired paramesonephric (Müllerian) ducts. They are associated with infertility, recurrent pregnancy loss, obstetric complications, and renal anomalies. The ovaries are unaffected in most cases (they derive from the genital ridge, not the Müllerian ducts).
Classification Systems
AFS/Buttram & Gibbons Classification (Most Widely Used)
The American Fertility Society (AFS) classification, adapted from Buttram and Gibbons (1979), divides MDAs into seven classes:
| Class | Anomaly | Embryological Mechanism |
|---|---|---|
| I | Segmental agenesis/hypoplasia | Failure of Müllerian duct development |
| II | Unicornuate uterus | Failure of one Müllerian duct to develop |
| III | Uterus didelphys | Complete non-fusion of both Müllerian ducts |
| IV | Bicornuate uterus | Incomplete fusion at cephalad extent |
| V | Septate uterus | Failure of resorption of the median septum |
| VI | Arcuate uterus | Near-complete resorption (normal variant) |
| VII | DES-related | In utero diethylstilbestrol exposure |
(Berek & Novak's Gynecology, Table 8-2; Grainger & Allison's Diagnostic Radiology, p. 888)
Note on newer systems: ESHRE/ESGE (2013) and the VCUAM system offer more detailed sub-classifications but the AFS system remains the dominant clinical framework.
Imaging Modalities
MRI is the gold standard for characterising MDAs - it provides exquisite anatomical detail, distinguishes myometrium from fibrous tissue on T2-weighted sequences, and is critical for surgical planning. Key protocol points:
- T2-weighted coronal oblique images (along the long axis of the uterus) are the primary acquisition plane
- T2-weighted axial oblique images best demonstrate fundal contour
- 3D ultrasound (including sonohysterography) is an excellent non-invasive first-line tool with high concordance with MRI findings
- MRI should be reserved for cases where 3D US is unavailable or inconclusive
- Hysterosalpingography (HSG) can suggest the diagnosis but cannot reliably distinguish subtypes
(Creasy & Resnik's Maternal-Fetal Medicine, p. 981; Grainger & Allison, p. 889)
Class I: Uterine Agenesis/Hypoplasia
Mechanism: Failure of normal development of both Müllerian ducts. Ovaries are intact and normal.
Subtypes: Vaginal, cervical, fundal, tubal, or combined agenesis/hypoplasia.
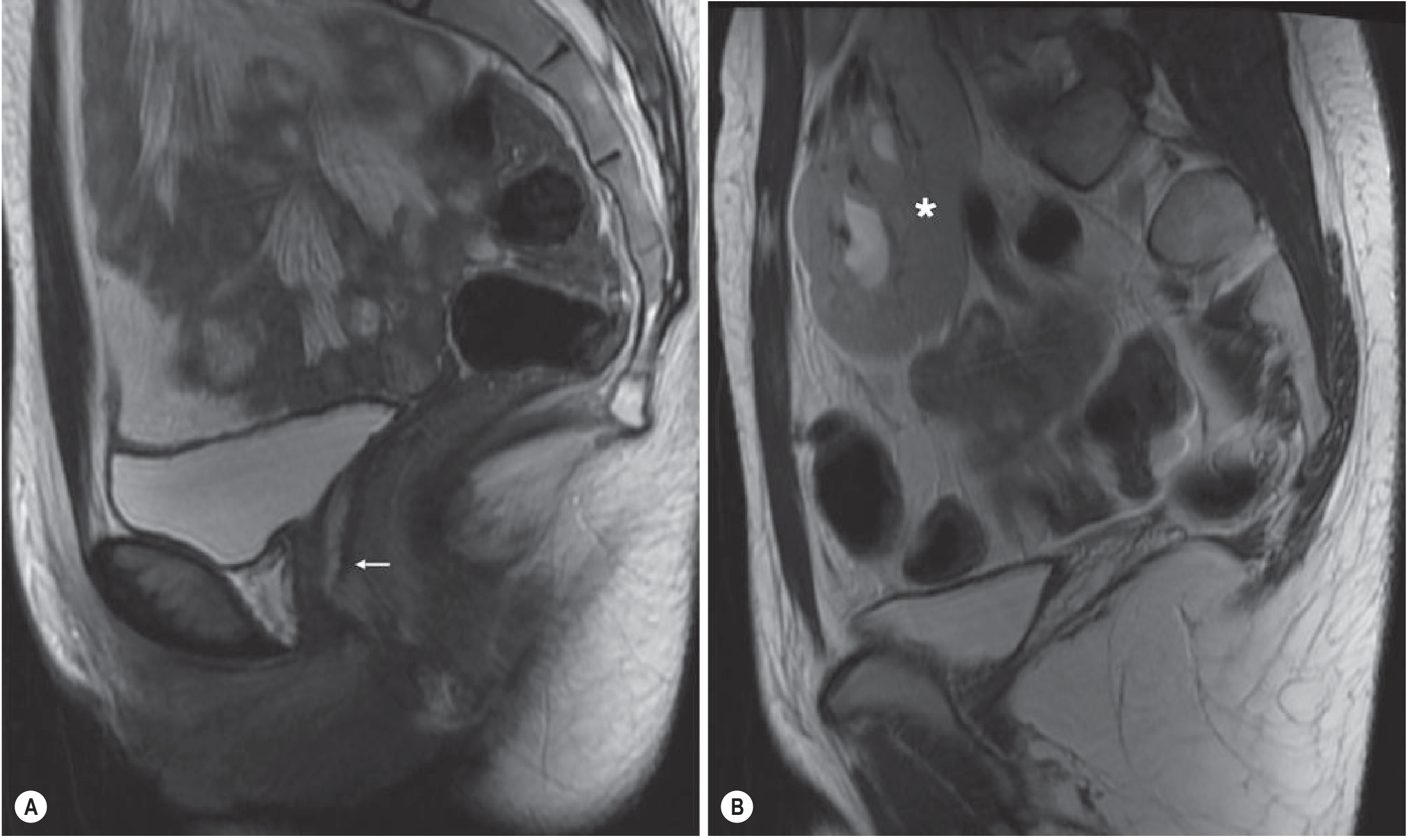
Mayer-Rokitansky-Küster-Hauser (MRKH) Syndrome: The commonest subtype. Uterine and vaginal agenesis/hypoplasia with normal ovaries and fallopian tubes. Associated with pelvic kidney in a significant proportion.
Imaging:
- US: Detection of uterine remnants is difficult
- MRI (sagittal + axial T2WI): Most reliable - shows absent uterus and upper vagina; pelvic kidney may be identified
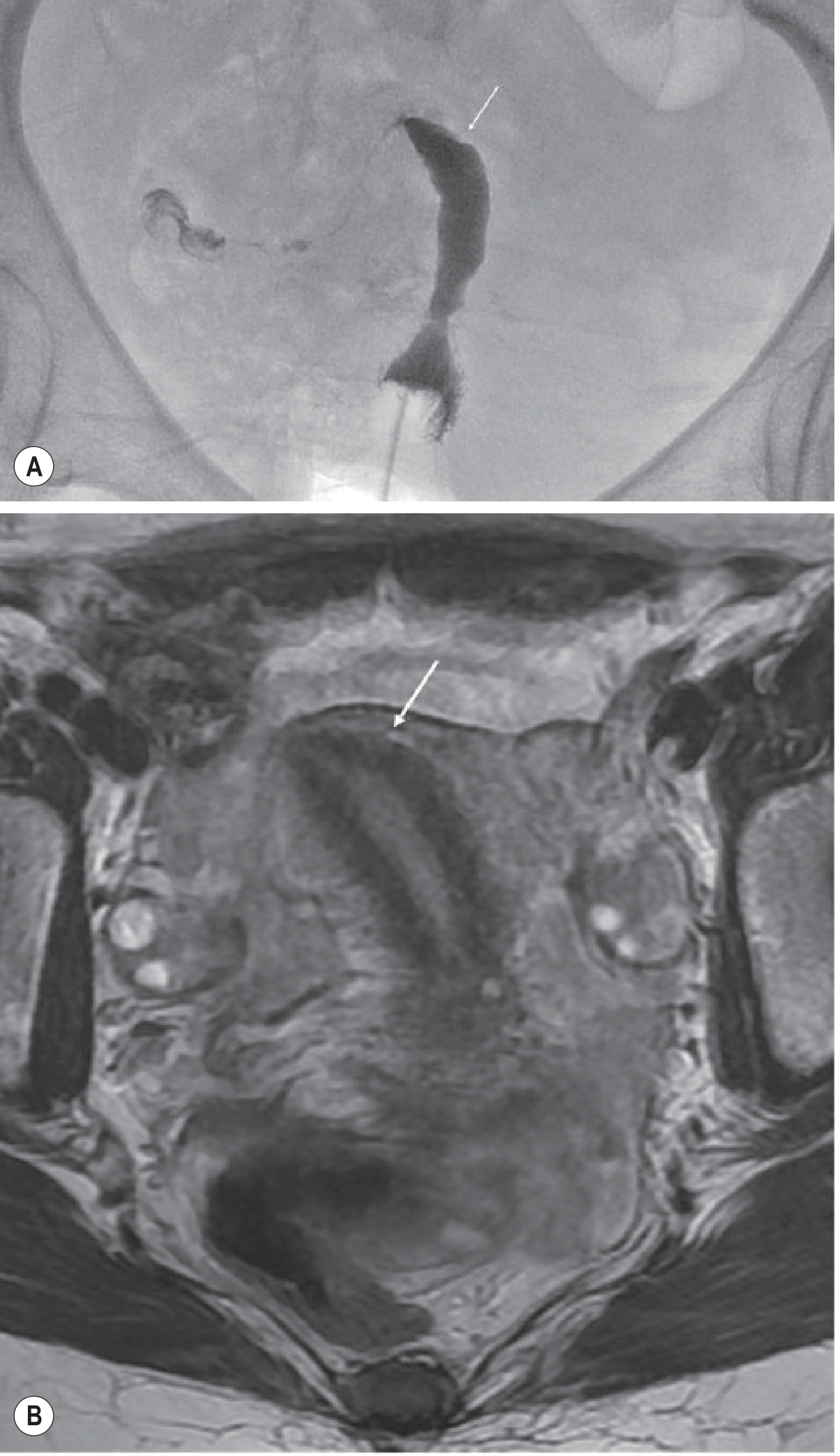
Class II: Unicornuate Uterus
Mechanism: Failure of normal development of one Müllerian duct. Associated with increased spontaneous abortion and obstetric complications.
Subtypes:
- IIa - With rudimentary horn (communicating cavity)
- IIb - With rudimentary horn (non-communicating cavity)
- IIc - With rudimentary horn (no cavity)
- IId - No rudimentary horn
Imaging:
- HSG / US: May raise suspicion
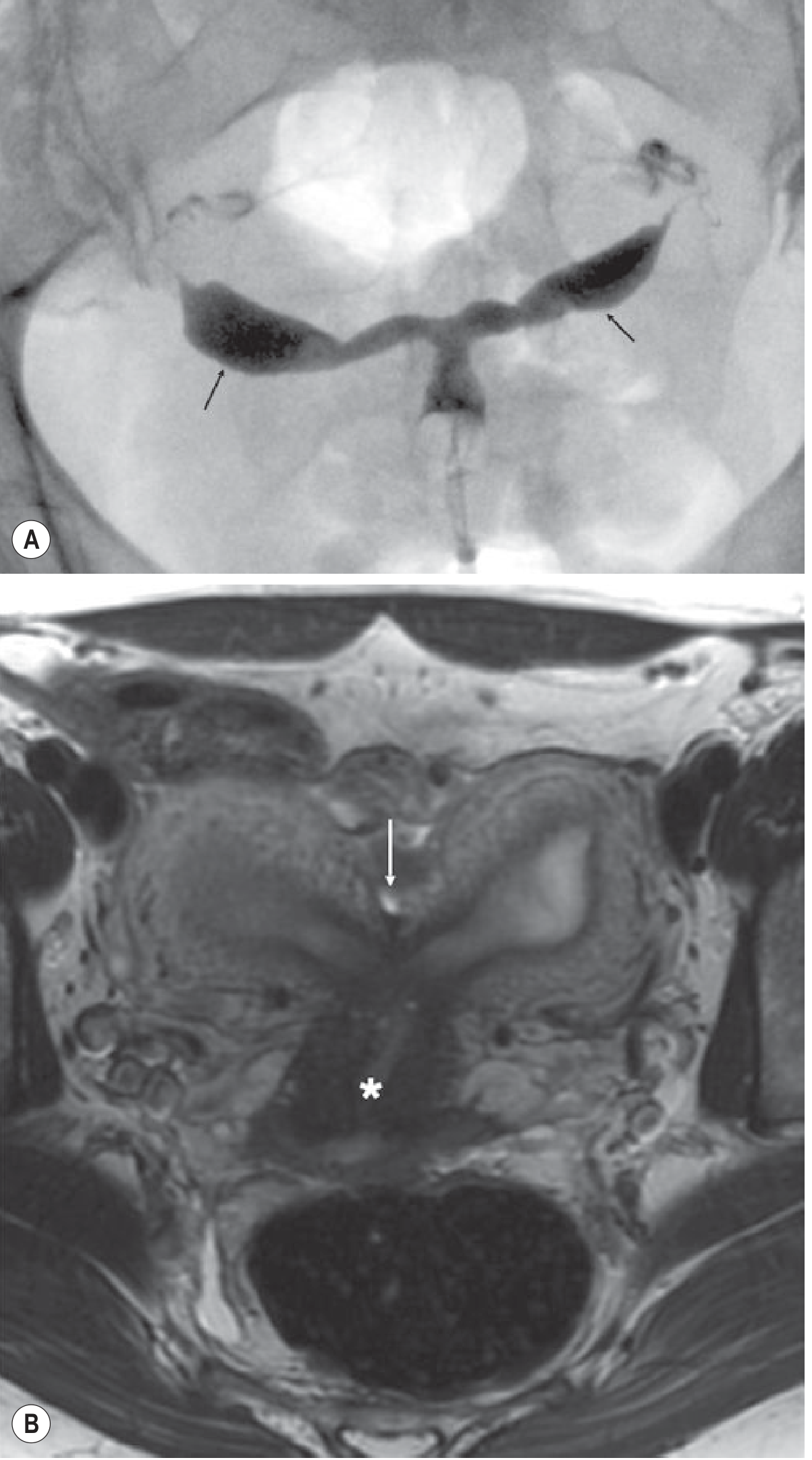
- MRI (axial oblique T2WI): Curved, elongated uterus with tapering of the fundal segment off midline - the classic "banana-like" configuration. Normal zonal anatomy is maintained.
- Functional non-communicating rudimentary horns accumulate blood → haematometra, with increased risk of endometriosis
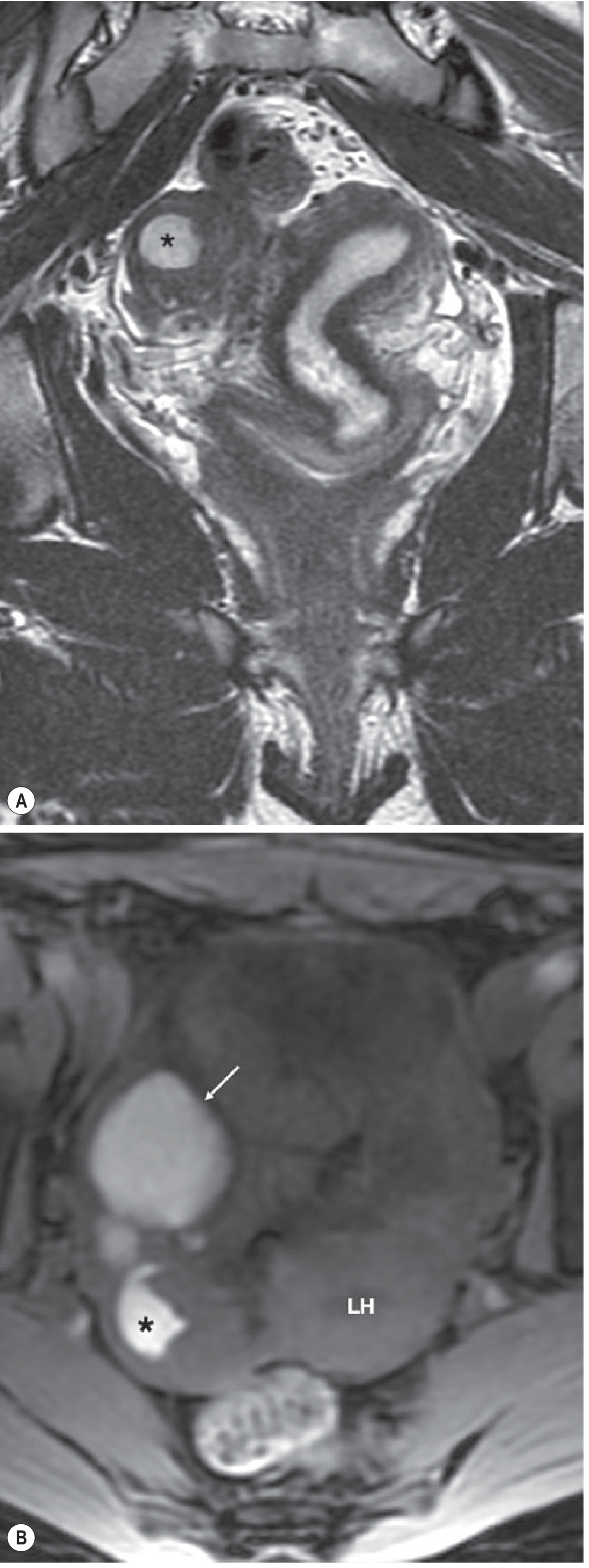
Class III: Uterus Didelphys
Mechanism: Complete non-fusion of both Müllerian ducts → two separate, normal-sized uterine horns and cervices. Longitudinal vaginal septum is present in 75% of cases.
Imaging:
- US: Demonstrates two uterine cavities
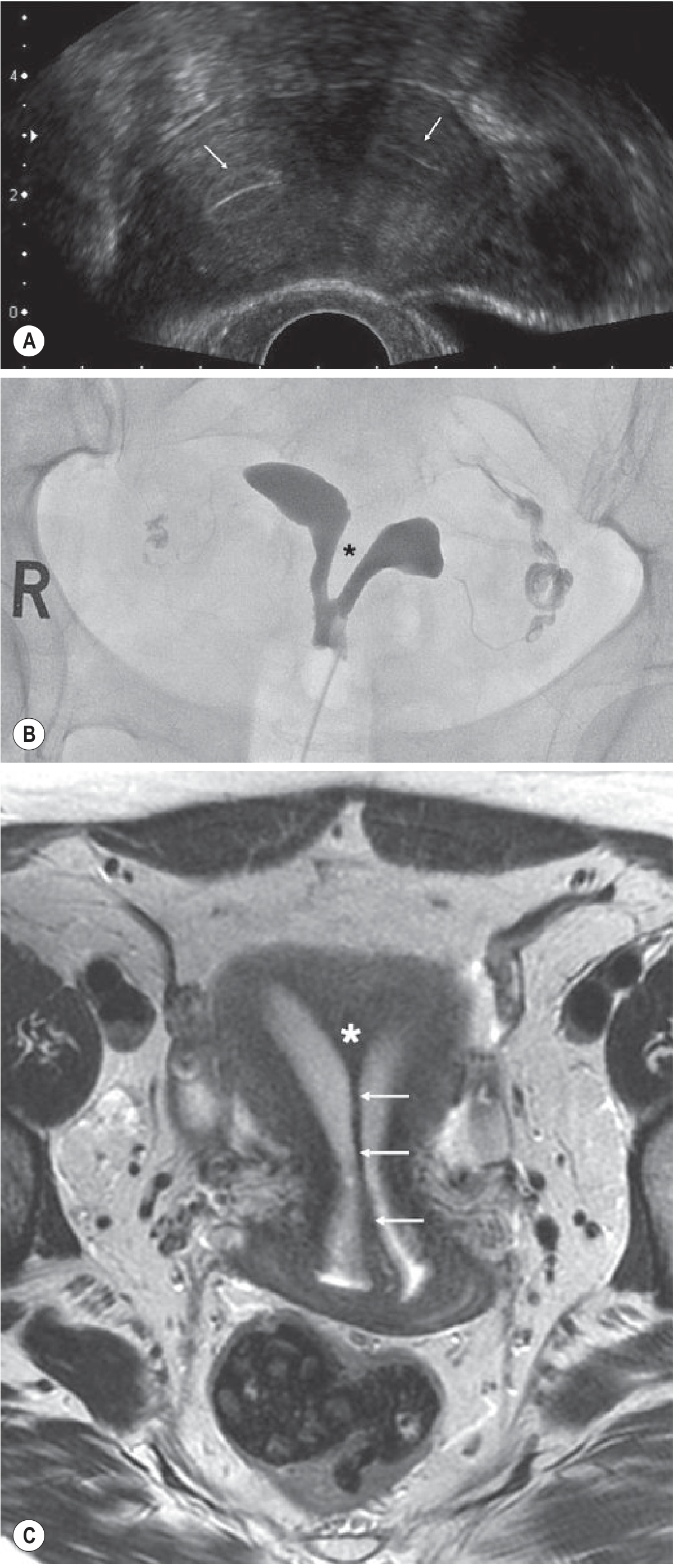
- MRI (coronal oblique T2WI): Two widely separated uterine horns with preserved endometrial and myometrial widths; two cervices and sometimes two vaginas clearly shown
(Grainger & Allison, p. 890)
Class IV: Bicornuate Uterus
Mechanism: Incomplete fusion of the cephalad extent of the uterovaginal horns with resorption of the uterovaginal septum. Obstetric complications relate to the degree of non-fusion.
Imaging:
- HSG: Widely divergent uterine horns (but cannot differentiate from septate uterus)
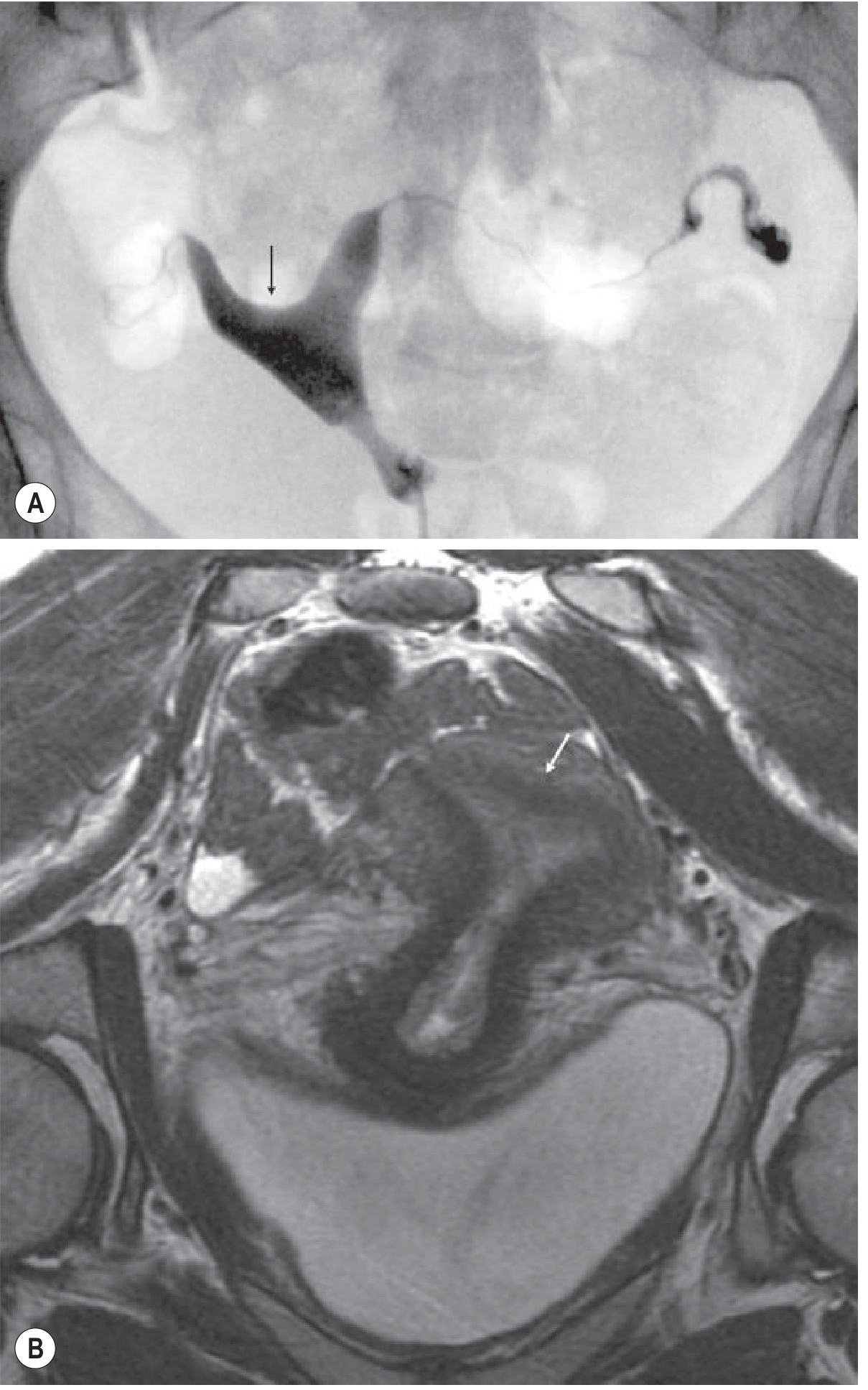
- MRI (coronal oblique T2WI): Two communicating uterine horns with a concave fundal contour; intercornual cleft ≥1 cm in the external fundal myometrium (myometrium is of normal signal on all sequences). Single cervical canal in most cases.
Key differentiator from septate uterus: The external fundal contour is concave/deeply indented (≥1 cm cleft), versus a convex or flat contour in septate uterus.
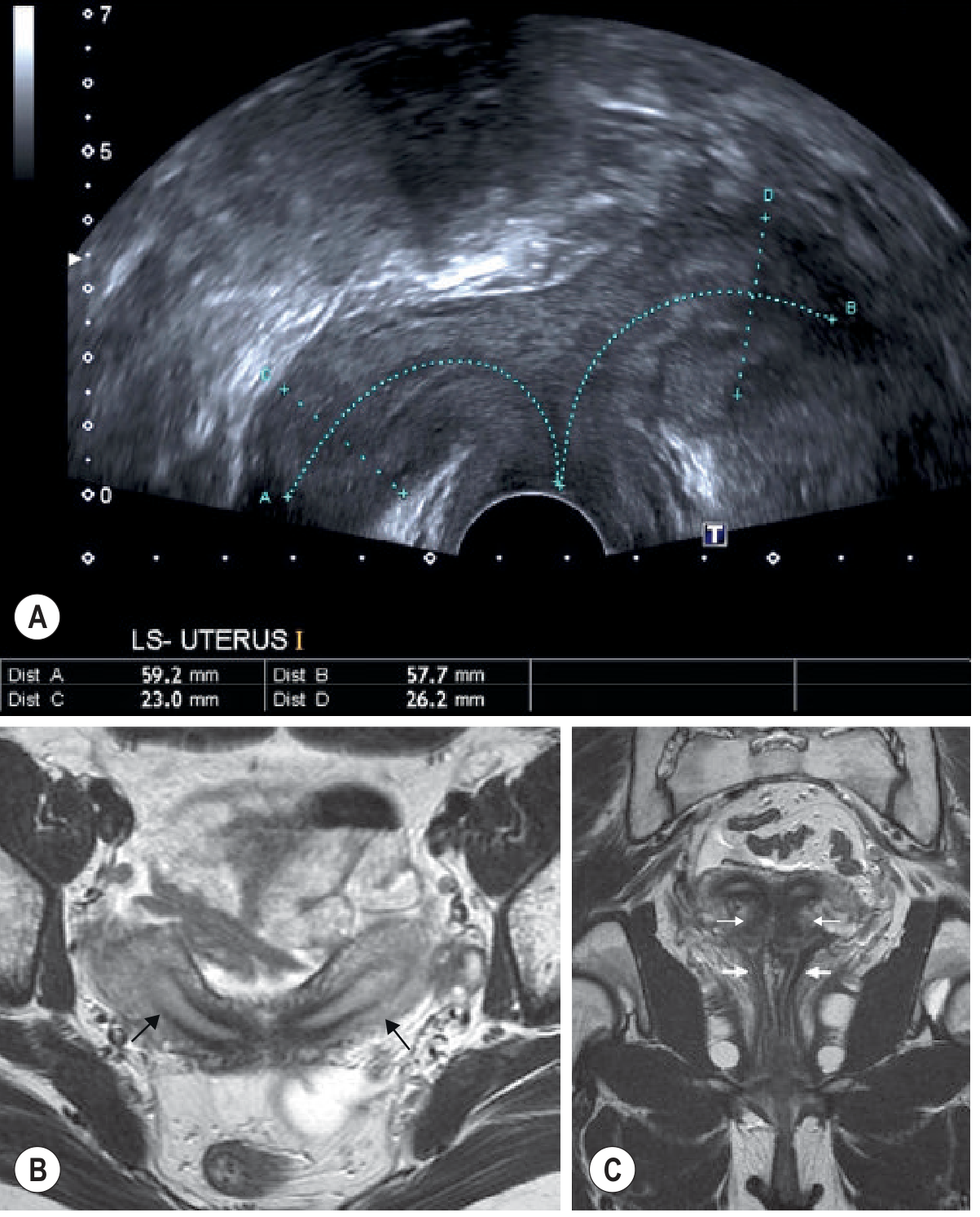
Class V: Septate Uterus
Mechanism: Incomplete resorption of the fibrous septum between two uterine horns following fusion. The septum may be partial or complete (extending to the external cervical os).
Clinical significance: The most common MDA and the one with the worst obstetric outcome of all types (highest rate of miscarriage, fetal malpresentation). Importantly it is also the most surgically correctable via hysteroscopic metroplasty.
Imaging (MRI - coronal oblique T2WI):
- External uterine contour is convex, flat, or concave ≤1 cm (distinguishing from bicornuate)
- The fibrous septum shows low T2 signal (fibrous tissue); a muscular septum shows intermediate T2 signal
- Measurement of septum dimensions guides surgical candidacy
Class VI: Arcuate Uterus
Mechanism: Near-complete resorption of the median septum with a residual smooth, broad fundal indentation. Considered a normal variant with no significant effect on fertility or pregnancy outcome.
Imaging:
- HSG / MRI: Smooth broad indentation of the fundus of the uterine cavity with a normal external uterine contour (no external indentation)
Class VII: DES-Related Anomalies
Mechanism: In utero exposure to diethylstilbestrol (a synthetic oestrogen, now withdrawn).
Imaging findings:
- T-shaped uterine cavity (most common finding)
- Uterine hypoplasia
- Irregular constrictions
- Intraluminal filling defects
(Grainger & Allison, p. 891)
Vaginal Anomalies
Vertical and lateral fusion defects produce vaginal septa, which may cause outflow obstruction and haematocolpos/haematometrocolpos.
| Anomaly | Prevalence | Key Feature |
|---|---|---|
| Imperforate hymen | ~0.1% (most common) | Thin, blue transilluminable membrane at introitus; imaging usually not needed |
| Transverse vaginal septum | Rare | Thicker, pink, non-transilluminable; MRI needed to plan surgery |
| Longitudinal vaginal septum | Common in didelphys (75%) | Often asymptomatic |
MRI of vaginal obstruction:
- Transverse septum: Low signal fibrous tissue on T2 sagittal images with loss of vaginal zonal anatomy
- Haematocolpos/haematometrocolpos: Dilated vagina/uterus with intermediate T2, high T1 fat-suppressed signal (blood products); fluid-debris levels may be present
(Grainger & Allison, p. 891-892)
Imaging Summary Table
| Class | First-Line | Key MRI Finding | External Contour | Cavities | Cervices |
|---|---|---|---|---|---|
| I (Agenesis/MRKH) | MRI | Absent uterus ± vagina; normal ovaries | - | 0 | 0 |
| II (Unicornuate) | MRI | "Banana-like" single horn off midline | Asymmetric | 1 | 1 |
| III (Didelphys) | US + MRI | 2 widely separated full-sized horns; longitudinal septum | Bilobate | 2 | 2 |
| IV (Bicornuate) | MRI | Intercornual cleft ≥1 cm, concave fundus | Concave (≥1 cm) | 2 | 1 (usually) |
| V (Septate) | MRI | Low-T2 septum; outer contour convex/flat/≤1 cm indent | Convex/flat | 2 | 1 |
| VI (Arcuate) | Any | Smooth broad fundal cavity indentation | Normal | 1 | 1 |
| VII (DES) | HSG/MRI | T-shaped cavity | Variable | 1 | 1 |
Associated Anomalies
- Renal anomalies (pelvic kidney, renal agenesis) occur in up to 30% of patients with MDAs, particularly MRKH syndrome. Renal US should always be performed.
- Skeletal anomalies also occur as part of MRKH syndrome.
- Endometriosis is increased with obstructed anomalies (e.g. non-communicating rudimentary horn).
Key Clinical Pearl: Septate vs. Bicornuate Uterus
This is the most clinically important distinction because:
- Septate uterus has the worst obstetric outcome but is surgically correctable (hysteroscopic metroplasty)
- Bicornuate uterus has a better prognosis and surgery is controversial
The critical differentiator is the external fundal contour on coronal oblique T2W MRI:
- Convex/flat outer contour = septate (treat with hysteroscopy)
- Concave outer contour with cleft >1 cm = bicornuate (usually managed conservatively)
HSG and 2D ultrasound cannot reliably make this distinction.
(Grainger & Allison's Diagnostic Radiology, pp. 888-891; Berek & Novak's Gynecology, Table 8-2; Creasy & Resnik's Maternal-Fetal Medicine, p. 981)
Make an essay answer for a radiodiagnosis postgraduate
Here is a structured essay answer written for a radiodiagnosis postgraduate examination:
Müllerian Duct Anomalies: Classification and Imaging
Introduction
Müllerian duct anomalies (MDAs) are congenital malformations of the female genital tract arising from defects in the development, fusion, or resorption of the paired paramesonephric (Müllerian) ducts. They occur in approximately 4-7% of the general female population and up to 25% of women with recurrent pregnancy loss. The ovaries are characteristically spared, as they derive from the urogenital ridge rather than the Müllerian system. MDAs are frequently associated with renal and skeletal anomalies, making a systematic imaging approach imperative. MRI is the gold standard investigation, providing unparalleled soft tissue contrast and multiplanar capability to characterise both uterine morphology and associated anomalies.
Embryology
Normal development of the female reproductive tract requires three sequential processes: (1) development of both Müllerian ducts, (2) fusion of their caudal segments in the midline to form the uterovaginal canal, and (3) resorption of the intervening median septum. Failure at any of these stages produces a corresponding class of anomaly. The upper third of the vagina, uterus, fallopian tubes, and cervix are all Müllerian derivatives. HOX genes (particularly HOXA13) and WNT4 are essential regulatory genes in this process.
Classification
The most widely used system is the American Fertility Society (AFS) classification (Buttram & Gibbons, 1979; revised AFS 1988), which divides MDAs into seven classes based on the degree of Müllerian development failure.
The ESHRE/ESGE classification (2013) is a more recent system that introduces sub-classifications and separately catalogues cervical and vaginal anomalies, but the AFS system remains the dominant framework in clinical radiology practice.
Class I: Segmental Müllerian Agenesis/Hypoplasia
This results from failure of normal development of one or both Müllerian ducts. The ovaries are normal. Subtypes are defined by the segment affected: vaginal (Ia), cervical (Ib), fundal (Ic), tubal (Id), or combined (Ie).
The most important subtype is Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome - uterine and vaginal agenesis or hypoplasia with intact ovaries and fallopian tubes. It is associated with pelvic/horseshoe kidney, skeletal anomalies, and cardiac defects in a significant proportion. Patients present with primary amenorrhoea and normal secondary sexual characteristics.
Imaging: Ultrasound is unreliable for detecting small uterine remnants. Sagittal and axial T2-weighted MRI is the modality of choice, demonstrating absent or rudimentary uterus and upper vagina, normal ovaries (which may be high-riding), and any associated renal anomaly.
Class II: Unicornuate Uterus
Results from failure of development of one Müllerian duct. The contralateral duct may develop a rudimentary horn, which may be:
- IIa: Communicating (with an endometrial cavity connecting to the main horn)
- IIb: Non-communicating (with a functioning endometrial cavity that does not connect - most clinically significant)
- IIc: Non-communicating with no endometrial cavity
- IId: No rudimentary horn
A functioning non-communicating rudimentary horn accumulates blood products (haematometra), causing cyclical pain and significantly increased risk of endometriosis. Ectopic pregnancy may implant within the rudimentary horn.
Imaging: On US and HSG, a unicornuate uterus may be suspected. The definitive diagnosis is on axial oblique T2-weighted MRI, which shows a curved, elongated uterus with tapering of the fundal segment off the midline - the characteristic "banana-shaped" or "spindle-shaped" configuration. Normal uterine zonal anatomy is maintained. The rudimentary horn, if present, is identified separately; a functioning non-communicating horn demonstrates haematometra with high T1 fat-suppressed signal. Renal agenesis ipsilateral to the undeveloped horn is present in up to 40% of cases.
Class III: Uterus Didelphys
Results from complete non-fusion of both Müllerian ducts, producing two fully separate and normally developed uterine horns, each with its own cervix. A longitudinal vaginal septum is present in approximately 75% of cases. This is associated with Herlyn-Werner-Wunderlich (HWW) syndrome when one hemi-vagina is obstructed and the ipsilateral kidney is absent.
Imaging: US demonstrates two separate uterine bodies. Coronal oblique T2-weighted MRI clearly shows two widely separated, full-sized uterine horns each with preserved normal zonal anatomy, two cervices, and frequently two vaginal channels. The intercornual angle is typically wide (>105°). This is distinguished from bicornuate uterus by the complete separation to the level of the cervix and normal size of each horn.
Class IV: Bicornuate Uterus
Results from incomplete fusion of the cephalad portions of the uterovaginal horns, with the lower uterine segment and cervix having fused normally. There is a single cervix in most cases. It is subclassified as complete (Bicornuate bicollis - separate cervices) or partial (Bicornuate unicollis). Obstetric complications are proportional to the degree of non-fusion.
Imaging: HSG demonstrates widely divergent uterine horns but cannot reliably distinguish this from a septate uterus. Coronal oblique T2-weighted MRI is definitive. Key findings are:
- External fundal contour is concave with an intercornual cleft of ≥1 cm (the single most important differentiating feature)
- Two uterine horns, each with normal myometrial signal intensity on all sequences
- A single cervix (usually)
- The inter-cornual distance is typically >4 cm
Class V: Septate Uterus
The most common MDA (accounting for approximately 35% of all cases). Results from failure of resorption of the fibromuscular median septum following normal fusion of the Müllerian ducts. The septum may be partial (not reaching the internal os) or complete (extending to the external cervical os, rarely to the vagina). This is the anomaly with the worst obstetric outcome - the highest rates of first-trimester miscarriage (up to 65%) and fetal malpresentation - yet it is the most surgically correctable by hysteroscopic metroplasty.
Imaging: The critical distinction from bicornuate uterus rests on the external fundal contour:
- In septate uterus, the outer uterine contour is convex, flat, or has only a shallow concavity of ≤1 cm
- Coronal oblique T2-weighted MRI clearly demonstrates the septum as low signal intensity tissue (fibrous) or intermediate signal (muscular/fibromuscular)
- The length and width of the septum are measured to guide surgical planning
- On 2D ultrasound and HSG, the two cavities are visible but the external contour cannot be assessed; hence neither modality can reliably distinguish septate from bicornuate uterus
A fibrous septum (low T2 signal) is associated with worse reproductive outcomes than a muscular septum (intermediate T2 signal).
Class VI: Arcuate Uterus
Considered a normal variant representing near-complete resorption of the median septum, leaving only a smooth, broad, shallow indentation of the fundal uterine cavity. It has no significant independent association with infertility or adverse obstetric outcomes.
Imaging: HSG or MRI shows a smooth, broad, curvilinear indentation of the fundal endometrial cavity with a completely normal external uterine contour. No myometrial tissue protrudes into the cavity.
Class VII: Diethylstilbestrol (DES)-Related Anomalies
Diethylstilbestrol was a synthetic oestrogen administered to pregnant women between the 1940s-1970s to prevent miscarriage. In utero exposure produces a characteristic pattern of uterine abnormalities.
Imaging (HSG): The hallmark is a T-shaped uterine cavity due to constriction bands at the cornua. Associated findings include uterine hypoplasia, irregular luminal constrictions, intraluminal filling defects (pseudopolyps), and cervical hypoplasia. These women also have increased rates of vaginal clear cell adenocarcinoma.
Vaginal Anomalies
Defects of vertical and/or lateral fusion produce vaginal septa. Obstruction leads to accumulation of secretions (hydrocolpos) or blood (haematocolpos, haematometrocolpos) and cyclical pelvic pain in post-pubertal females.
Imperforate hymen (prevalence ~0.1%) is the most common obstructive anomaly. On clinical examination it is a thin, blue, transilluminable membrane. Imaging is usually not required, but if performed, US/MRI shows a fluid- or blood-filled vagina.
Transverse vaginal septum is thicker, non-transilluminable, and located at variable levels. MRI (sagittal T2WI) identifies the septum as a low signal fibrous band with loss of normal vaginal zonal anatomy, and delineates the precise length of the defect for pre-operative planning. Haematometrocolpos appears as a distended vagina and uterus with intermediate T2 and high T1 fat-suppressed signal (blood products), often with fluid-debris levels.
Longitudinal vaginal septum most commonly accompanies didelphys uterus. It may be partial or complete and is often asymptomatic.
Critical Differential: Septate vs. Bicornuate Uterus
This is the most clinically consequential distinction in MDA imaging because it dictates management:
| Feature | Septate (Class V) | Bicornuate (Class IV) |
|---|---|---|
| External fundal contour | Convex/flat/concave ≤1 cm | Concave, cleft >1 cm |
| Intercornual angle | <75° | >105° |
| Septum signal on T2W | Low (fibrous) or intermediate | N/A - myometrium (normal signal) |
| Fundal myometrium | Intact, uninterrupted | Deep cleft reaching myometrium |
| Surgical treatment | Hysteroscopic metroplasty | Usually conservative |
| Prognosis post-surgery | Excellent | Surgery not routinely indicated |
HSG and 2D ultrasound are insufficient to make this distinction. 3D ultrasound (coronal plane reconstruction) approaches MRI accuracy and is the preferred first-line non-invasive investigation. MRI remains definitive.
Role of Imaging Modalities - Summary
| Modality | Role |
|---|---|
| 2D Ultrasound | First-line screening; limited for external contour assessment |
| 3D Ultrasound / SHG | Highly accurate; approaches MRI; preferred first-line investigation |
| HSG | Delineates uterine cavity; cannot assess external contour; cannot differentiate septate from bicornuate |
| MRI | Gold standard; assesses external contour, septum composition, zonal anatomy, associated anomalies |
| Hysteroscopy | Therapeutic and diagnostic; only intracavitary view |
Associated Anomalies
Renal anomalies (pelvic kidney, horseshoe kidney, unilateral renal agenesis, duplex collecting systems) occur in up to 30% of MDA patients. The ipsilateral kidney to the undeveloped Müllerian duct is most frequently affected. Renal ultrasound is mandatory in all patients with confirmed MDAs.
Conclusion
Müllerian duct anomalies represent a wide spectrum of congenital uterine malformations with significant implications for reproductive health. The AFS seven-class system provides the standard clinical framework. MRI, with dedicated T2-weighted coronal and axial oblique sequences, is the definitive imaging modality - its ability to assess both the internal uterine architecture and the external fundal contour is critical, particularly in distinguishing the treatable septate uterus from the bicornuate uterus. A systematic approach incorporating ultrasound, HSG where appropriate, and MRI, combined with renal screening, ensures complete characterisation and optimal management planning.
Sources: Grainger & Allison's Diagnostic Radiology (pp. 888-892); Berek & Novak's Gynecology (Table 8-2); Creasy & Resnik's Maternal-Fetal Medicine (p. 981)
This is a shared conversation. Sign in to Orris to start your own chat.