A person's left kidney is atrophic and not visible in USG whereas right one is perfectly normal. He found out during routine USG. What could be the reason.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Excellent - I now have the diagram and all the key information needed. Let me compile a comprehensive answer.
Here is a thorough answer based on authoritative textbook sources:
Unilateral Left Renal Atrophy - Causes
The scenario you describe - an atrophic, non-visualized left kidney found incidentally on USG with a normal right kidney - is a classic clinical finding. The right kidney has undergone compensatory hypertrophy, which is why it appears normal and may even be slightly larger than expected. This is actually a key clue: when one kidney fails early in life or gradually loses function, the contralateral kidney enlarges to compensate.
Here is the landmark reference diagram from Comprehensive Clinical Nephrology that maps all causes of a small/absent kidney by appearance and laterality:
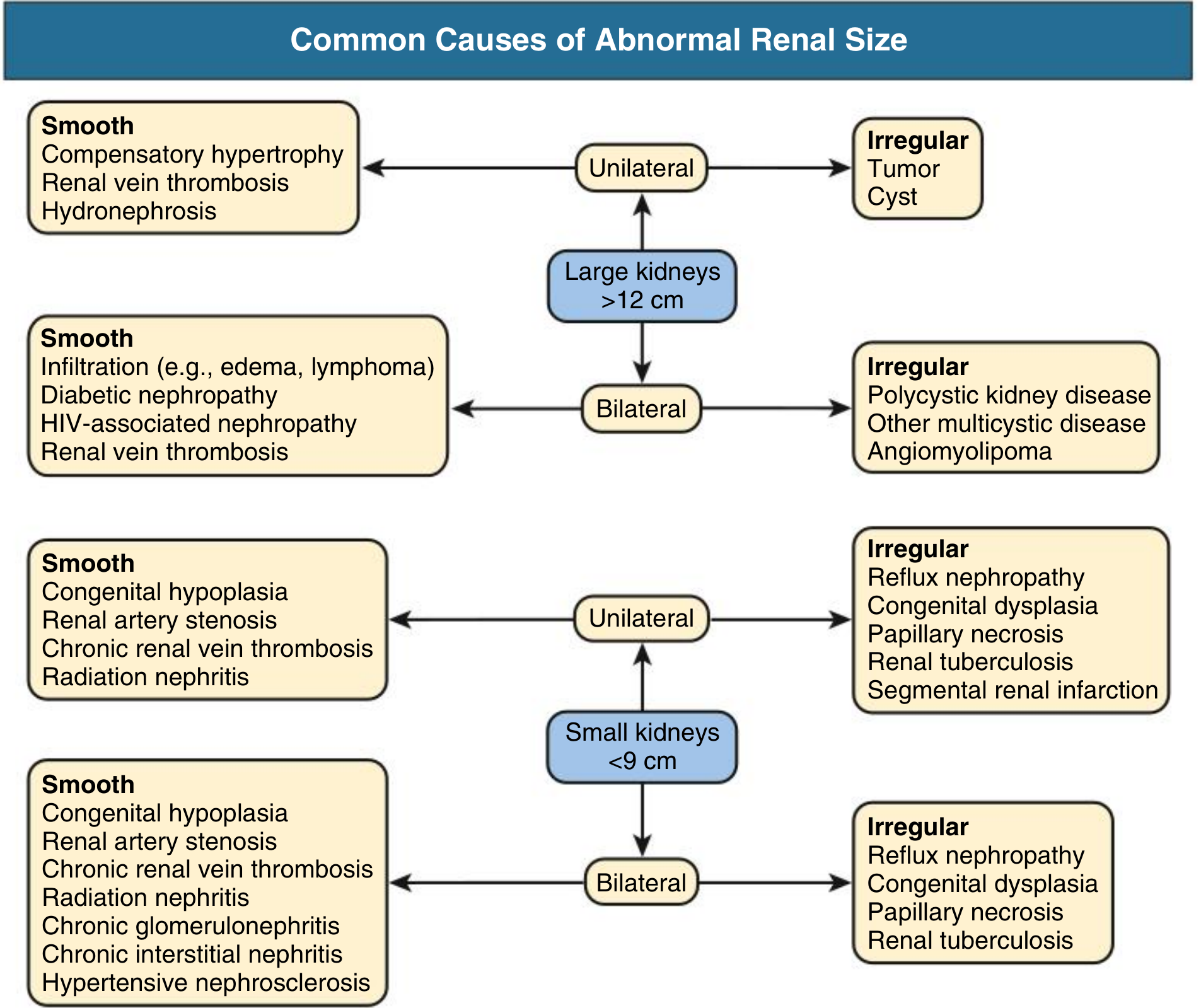
Causes - Smooth Small/Absent Kidney (Unilateral)
These conditions produce a small kidney with a smooth outline, or the kidney may be so atrophic it is not visualized at all:
1. Renal Agenesis (Congenital Absence)
The most common reason a kidney is completely non-visualizable. The ureteric bud (from the Wolffian duct) failed to develop or failed to reach the metanephros. Without a drainage system, the metanephric mass undergoes atrophy. The ureter is absent in ~50% of cases. This is usually found incidentally on imaging, causes no symptoms, and is associated with compensatory hypertrophy of the opposite kidney. Associated anomalies (cardiac, vertebral, genital) may coexist (VACTERL spectrum).
- Smith and Tanagho's General Urology, 19th Ed.
2. Congenital Hypoplasia
The kidney formed but is small - total renal mass divided unequally. One kidney is small while the other is correspondingly larger. Some "hypoplastic" kidneys turn out to be dysplastic on pathology. Differentiation from acquired atrophy is difficult on imaging alone.
- Smith and Tanagho's General Urology
3. Renal Artery Stenosis (RAS)
A narrowed renal artery causes chronic ischemia, leading to progressive shrinkage of the affected kidney. This is particularly common in:
- Atherosclerosis (older patients, often incidental) - the most common cause in adults >50 years
- Fibromuscular dysplasia (FMD) - more common in younger women
"A discrepancy in kidney size of >2 cm suggests chronic disease in a unilateral kidney, such as that seen in renal artery stenosis with atrophy of the affected kidney." Associated hypertension is a key clue - and the hypertension can be cured or improved by revascularization or nephrectomy.
- Washington Manual of Medical Therapeutics; Smith and Tanagho's General Urology
4. Renal Artery Embolism / Thromboembolism
Atheroembolism or thromboembolism (e.g., in patients with atrial fibrillation) can cause infarction of the kidney with subsequent atrophy. This is frequently asymptomatic and discovered incidentally years after the event.
- Symptom to Diagnosis, 4th Ed.
5. Chronic Renal Vein Thrombosis
Can also lead to a small, atrophic kidney unilaterally.
6. Radiation Nephritis
Prior radiotherapy to the left upper abdomen (e.g., for gastric, pancreatic, or lymphoma treatment) can cause radiation nephritis and progressive left renal atrophy.
Causes - Irregular Small Kidney (Unilateral)
These produce a small, scarred kidney with an irregular outline:
7. Reflux Nephropathy (Chronic Pyelonephritis)
The most common cause of a small, scarred kidney in children and young adults. Vesicoureteral reflux (VUR) allows infected urine to ascend to the kidney, causing recurrent episodes of pyelonephritis, scarring, cortical thinning, calyceal clubbing, and progressive atrophy. "Reflux nephropathy often goes unnoticed until early adulthood." VUR may have been undiagnosed in childhood, and the patient presents as an adult with an incidentally found small left kidney.
- Harrison's Principles of Internal Medicine 22E; Grainger & Allison's Diagnostic Radiology
8. Renal Tuberculosis
Mycobacterium tuberculosis can cause granulomatous destruction of renal parenchyma, scarring, calcification, and ultimately an end-stage "putty kidney" or autonephrectomy. Often clinically silent for years.
9. Segmental Renal Infarction
Focal or segmental infarcts from emboli or vasculitis leave permanent scars and cortical loss. Over time, the kidney becomes small and irregularly scarred.
10. Congenital Dysplasia
Abnormal differentiation of the metanephric blastema leads to a dysplastic kidney - often small, with primitive ducts, cartilage, or cysts on histology. May be the underlying pathology behind what appears to be "hypoplasia."
11. Papillary Necrosis
Can cause segmental cortical loss and irregular scarring.
Why Is the Kidney "Not Visible" on USG?
An atrophic kidney can be truly non-visualizable because:
- It is extremely small (<3-4 cm) and blends with surrounding retroperitoneal fat
- Heavy echogenicity from fibrosis/scarring makes it indistinguishable from perinephric fat
- Overlying bowel gas obscures the left renal fossa
If truly not seen, CT scan or a DMSA nuclear scan are the next steps to confirm whether the kidney is absent vs. extremely atrophic vs. ectopic (pelvic, intrathoracic kidneys can be missed on USG).
Key Clinical Differentiators
| Feature | Agenesis/Hypoplasia | RAS | Reflux Nephropathy | TB |
|---|---|---|---|---|
| Age of presentation | Any (usually young) | Older adults | Young adults | Any |
| Hypertension | No (unless solitary) | Yes - often refractory | Can occur | Rare |
| USG outline | Absent / smooth | Smooth, small | Irregular, scarred | Irregular, calcified |
| Contralateral kidney | Compensatory hypertrophy | Usually normal | Usually normal | Usually normal |
| History | None | Vascular risk factors | Recurrent UTIs in childhood | TB exposure |
Bottom Line
In an asymptomatic person found incidentally to have a non-visualizable left kidney, the most likely causes in order of probability are:
- Renal agenesis (congenital) - if truly absent from birth
- Reflux nephropathy - end-stage scarred/atrophic kidney from childhood VUR
- Renal artery stenosis with ischemic atrophy
- Congenital hypoplasia/dysplasia
- Old renal artery embolism/thrombosis (especially in older patients with AF)
- Renal tuberculosis (in endemic regions)
A DMSA scan to confirm the non-functional nature, Doppler USG of the right renal artery (to check for compensatory hypertrophy-related changes), blood pressure measurement, and urine analysis are the appropriate next steps.
- Comprehensive Clinical Nephrology, 7th Ed., Fig. 6.1
- Smith and Tanagho's General Urology, 19th Ed., pp. 534-535
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed.
- Harrison's Principles of Internal Medicine, 22E
- Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.