Physiology of menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed answer.
Physiology of the Menstrual Cycle
The menstrual cycle is a finely orchestrated series of hormonal, ovarian, and uterine events designed to prepare the female reproductive system for fertilization and implantation. The average cycle lasts 28 days (range 21-35 days), and by convention, day 1 is the first day of menstrual bleeding.
Overview: Two Parallel Cycles
The cycle is best understood as two synchronized cycles running in parallel:
| Ovarian Cycle | Uterine Cycle |
|---|---|
| Follicular phase (days 1-14) | Proliferative phase (days 1-14) |
| Ovulation (day 14) | - |
| Luteal phase (days 14-28) | Secretory phase (days 14-28) |
Neuroendocrine Axis
The entire cycle is governed by a hypothalamus - anterior pituitary - ovary axis.
- The hypothalamic arcuate nucleus secretes GnRH (gonadotropin-releasing hormone) in a pulsatile fashion into the hypophyseal portal circulation. Pulse frequency determines the relative secretion of LH vs FSH: slower pulses favor FSH; faster pulses favor LH.
- GnRH stimulates the anterior pituitary to release FSH and LH.
- The ovary responds with follicular development, steroidogenesis, and ovulation.
"The pulse frequency determines the relative amounts of LH and FSH secretion." - Berek & Novak's Gynecology, p. 264
Phase 1: Follicular Phase (Days 1-14) - The Proliferative Phase
Hormonal Trigger
With the demise of the corpus luteum at the end of the previous cycle, estrogen, progesterone, and inhibin A all fall. This removes negative feedback on the pituitary, allowing FSH levels to rise and recruit a cohort of primordial/primary follicles.
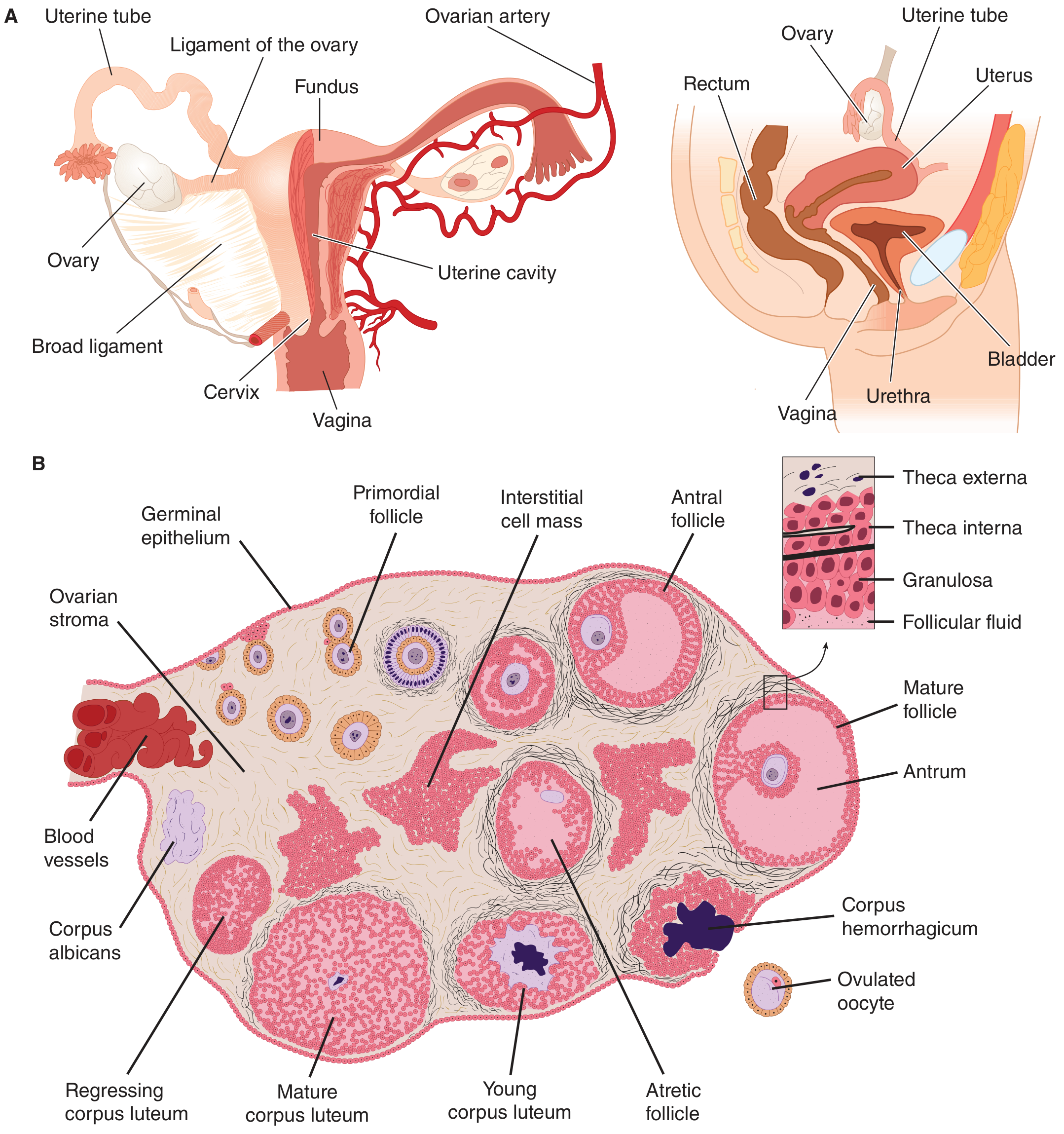
Follicular Development (Ovarian Events)
At birth, both ovaries contain ~6-7 million primordial follicles; by puberty this falls to ~400,000. Each cycle, FSH recruits a cohort of antral follicles that begin to grow.
Two-Cell, Two-Gonadotropin Theory - the key mechanism of estrogen production:
- Theca cells (stimulated by LH) produce androgens (mainly androstenedione)
- These androgens diffuse into granulosa cells (stimulated by FSH), where aromatase converts them to estradiol (E2)
- This synergistic relationship is essential for follicular estrogen production
As estradiol rises, it suppresses FSH (negative feedback). The dominant follicle "wins" because it has accumulated the most FSH receptors and is most sensitive to declining FSH levels. All other follicles in the cohort undergo atresia (via apoptosis). By ~day 6-8, one dominant (Graafian) follicle has been selected.
Rising inhibin B from granulosa cells further suppresses FSH secretion from the pituitary.
Endometrial Events (Uterine Proliferative Phase)
Rising estradiol stimulates the endometrium:
- Proliferation of endometrial glands and stroma
- Growth and elongation of spiral arteries
- Cervical mucus becomes copious, watery, elastic, and forms a "ferning" pattern on a glass slide - channels form that allow sperm penetration
The superficial two-thirds of the endometrium (the decidua functionalis) proliferates. The deep third (decidua basalis) does not proliferate but serves as the source of regeneration after menses.
Ovulation (Day 14)
Just before ovulation, estradiol reaches a sustained peak. This triggers a switch from negative to positive feedback on the pituitary:
- The LH surge (and a smaller FSH surge) is triggered - this is the proximate cause of ovulation
- The LH surge stimulates progesterone production by granulosa cells (via upregulation of LH receptors on granulosa cells during the late follicular phase)
- The small FSH midcycle surge is attributable to this progesterone pulse
The distended follicle ruptures 24-36 hours after the LH surge, releasing the oocyte into the peritoneal cavity. The fimbriated ends of the fallopian tube pick up the oocyte. Minor peritoneal bleeding at this time can cause fleeting lower abdominal pain - mittelschmerz.
At ovulation, cervical mucus peaks in quantity and becomes maximally penetrable by sperm.
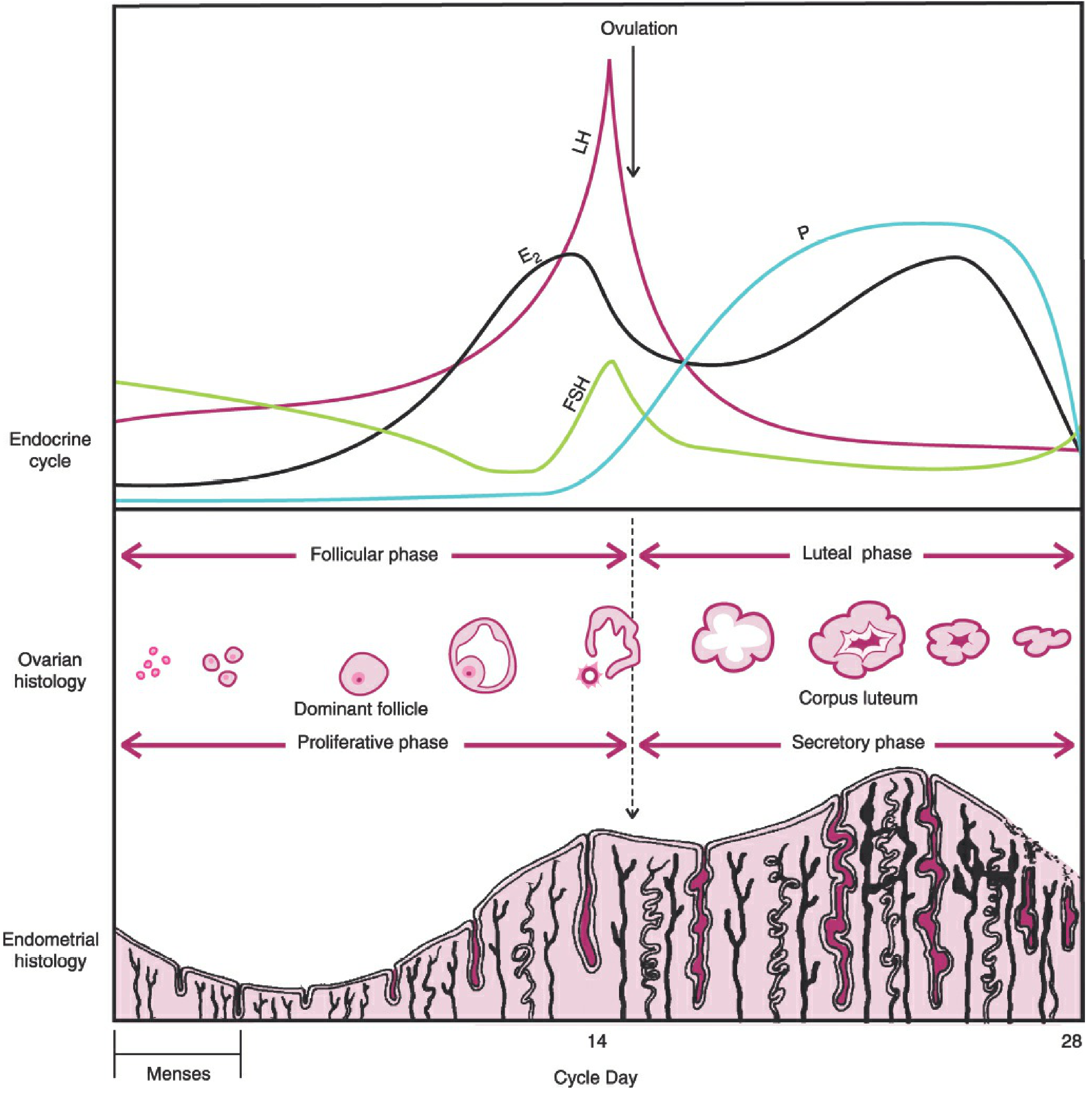
Phase 2: Luteal Phase (Days 14-28) - The Secretory Phase
Corpus Luteum Formation
After ovulation, the ruptured follicle fills with blood - the corpus hemorrhagicum. The granulosa and theca cells rapidly proliferate and accumulate lipid-rich material to form the corpus luteum ("yellow body"). Its development and function depend on an adequate blood supply, mediated by VEGF.
The corpus luteum is the main endocrine organ of the luteal phase. It secretes:
- Progesterone (dominant hormone of this phase)
- Estradiol (rises again in mid-luteal phase)
- Inhibin A
Progesterone levels rise precipitously after ovulation and are used as a presumptive sign that ovulation has occurred.
Endometrial Events (Uterine Secretory Phase)
Under progesterone:
- Endometrial proliferation slows, then halts
- Uterine glands become tortuous, accumulate glycogen in vacuoles, and increase secretions
- Stroma becomes edematous
- Spiral arteries elongate and become tightly coiled
- Cervical mucus becomes thick, scanty, non-elastic, does not fern - inhospitable to sperm
This transformation creates an optimal environment for embryo implantation, which typically occurs days 20-23 of a 28-day cycle (the "window of implantation").
Progesterone's mild thermogenic action raises basal body temperature during the luteal phase - the basis of the rhythm method of contraception (temperature rise is retrospective confirmation of ovulation).
Luteolysis (If No Pregnancy)
The corpus luteum has a fixed lifespan of 12-16 days unless rescued by hCG from a developing embryo. Without continued LH stimulation, it regresses - a process called luteolysis.
Falling progesterone, estrogen, and inhibin A remove negative feedback on FSH, allowing FSH to rise again and begin recruiting the next follicular cohort.
Loss of progesterone support causes endometrial breakdown:
- Spiral artery vasoconstriction and ischemia
- Sloughing of the decidua functionalis
- Menstruation: 2-6 days of flow, average blood loss 20-60 mL
If Pregnancy Occurs
The embryo secretes human chorionic gonadotropin (hCG), which mimics LH and "rescues" the corpus luteum from luteolysis. The corpus luteum continues to produce progesterone until the luteal-placental shift at approximately 5 weeks of gestation, when the developing placenta takes over progesterone production.
Summary of Hormonal Changes Through the Cycle
| Phase | Dominant Hormone | Endometrium | Ovary | Cervical Mucus |
|---|---|---|---|---|
| Menstruation (days 1-5) | Low E2, Low P | Shedding | Follicular recruitment begins | Scanty |
| Follicular (days 5-13) | Estradiol (E2) rises | Proliferates | Dominant follicle develops | Watery, ferning |
| Ovulation (day ~14) | E2 peak → LH surge | Maximal proliferation | Follicle ruptures | Most copious and penetrable |
| Luteal (days 15-28) | Progesterone dominant | Secretory transformation | Corpus luteum active | Thick, non-ferning |
| Late luteal (days 26-28) | All fall | Ischemia/necrosis | Corpus luteum regresses | Scanty |
Key Regulatory Feedback Loops
- Negative feedback (dominant throughout most of cycle): Estrogen + progesterone + inhibin → suppress GnRH, FSH, LH
- Positive feedback (triggers ovulation): Sustained high estrogen → LH surge
- FSH self-limitation: As estrogen and inhibin B rise in the follicular phase, FSH is suppressed - only the dominant follicle (most FSH receptors) survives this
Clinically Relevant Points
- Variability in cycle length is almost entirely due to variability in the follicular phase duration (10-21 days); the luteal phase is nearly constant at 14 days
- Ovulation always occurs 14 days before the next menses - e.g., in a 35-day cycle, ovulation is on day 21
- Inhibin B peaks in the follicular phase; Inhibin A peaks in the luteal phase
- Androgen excess (e.g., PCOS) suppresses FSH and causes chronic anovulation
- A mid-luteal progesterone level >3 ng/mL is a presumptive sign of ovulation
Sources: Berek & Novak's Gynecology, pp. 264-294 | Costanzo Physiology 7th Edition, pp. 479-481 | Ganong's Review of Medical Physiology 26th Edition, pp. 404-406
This is a shared conversation. Sign in to Orris to start your own chat.