My working diagnosis is acute decompensated heart failure. Give me the latest 2025/2026 guideline-directed medical therapy with citations."
Reading File
Finding Sources
Searching PubMed
"acute decompensated heart failure" AND "guideline" AND management
Searching the Web
2025 2026 ACC AHA ESC guidelines acute decompensated heart failure GDMT treatment
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12979370
Searching PubMed
"acute heart failure" AND ("SGLT2" OR "sacubitril" OR "decongestion" OR "GDMT")
Loading Image
Reading Article
PMID: 42201275
Reading File
I now have comprehensive data from Harrison's 2025, the 2026 PMC evidence update, AHA 2025 guidelines summary, the JACC 2026 review, and key PubMed citations. Let me compile the full answer.
Acute Decompensated Heart Failure (ADHF): 2025/2026 Guideline-Directed Medical Therapy
Phenotype-Based Framework (Harrison's 2025)
The fundamental first step is phenotyping the presentation, as therapy is directed by hemodynamic profile:
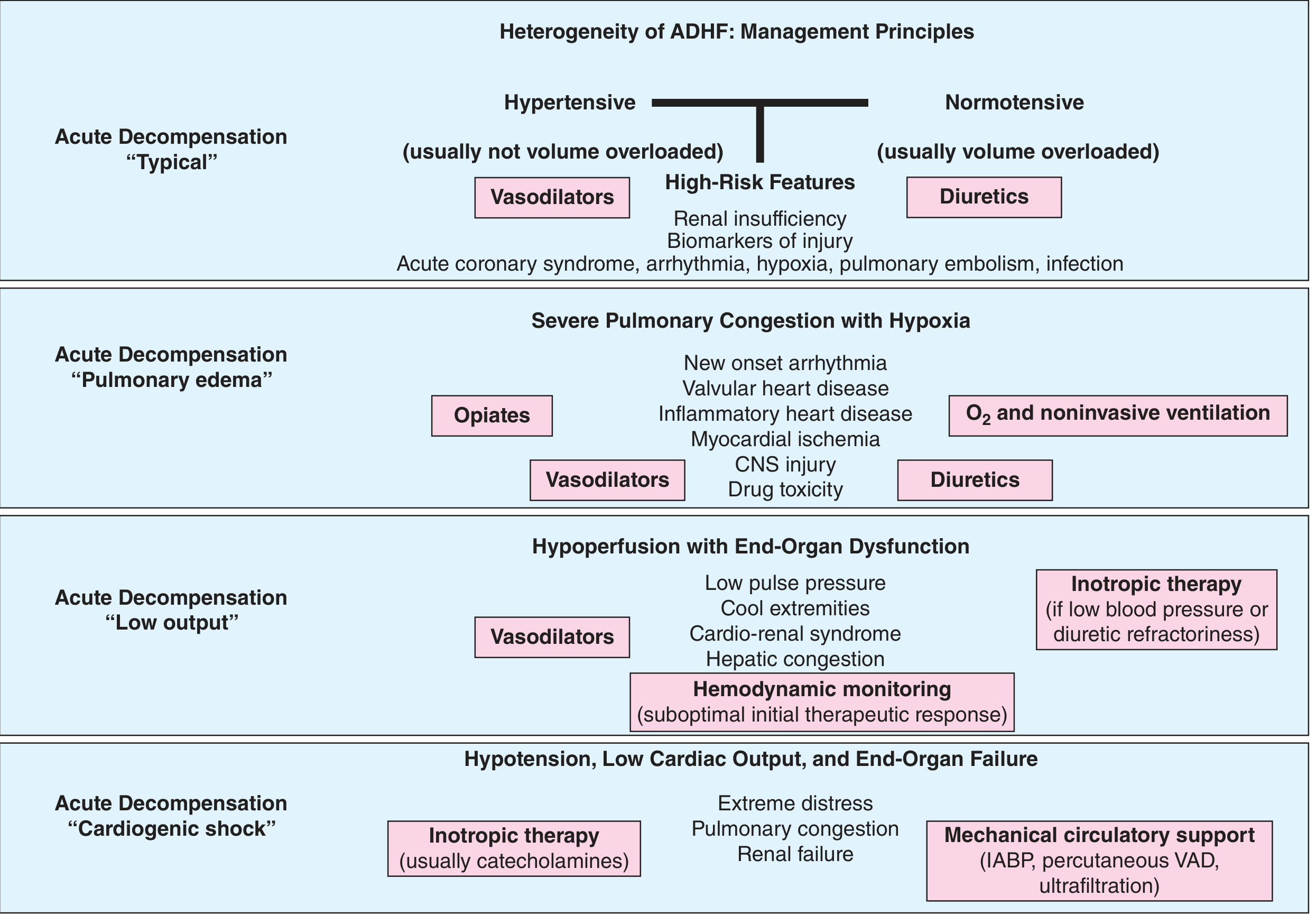
Figure 265-2 from Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
| Phenotype | Key Features | Primary Therapy |
|---|---|---|
| "Typical" - Hypertensive | Elevated BP, usually not volume overloaded | Vasodilators |
| "Typical" - Normotensive | Volume overloaded, elevated JVP, edema | IV Diuretics |
| "Pulmonary edema" | Severe congestion + hypoxia | O2/NIV + Vasodilators + Diuretics |
| "Low output" | Cool extremities, cardiorenal syndrome | Vasodilators ± Inotropes + monitoring |
| "Cardiogenic shock" | Hypotension, end-organ failure | Inotropes (catecholamines) + MCS |
Step 1: Identify and Treat Precipitants (All Cases)
Before or concurrent with hemodynamic therapy, systematically evaluate for:
- Medication nonadherence / dietary salt excess (most common)
- Ischemia - investigate and consider revascularization in all patients with atherosclerotic CVD
- Arrhythmia (AF, VT) - antiarrhythmic therapy, cardioversion, or ablation as appropriate
- Valvular disease - echocardiography to identify candidates for intervention
- Infection / pulmonary embolism
- Nephrotoxins: NSAIDs, thiazolidinediones, TNF inhibitors, some antidepressants, cold/flu preparations, selected chemotherapy agents
Harrison's Principles of Internal Medicine, 22nd Ed. (2025), p. 2033
Step 2: Immediate Pharmacologic Management
A. Decongestion - IV Loop Diuretics (FIRST PRIORITY)
- Initiate IV loop diuretic within 1 hour of presentation (AHA 2025, Class I)
- Starting dose should equal or exceed the patient's chronic oral daily dose
- Bolus vs. continuous infusion: no definitive superiority of one over the other from RCT data - use clinical judgment
- Target: euvolemia (JVP normalization, clearance of rales, resolution of edema) - residual congestion drives readmission
- Monitor: urine output, daily weight, serum electrolytes, creatinine
Diuretic resistance strategies (when initial loop diuretics fail):
- Sequential nephron blockade: add thiazide (metolazone, chlorothiazide) or hydrochlorothiazide on top of loop diuretic. The CLOROTIC trial confirmed hydrochlorothiazide significantly improved weight loss vs. placebo in patients on oral furosemide admitted for decompensation (monitor for hypokalemia and creatinine rise)
- Acetazolamide (ADVOR trial): facilitates greater decongestion but no reduction in HF readmission or mortality - use selectively
- Ultrafiltration (aquapheresis): reserved for patients refractory to maximal diuretic therapy; controlled fluid removal with electrolyte-neutral effect
- A 2025 systematic review and meta-analysis (Fioretti et al., Eur J Heart Fail 2025, PMID 41367306) confirmed combination diuretic therapy improves decongestion in ADHF
Natriuresis-guided therapy: Consider monitoring urine sodium as a marker of diuretic response. Spot urinary Na <50-70 mmol/L at 2 hours predicts suboptimal response and should prompt dose escalation or combination strategy. The 2026 JACC review by Bruno et al. supports natriuresis-guided therapy as standard of care (PMID 42201275).
B. Vasodilators (Hypertensive / Pulmonary Edema Phenotype)
- IV nitroglycerin or nitroprusside for patients with elevated systolic BP (>140 mmHg) and volume redistribution ("flash pulmonary edema" pattern)
- Reduce preload and afterload rapidly
- Do not use in hypotensive or low-output patients
C. Oxygen / Non-Invasive Ventilation
- Titrate O2 to SpO2 ≥92-94% - do not target hyperoxemia
- The 2026 ESC Heart Failure meeting presented the Redox A-CHF trial confirming that restrictive oxygenation (SpO2 ~90%) leads to significantly greater reduction in estimated lung fluid content vs. liberal O2 (>96%) in ADHF - now guideline-endorsed
- NIV (CPAP/BiPAP): first-line for acute cardiogenic pulmonary edema with hypoxia. Reduces need for intubation
- Opiates (morphine): use cautiously - may reduce dyspnea and venodilate, but associated with adverse outcomes in some registries
D. Inotropic Therapy (Low-Output / Cardiogenic Shock)
- Reserved for hypoperfusion states: low pulse pressure, cold extremities, rising lactate, oliguria, hepatic congestion
- Options: dobutamine (preferred), milrinone (alternative, especially with beta-blocker use or pulmonary hypertension), norepinephrine (cardiogenic shock with hypotension)
- Use lowest effective dose; bridge to recovery, definitive therapy (LVAD, transplant), or palliation
- Avoid long-term intermittent inotropic therapy - no mortality benefit and potentially harmful (AHA 2025)
- Pulmonary artery catheter: not routine - reserve for refractory cases, suspected cardiogenic shock, complex cardiorenal syndrome, or suspected pulmonary arterial hypertension
E. Mechanical Circulatory Support (Cardiogenic Shock)
- IABP (intra-aortic balloon pump): widely available, modest hemodynamic benefit
- Percutaneous VAD (Impella, TandemHeart): stronger hemodynamic support for refractory cardiogenic shock
- Consider as bridge to decision (recovery, LVAD, or cardiac transplantation)
Harrison's Principles of Internal Medicine, 22nd Ed. (2025), pp. 2033-2035
Step 3: The Paradigm Shift - In-Hospital GDMT Initiation (2025/2026 KEY UPDATE)
"Management of AHF has shifted from focusing solely on symptomatic decongestion to the rapid initiation of disease-modifying therapies during hospitalization."
The STRONG-HF secondary analysis demonstrated that rapid GDMT uptitration has a significant decongestive and diuretic-sparing effect, shifting the paradigm from diuretic-centered to GDMT-centered decongestion.
Quadruple GDMT (HFrEF, LVEF <40%) - Initiate/Continue During Hospitalization
| Drug Class | Agent(s) | Notes |
|---|---|---|
| SGLT2 inhibitor | Empagliflozin 10 mg or Dapagliflozin 10 mg | Start during hospitalization regardless of diabetes. Benefit across the EF spectrum. 2025 CCS/CHFS and JCS/JHFS guidelines incorporated SGLT2i into HFnrEF (HFmrEF + HFpEF) algorithms |
| ARNI | Sacubitril/valsartan | Preferred over ACEi/ARB in HFrEF tolerating neurohormonal therapy. ESC permits as first-line; AHA/ACC/HFSA allows first-line initiation |
| ACEi or ARB | Ramipril, enalapril, lisinopril; losartan, valsartan | Use if ARNI not tolerated. Continue unless hemodynamically unstable during ADHF |
| Beta-blocker | Carvedilol, metoprolol succinate, bisoprolol | Continue in compensated patients. In newly decompensated HFrEF, do not start until euvolemic and hemodynamically stable. Reduce dose if fluid overloaded but avoid abrupt discontinuation |
| MRA | Spironolactone or eplerenone | Continue or initiate once renal function and potassium are acceptable |
Important: NICE 2025 guidelines moved away from rigid drug-sequencing toward patient-centered, simultaneous initiation of all four pillars when clinically feasible, based on the patient's history, frailty, prognosis, and preferences. (Medscape/NICE 2025 summary)
SGLT2i in ADHF - Special Note
- Start empagliflozin or dapagliflozin as soon as clinically feasible during the hospitalization (even within 24-48 hours of admission)
- The 2025 Canadian (CCS/CHFS) and Japanese (JCS/JHFS) guidelines now explicitly recommend SGLT2i across the EF spectrum (HFrEF, HFmrEF, HFpEF)
- Evidence supports osmotic diuretic + natriuretic effects that aid decongestion
HFpEF and HFmrEF (LVEF ≥40%)
- SGLT2 inhibitor: recommended (empagliflozin/dapagliflozin) - Class IIa, AHA/ACC/HFSA; now Class I in 2025 Canadian guidelines
- Finerenone (non-steroidal MRA): REDEFINE-HF trial (NCT06008197) ongoing for post-acute HFmrEF/HFpEF - results anticipated; guideline position may change
- ARNI: reasonable to use in HFpEF; 2025 CCS guidelines support this
- Diuretics: still cornerstone for symptom relief in volume-overloaded HFpEF
Step 4: Monitoring Parameters
During hospitalization (daily):
- Fluid intake/output, body weight
- Heart rate, rhythm, blood pressure, SpO2
- Serum electrolytes (Na, K, Mg), creatinine, BUN
- BNP or NT-proBNP (pre-discharge level strongly predicts post-discharge mortality and readmission)
- Signs of congestion (JVP, rales, edema)
High-risk predictors for worse outcome (Harrison's 2025):
- BUN >43 mg/dL
- sBP <115 mmHg
- Creatinine >2.75 mg/dL
- Elevated troponin or markedly elevated natriuretic peptides
Step 5: Pre-Discharge and Transition Planning
- Do not discharge with residual congestion - this is the strongest modifiable predictor of 30-day readmission
- Pre-discharge BNP/NT-proBNP measurement to stratify risk
- Resume/optimize oral loop diuretic at discharge
- Ensure quadruple GDMT is prescribed before discharge (or documented rationale for omission)
- "High-intensity care" strategy: rapid up-titration of quadruple therapy with frequent clinical and laboratory reassessment (AHA 2025)
- Early follow-up: telephone contact within 3 days post-discharge; in-person visit within 7-14 days
Medications to Avoid in ADHF / Heart Failure
| Drug Class | Reason |
|---|---|
| Calcium channel blockers (diltiazem, verapamil) | Worsen HF and increase hospitalization |
| NSAIDs / COX-2 inhibitors | Worsen fluid retention, blunt ACEi efficacy |
| Class I antiarrhythmics | Proarrhythmic, negative inotropic |
| Thiazolidinediones | Fluid retention |
| Long-term intermittent inotropic therapy | No mortality benefit, potentially harmful |
Key 2025/2026 Citations
| Source | Reference |
|---|---|
| Harrison's Principles of Internal Medicine 22E | Harrison's (McGraw Hill, 2025), Chapter 265, pp. 2033-2036 |
| AHA 2025 HF Guideline Update | AHA 2025 HF Guidelines summary |
| NICE 2025 HFrEF Guideline | Medscape/NICE 2025 Expert Insight |
| 2025 CCS/CHFS + JCS/JHFS Guidelines | Incorporated into Heart Failure Evidence Update 2026, PMC12979370 |
| JACC 2026 Review (Bruno J et al.) | Contemporary Management of AHF: From Emergency to Long-Term Remission. JACC 2026. PMID 42201275 |
| Combination Diuretic Therapy Meta-Analysis | Fioretti F et al. Eur J Heart Fail 2025. PMID 41367306 |
| Diuretic Potentiation Strategies | Siddiqi TJ, Packer M et al. JACC Heart Fail 2025. PMID 39779178 |
| Paradigm shift review (Biegus J et al.) | Decongestion in AHF: Changing diuretic-centred paradigm. Eur J Heart Fail 2024. PMID 39169731 |
| International Expert Consensus | Cotter G, Biegus J, Fudim M et al. Eur J Heart Fail 2025. PMID 41015948 |
| ESC Heart Failure 2026 Highlights | ESC TV - Heart Failure 2026 |
Clinical bottom line for 2025/2026: The era of "decongest first, optimize later" is over. The hospitalization should now serve a dual purpose - (1) achieve full decongestion with phenotype-directed diuretics/vasodilators, and (2) initiate or optimize all four pillars of GDMT (SGLT2i + ARNI/ACEi/ARB + beta-blocker + MRA) before discharge, guided by the patient's hemodynamic tolerance. SGLT2 inhibitors are now recommended across the full EF spectrum.
This is a shared conversation. Sign in to Orris to start your own chat.