Antiparkinson drug
Reading File
Finding Sources
Searching PubMed
"Parkinson disease" AND "pharmacotherapy"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Antiparkinson Drugs
Parkinson disease (PD) results from progressive degeneration of dopaminergic neurons in the substantia nigra, leading to dopamine depletion in the neostriatum. All current drugs offer symptomatic relief - none halt neuronal degeneration. The key principle is restoring the dopamine/acetylcholine balance in the basal ganglia.
Pathophysiology Basis
The loss of nigrostriatal dopamine leads to:
- Bradykinesia (most responsive to treatment)
- Rigidity
- Resting tremor
- Postural instability
Drug Classes
1. Levodopa + Carbidopa (Gold Standard)
Mechanism:
Dopamine itself cannot cross the blood-brain barrier (BBB). Levodopa, its immediate precursor, is actively transported across the BBB and converted to dopamine in residual nigrostriatal neurons.
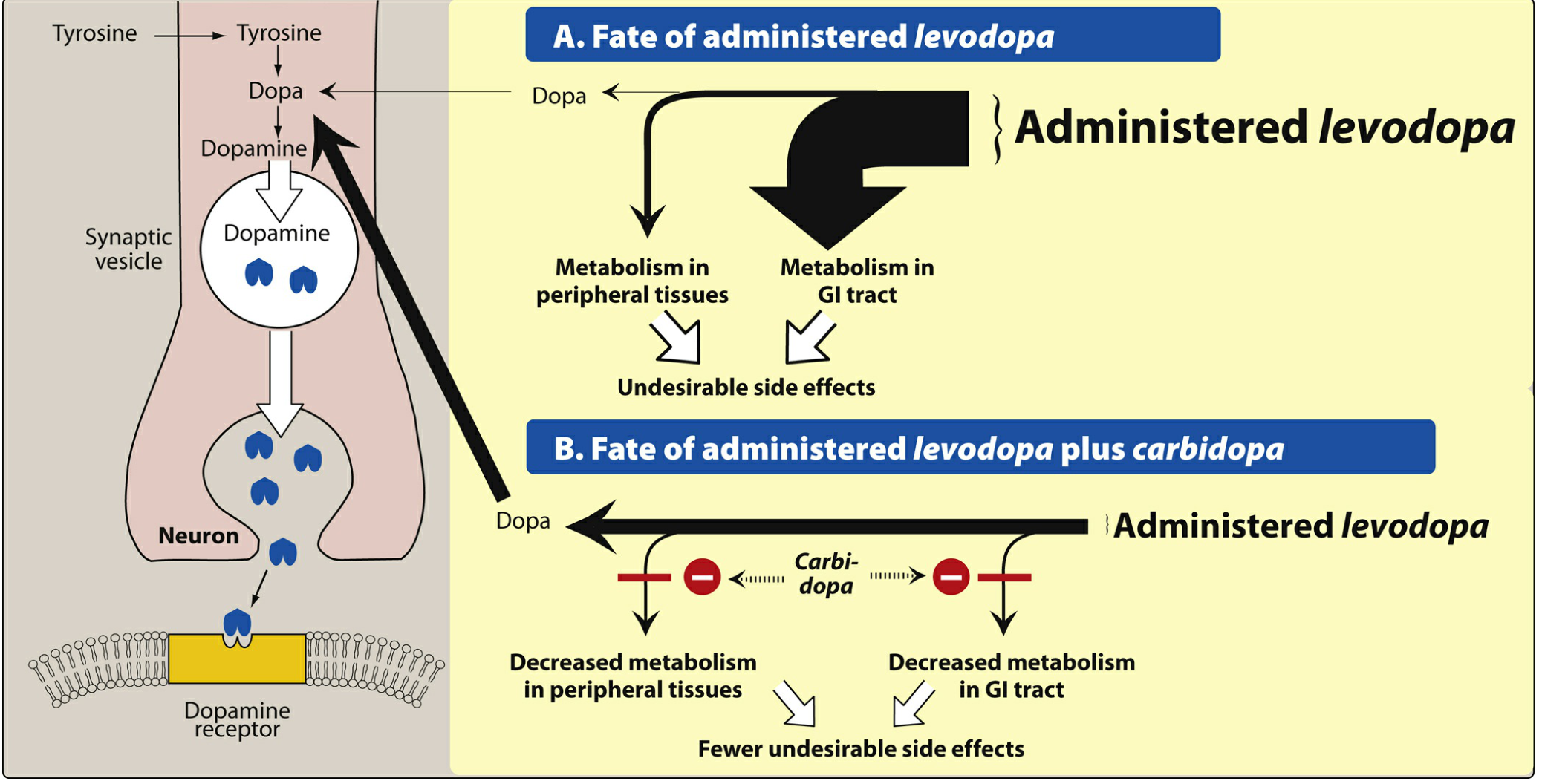
- Carbidopa is a peripheral DOPA decarboxylase inhibitor that cannot cross the BBB. It blocks conversion of levodopa to dopamine in the periphery, reducing the required dose 4-5 fold and markedly reducing peripheral side effects (nausea, vomiting, arrhythmias, hypotension).
- Usual starting dose: carbidopa/levodopa 25 mg/100 mg three times daily.
Therapeutic uses:
- First-line for PD, most effective for bradykinesia; also reduces rigidity and tremor.
- About two-thirds of patients respond substantially for the first 3-5 years, then response declines.
Adverse effects:
- Peripheral: Nausea, vomiting, orthostatic hypotension, cardiac arrhythmias
- Central: Dyskinesias (choreoathetosis), "on-off" fluctuations, wearing-off phenomenon, hallucinations, confusion
- The on-off phenomenon: unpredictable switches between mobile ("on") and immobile ("off") states, related to short plasma half-life (1-2 hours)
Key drug interactions:
- Pyridoxine (B6) enhances peripheral metabolism of levodopa - avoided without carbidopa
- MAO inhibitors (non-selective): hypertensive crisis risk
- Antipsychotics: block dopamine receptors, worsen parkinsonism
(Lippincott Pharmacology, p. 515-517; Katzung, p. 780)
2. Dopamine Receptor Agonists
These directly stimulate dopamine receptors (D2 > D3) without requiring conversion in surviving neurons - useful in advanced disease where neuron count is very low.
| Drug | Type | Route | Notes |
|---|---|---|---|
| Bromocriptine | Ergot | Oral | Older; risk of fibrosis, vasospasm |
| Pramipexole | Non-ergot | Oral | D3 preferring; also for restless legs |
| Ropinirole | Non-ergot | Oral | Also for restless legs |
| Rotigotine | Non-ergot | Transdermal patch | Once-daily; steady levels |
| Apomorphine | Non-ergot | SC injection / sublingual | Rescue for acute "off" episodes |
Advantages over levodopa:
- Longer duration of action - fewer "on-off" fluctuations
- Fewer dyskinesias (especially in early therapy)
- May delay need for levodopa initiation in early PD
Adverse effects:
- Nausea, vomiting, orthostatic hypotension
- Hallucinations, confusion (more common than with levodopa)
- Impulse control disorders - compulsive gambling, hypersexuality, binge eating (up to 45% prevalence) - related to D2/D3 mesocorticolimbic activation
- Sudden-onset sleep ("sleep attacks") - especially pramipexole and ropinirole
- Ergot-specific: pulmonary/retroperitoneal fibrosis, erythromelalgia, cardiac valvulopathy (pergolide)
Contraindications: History of psychosis, recent MI, active peptic ulcer; ergot derivatives - avoid in peripheral vascular disease.
(Lippincott Pharmacology, p. 524-527; Katzung, p. 782-783)
3. MAO-B Inhibitors
Mechanism: Monoamine oxidase B selectively metabolizes dopamine in the brain. Inhibiting it raises dopamine levels in the striatum.
| Drug | Dose | Use |
|---|---|---|
| Selegiline (deprenyl) | 5 mg with breakfast + 5 mg with lunch | Adjunct to levodopa |
| Rasagiline | 0.5-1 mg/day | Monotherapy (mild disease) or adjunct |
| Safinamide | 50-100 mg/day | Adjunct in fluctuating patients |
- Selegiline is metabolized to amphetamine and methamphetamine (may cause insomnia - avoid evening doses).
- Rasagiline is more potent; used as monotherapy for early disease.
- Both may have modest neuroprotective effects (MPTP animal models - MAO-B converts MPTP to the toxic MPP+), but human evidence is inconclusive.
- At high doses, selegiline loses MAO-B selectivity and can cause hypertensive crisis with tyramine-rich foods ("cheese reaction").
(Katzung, p. 783-784)
4. COMT Inhibitors
Mechanism: Catechol-O-methyltransferase (COMT) metabolizes levodopa peripherally. Blocking COMT extends the half-life of levodopa, reducing "wearing-off."
| Drug | Site of action | Key feature |
|---|---|---|
| Entacapone | Peripheral only | Preferred - no hepatotoxicity; given with each levodopa dose |
| Tolcapone | Peripheral + central | Risk of fatal hepatotoxicity - requires LFT monitoring |
| Opicapone | Peripheral | Once-daily dosing |
- COMT inhibitors are always used as adjuncts to levodopa/carbidopa - never alone.
- Entacapone + carbidopa + levodopa is available as a fixed combination (Stalevo).
- Main side effects: diarrhea, orange discoloration of urine, dyskinesias (from enhanced levodopa effect), hepatotoxicity (tolcapone).
(Katzung, p. 579-585; Harrison's, 2025)
5. Amantadine
Originally an antiviral drug, accidentally found to have antiparkinsonian activity.
Mechanisms:
- Stimulates dopamine release from presynaptic terminals
- Blocks NMDA-type glutamate receptors (anti-dyskinetic effect)
- Mild anticholinergic activity
Clinical use:
- Mild early PD (monotherapy)
- Reducing levodopa-induced dyskinesias in advanced disease
- Less efficacious than levodopa; tolerance often develops within weeks
Adverse effects: Restlessness, hallucinations, confusion, livedo reticularis, peripheral edema, urinary retention, dry mouth. Abrupt withdrawal can cause acute confusional state and parkinsonism worsening.
(Katzung, p. 785; Lippincott, p. 528)
6. Adenosine A2A Receptor Antagonist
Istradefylline (analog of caffeine): Selective A2A antagonist. Taken 20-40 mg/day as adjunct to carbidopa-levodopa to reduce "off" time. Side effects include dyskinesias and hallucinations.
7. Anticholinergic (Antimuscarinic) Agents
Drugs: Benztropine, trihexyphenidyl, biperiden, procyclidine
Mechanism: In PD, dopamine depletion leaves acetylcholine relatively unopposed. Blocking muscarinic receptors corrects this imbalance.
Effects: Improve tremor and rigidity, but little effect on bradykinesia. Less effective than levodopa overall - used as adjuncts, especially in younger patients with prominent tremor.
Adverse effects: Classic anticholinergic - dry mouth, constipation, urinary retention, blurred vision, confusion (especially in elderly).
Contraindications: Glaucoma, prostatic hypertrophy, cognitive impairment.
Summary Table
| Drug Class | Key Drugs | Main Mechanism | Best Used For |
|---|---|---|---|
| Levodopa + carbidopa | Sinemet, Rytary | Dopamine precursor | All stages - first-line |
| DA agonists | Pramipexole, ropinirole | Direct D2/D3 agonism | Early disease (delay levodopa), fluctuations |
| MAO-B inhibitors | Selegiline, rasagiline | Block DA breakdown | Early monotherapy, adjunct |
| COMT inhibitors | Entacapone, tolcapone | Extend levodopa half-life | Wearing-off phenomenon |
| Amantadine | Amantadine | NMDA block, DA release | Mild disease, dyskinesias |
| Anticholinergics | Benztropine, trihexyphenidyl | Block ACh excess | Tremor, rigidity (adjunct) |
| A2A antagonist | Istradefylline | Block adenosine A2A | Reduce "off" time |
Complications of Long-term Levodopa Therapy
- Wearing-off ("end-of-dose" deterioration): PD symptoms return before next dose; managed by reducing dosing intervals, adding COMT inhibitor or MAO-B inhibitor.
- On-off phenomenon: Unpredictable motor fluctuations - managed by extended-release formulations, COMT inhibitors, or deep brain stimulation (DBS).
- Dyskinesias: Involuntary movements at peak dose - managed by dose reduction, amantadine, or DBS.
- Drug holiday (rarely used): Temporary withdrawal to restore levodopa responsiveness - significant risk of neuroleptic malignant-like syndrome.
Non-pharmacological Option
Deep brain stimulation (DBS) of the subthalamic nucleus or globus pallidus interna is indicated for patients with motor fluctuations or dyskinesias refractory to pharmacologic optimization.
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 515-530; Katzung's Basic & Clinical Pharmacology 16e, p. 780-790; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's Principles of Internal Medicine 22e (2025)
This is a shared conversation. Sign in to Orris to start your own chat.